The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
The scapula (Latin: scapula) is a flat triangular bone with four major processes (scapular spine, glenoid process, acromion, coracoid process), located in the upper back and forming the posterior part of the shoulder girdle.
The scapula plays a key role in:
darm movement: contributes to rotation and abduction at the shoulder joint (1/3 of the range of motion is scapulothoracic, 2/3 is scapulohumeral);
Thestability of the shoulder: is provided by the shoulder joint itself, as well as the scapulothoracic and acromioclavicular joints and the upper shoulder support complex.
Epidemiology
Scapular fractures are rare injuries, accounting for less than 1% of all fractures and 3–5% of shoulder girdle injuries. They are most commonly found in young men (25–50 years old).
Prevalencebyfracture type:
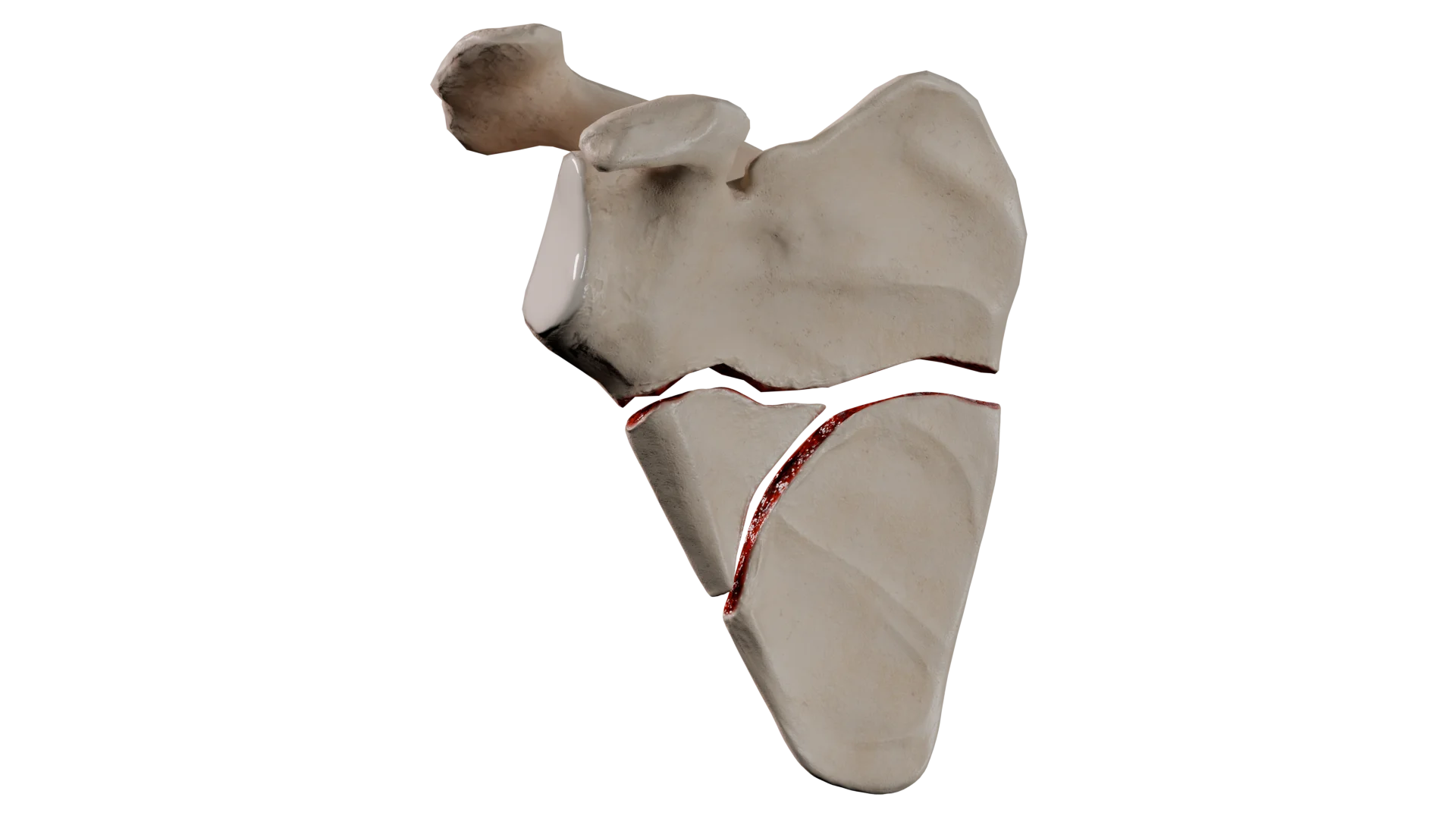
body of the scapula — the most common type, 50–60% of cases;
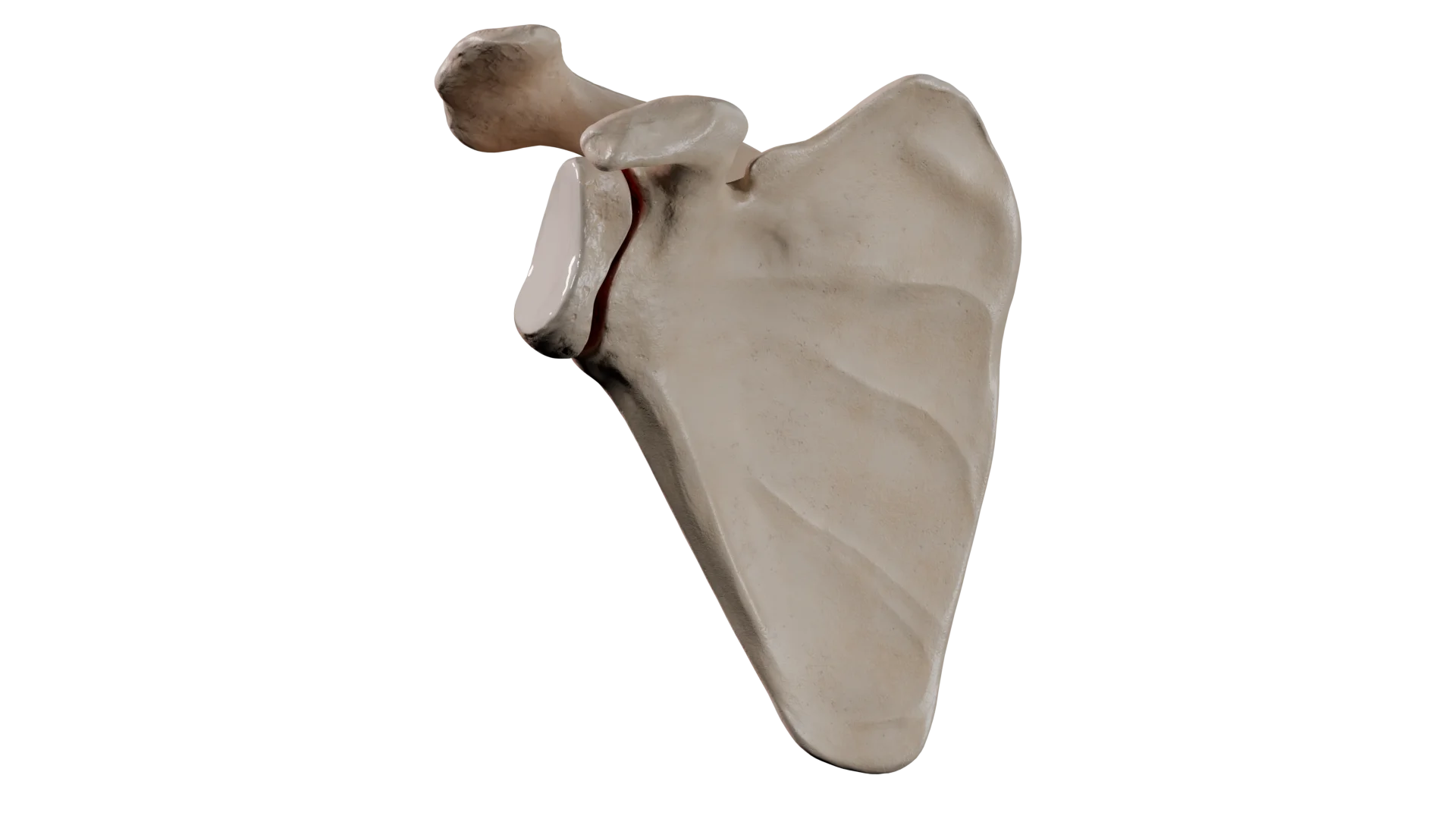
extraarticular glenoid fractures — 20–25%. Often associated with clavicle fractures (“floating shoulder”);
intraarticular glenoid fractures — 10%;
acromial process — about 8%;
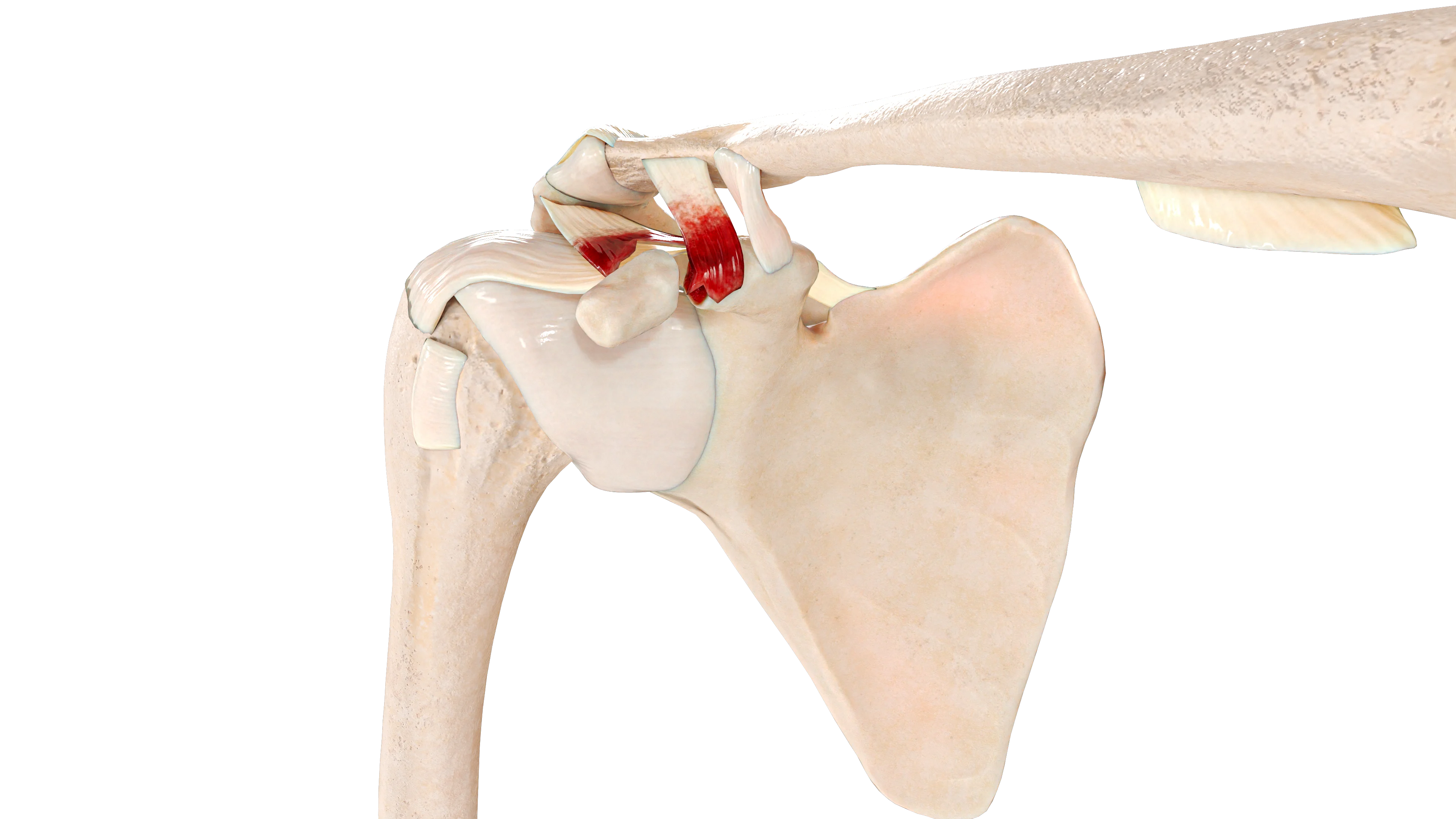
coracoid process — 3–5%;
spine of the scapula — 2–3%.
Due to the high energy impact, scapular fractures are often accompanied by other serious injuries:
chest injuries (80%) — often include lung contusions (40%) and hemo/pneumothorax (more than 30%);
fractures of the pectoral girdle bones (50%), including clavicle (25%);
rib fractures (50%);
head injuries (35–50%);
spinal fractures (25–30%);
pelvic fractures (15%);
vascular and nerve injuries of the arm (10%).
Etiology
Scapular fractures are almost always the result of high-energy trauma, most often vehicle accidents (80–90%). This is due to the bone being well protected by the surrounding muscles.
Primary mechanisms of injury:
Direct trauma: a strong blow directly to the shoulder.
Indirect trauma: transfer of force through the arm (e.g., fall on outstretched hand — FOOSH).
Fracture mechanisms for different parts of the scapula:
body of the scapula: result of direct blow, fall or compression;
glenoid neck: result of indirect trauma, most commonly a fall on outstretched hand;
intraarticular glenoid fractures: usually occur during anterior shoulder dislocation (less frequently posterior, for example, due to electrical shock or seizure);
acromial process: result of direct trauma; stress fractures may also occur in athletes;
coracoid process: may be caused by direct trauma, sudden muscle contraction, or ligament tension during shoulder dislocation;
spine of the scapula: result of direct trauma; in rare cases, may be a pathological fracture due to tumor metastasis.
Classification of scapular fractures
Scapular fractures are classified primarily by anatomical location. Additionally, the presence of fragments and the shape of the fracture line are considered in accordance with standard terminology. Below are the most commonly used classifications.
Hardegger classification
This is the simplest and most commonly used classification, based on the localization of the fracture (Hardegger classification).
Anatomical classification of scapular fractures according to Hardegger
Fracture of the neck of the scapular articular process (14F0 according to AO/OTA classification)
Intraarticular glenoid fracture (Type IA according to Ideberg classification)
Fracture of the scapular acromial process (Type II according to Kuhn classification)
Fracture of the scapular coracoid process (Type I according to Ogawa classification; Type II according to Eyres classification)
Classification of glenoid fractures according to Ideberg
For glenoid cavity fractures, the Ideberg classification (1984) includes six types:
Type I: fracture of the rim of the glenoid cavity:
Subtype IA — fracture of the anterior rim (bony Bankart type);
Subtype IB — fracture of the posterior rim.
Type II: transverse fracture across the glenoid cavity extending to the neck of the scapula. In this type of fracture, the shoulder joint is unstable.
Type III: rare oblique fracture through the upper portion of the cavity extending to the scapular body.
Type IV: transverse fracture reaching the medial border of the scapula. It results from high-energy impact.
Type V: combined fracture, representing a combination of several types (II and IV, III and IV, or II, III, and IV), divided into subtypes A, B, C. This fracture is extremely unstable.
Type VI: severe comminuted damage to the entire articular process.
Classification of acromion fractures according to Kuhn
Fractures of the scapular acromial process are classified according to Kuhn (Kuhn classification). The classification identifies three fracture types, and based on the type, determines the treatment strategy:
Type I: fracture with minimal displacement, not requiring surgical intervention.
Type II: displaced fracture without narrowing of the subacromial space. For this type of fracture, both surgical and conservative treatment are possible.
Type III: displaced fracture with narrowing of the subacromial space. This type of fracture requires surgical treatment.
Classification of coracoid process fractures
There are two main classifications for fractures in this area.
Ogawa classification
This classification (Ogawa classification) is based on the relation of the fracture line to the attachment site of the coracoclavicular ligaments:
Type I: fracture line is located proximal to the attachment site (base fracture).
Type II: the fracture line runs distal to the attachment of the coracoclavicular ligaments.
Such a division is justified from clinical and functional perspectives. Typically, a Type I fracture is associated with instability of the Superior Shoulder Suspensor Complex (SSSC).
Eyres Classification
The classification proposed by Eyres (Eyres’ anatomical classification) includes 5 fracture types:
Type I: fracture of the tip of the process.
Type II: fracture of the middle segment of the process.
Type III: fracture of the base of the process.
Type IV: fracture involving the upper part of the scapular body.
Type V: fracture extending into the area of the glenoid cavity of the scapula.
Comprehensive AO/OTA classification
It is a comprehensive and standardized classification of scapular fractures.
Diagnosis of scapular fractures
The diagnosis of scapular fractures relies on clinical assessment and radiological imaging techniques.
Clinical Evaluation
History — high-energy trauma or direct blow.
Examination — swelling, bruising, abrasions in the scapular area.
Palpation — local tenderness or step-off felt beneath the skin.
Evaluation of accompanying injuries — check for chest, pelvis, head, and spinal traumas or vascular and nerve injuries.
Radiologic Methods
X-ray — standard anteroposterior, lateral (Y-view), and axillary views.
Computed tomography (CT) — provides detailed information, particularly for intra-articular or complex fractures, and aids in preoperative planning.
Clinical Manifestations
Typical clinical presentation in scapular fracture:
Symptoms — acute pain in the shoulder or upper back, swelling, and restricted shoulder mobility.
Physical findings — visible swelling, tenderness, crepitus (crackling) over the scapula, sometimes deformity.
Manifestations of concomitant injuries.
Treatment of scapular fractures
Thanks to the scapula’s sturdy structure and its protection by surrounding muscles and the rib cage, many fractures are characterized by minimal displacement and are amenable to conservative treatment. Fractures affecting the glenoid cavity that are significantly displaced and unstable typically require surgical treatment.
Medical therapy
Conservative treatment is indicated in most fractures of the scapular body, spine, acromial and coracoid processes without significant displacement. Intra-articular fractures of the glenoid cavity with less than 2 mm displacement and no shoulder joint instability can also be treated conservatively.
3D animation — comminuted fracture of the scapular body
3D animation — fracture of the neck of the glenoid process of the scapula
Treatment involves immobilization with a bandage for a period of 2–4 weeks. To prevent the development of adhesive capsulitis, early passive movements are recommended from the second week after injury (controlled by pain). Active movements are permitted no earlier than 4 weeks post-injury. Healing is generally achieved within 6–12 weeks and depends on the severity of the injury.
Surgical Therapy
Surgical treatment is applied in 10–20% of cases. Indications for surgery depend on the fracture location and degree of displacement.
Indications for surgical treatment of scapular fractures based on location
Open reduction and internal fixation (ORIF) using plates and screws.
Arthroscopic fixation with sutures and screws for small fragments of the glenoid cavity.
Early surgical treatment can improve functional outcomes in appropriately selected patients.
Prognosis for scapular fracture
Scapular fractures generally have a high likelihood of union due to good blood supply and surrounding soft tissues. In the majority of patients, shoulder function is restored in full. In cases of extensive soft tissue injury, pain syndrome may persist for a long time.
Therefore, fractures of the scapular body have an excellent prognosis. A good prognosis is assumed for fractures of the acromial and coracoid processes. Fractures of the glenoid neck are generally prognostically favorable, but improper union can reduce shoulder strength and stability. Intra-articular glenoid fractures have an ambiguous prognosis. The outcome of the fracture may result in post-traumatic osteoarthritis of the glenohumeral joint, joint instability, limitation of movement in the injured joint.
Timely diagnosis, comprehensive treatment of accompanying injuries, and adherence to rehabilitation programs by the patient are the key to achieving optimal results.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Rehabilitation after scapular fracture
Although the fracture consolidation process is favorable, the restoration of full function of the glenohumeral joint largely depends on a structured and phased rehabilitation program.
Rehabilitation goals:
restoration of the range of motion in the glenohumeral joint;
restoration of muscle tone;
return to work and sports activities.
Principles of structured and sequential rehabilitation:
initial immobilization for stabilization and fracture healing;
early mobilization;
elimination of the consequences of soft tissue injuries;
progressive load.
Phases of Rehabilitation
The recovery program can be divided into four consecutive stages:
pThe first stage (up to 2–3 weeks)— immobilization of the injured limb is indicated. At this time, active movements in unaffected joints (wrist, elbow) are permitted;
Theearly mobilization phase (3–6 weeks) — early passive movements in the shoulder joint and isometric (static) exercises for the muscles of the shoulder girdle are indicated;
phase of functional recovery (6–12 weeks) — work begins on restoring the full range of active motion. Progressive loading for the muscles using weights and expanders is introduced while avoiding forced movements;
Return to full activity (12+ weeks) — involves fully restoring lost endurance and strength through strength training, plyometric exercises, and practicing specific movements for a particular type of activity.
Expected restoration of the full range of motion is projected to be at 3–4 months post-injury. Symmetrical strength compared to the uninjured limb is generally restored by 4–6 months post-injury with completed rehabilitation measures. Return to non-contact sports is permitted after 3–4 months post-injury. Participation in contact sports is allowed no sooner than 6 months.
FAQ
1. What are the dangers of a scapula fracture?
The primary dangers of a scapula fracture include a high likelihood of damage to thoracic organs, major vessels, and nerves by bone fragments, as well as persistent dysfunction of the affected upper extremity.
2. What associated injuries are most commonly linked with scapula fractures?
Since a scapula fracture results from high-energy trauma, it is often accompanied by other injuries. The most common are thoracic injuries in the form of rib fractures with accompanying complications (pneumo/hemothorax, lung contusion) occurring in 80% of cases, as well as clavicle fractures and brachial plexus injuries diagnosed in approximately 25% of cases.
3. When is standard radiography insufficient, necessitating the use of CT?
Computed tomography is required when there is a suspicion of an intra-articular or complex comminuted fracture. CT provides detailed information on the degree of fragment displacement and is a key study for accurate preoperative planning.
4. How long does it take for a scapula fracture to heal?
The healing process (consolidation) of a scapula fracture typically takes 6 to 12 weeks. The duration depends on the severity of the injury and the presence of associated injuries. Complete functional recovery, including muscle strength, may take 4 to 6 months.
5. What are the main criteria for deciding on surgical therapy?
Surgical therapy is indicated for significant limb instability or fragment displacement. Key criteria include displacement of the glenoid articular fragments by more than 2–4 mm, displacement of the scapular body by more than 20 mm, angular deformity over 40°, and the “floating shoulder” condition with a concomitant clavicle fracture.
6. Which type of scapula fracture has the most uncertain prognosis?
Intra-articular glenoid (joint cavity) fractures have the most uncertain prognosis. Such injuries may result in the development of post-traumatic osteoarthritis of the glenohumeral joint, chronic instability, or persistent limitation of the range of motion.
7. What are the recommended durations for immobilization and initiation of movements?
Immobilization of the limb is indicated for a period of 2 to 4 weeks. To prevent the development of glenohumeral joint stiffness, early passive movements are recommended to start from the second week, while active movements are allowed no earlier than 4 weeks post-injury.
8. When can a patient return to sports activities?
Returning to non-contact sports is possible 3–4 months after the injury. Engaging in contact sports that require full strength exertion is permissible no sooner than 6 months, provided successful rehabilitation.
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Lin IH, Lin TL, Chang HW, Lin CY, Tsai CH, Lo CS, Chen HY, Chen YW, Hsu CJ. Arthroscopy-Assisted Reduction and Internal Fixation versus Open Reduction and Internal Fixation for Glenoid Fracture with Scapular Involvement: A Retrospective Cohort Study. J Clin Med. 2022 Feb 21;11(4):1131.
3.
Sharifpour S, Mirghaderi P, Ghaseminejad Raeini A, Mirghaderi R, Moharrami A, Kalantar SH. Management of a floating shoulder accompanied by a scapular surgical neck fracture: a case report and review of the literature. Ann Med Surg (Lond). 2023 Mar 27;85(4):960-964.
4.
Matsuo T, Yoshikawa K, Oki S, Takeuchi D. Reconstruction surgery of intra-articular scapular fracture nonunion: a case report and literature review. JSES Rev Rep Tech. 2021 Oct 14;2(1):68-74.
5.
Berritto D, Pinto A, Russo A, Urraro F, Laporta A, Belfiore MP, Grassi R. Scapular fractures: a common diagnostic pitfall. Acta Biomed. 2018 Jan 19;89(1-S):102-110.
6.
Chen X, Deng YD, Qiu XS, Chen YX, Zhang ZT. Analysis of the curative effect and prognostic factors in patients with scapular fracture with surgical indications after conservative treatment: a case series and clinical outcomes. Quant Imaging Med Surg. 2023 Aug 1;13(8):5130-5140.
7.
Ogawa K, Inokuchi W, Honma T. Overlooked Fracture of the Inferior Scapular Angle Treated Conservatively. Case Rep Orthop. 2019 Jan 10;2019:9640301.
8.
Hefny AF, Mansour NA, Hefny MA, Masuadi E, Al Bahri S, Elkamhawy AA, Saber KS. Significance of Scapular Fracture Existence in Blunt Chest Trauma: A Retrospective Cohort Study. Surg Res Pract. 2024 May 20;2024:3550087.
9.
Chen L, Liu CL, Wu P. Fracture of the scapular neck combined with rotator cuff tear: A case report. World J Clin Cases. 2020 Dec 26;8(24):6450-6455.
10.
Neral M, Knapik DM, Wetzel RJ, Salata MJ, Voos JE. Scapular Body Fracture in the Athlete: A Systematic Review. HSS J. 2018 Oct;14(3):328-332.
11.
Chouhan V, Ladhania M, Vatsa A. Bilateral Scapular Fracture due to an Epileptic Seizure: A Case Report. J Orthop Case Rep. 2023 May;13(5):64-67.
12.
Ogawa K, Matsumura N, Yoshida A, Inokuchi W. Fractures of the coracoid process: a systematic review. JSES Rev Rep Tech. 2021 May 12;1(3):171-178.
St. Petersburg FL 33702, 7901 4th St N STE 300, USA
Thank you!
Your message is sent! Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io
Cookie Consent
We use cookies to enhance your browsing experience, analyze site traffic, and deliver content. Please choose whether you accept all cookies or wish to reject non-essential tracking.
Cookie Preferences
Manage your cookie preferences below:
Essential cookies enable basic functions and are necessary for the proper function of the website.
Name
Description
Duration
Geolocation Config
This cookie is used to store the consent settings based on the visitor's location.
30 days
Cookie Preferences
This cookie is used to store the user's cookie consent preferences.
30 days
Google reCAPTCHA helps protect websites from spam and abuse by verifying user interactions through challenges.
Name
Description
Duration
_GRECAPTCHA
Google reCAPTCHA sets a necessary cookie (_GRECAPTCHA) when executed for the purpose of providing its risk analysis.
179 days
Statistics cookies collect information anonymously. This information helps us understand how visitors use our website.
Google Analytics is a powerful tool that tracks and analyzes website traffic for informed marketing decisions.
ID used to identify users for 24 hours after last activity
24 hours
_gat
Used to monitor number of Google Analytics server requests when using Google Tag Manager
1 minute
_gac_
Contains information related to marketing campaigns of the user. These are shared with Google AdWords / Google Ads when the Google Ads and Google Analytics accounts are linked together.
90 days
__utma
ID used to identify users and sessions
2 years after last activity
__utmt
Used to monitor number of Google Analytics server requests
10 minutes
__utmb
Used to distinguish new sessions and visits. This cookie is set when the GA.js javascript library is loaded and there is no existing __utmb cookie. The cookie is updated every time data is sent to the Google Analytics server.
30 minutes after last activity
__utmc
Used only with old Urchin versions of Google Analytics and not with GA.js. Was used to distinguish between new sessions and visits at the end of a session.
End of session (browser)
__utmz
Contains information about the traffic source or campaign that directed user to the website. The cookie is set when the GA.js javascript is loaded and updated when data is sent to the Google Anaytics server
6 months after last activity
__utmv
Contains custom information set by the web developer via the _setCustomVar method in Google Analytics. This cookie is updated every time new data is sent to the Google Analytics server.
2 years after last activity
__utmx
Used to determine whether a user is included in an A / B or Multivariate test.
18 months
_ga
ID used to identify users
2 years
_gali
Used by Google Analytics to determine which links on a page are being clicked
30 seconds
Clarity is a web analytics service that tracks and reports website traffic.