External Ear Injuries: Symptoms, Diagnosis, and Treatment
Danata A.Otorhinolaryngologist, MD
15 min read·April 14, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
External ear injuries include mechanical damage to the auricle and external auditory canal. These conditions vary by depth of lesion, etiology, and mechanism of injury.
Superficial and deep injuries of the auricle occur due to mechanical impact (trauma, blows, falls, bites, car accidents).
Injuries to the auditory canal often occur during attempts at self-cleaning of earwax or the entry of foreign objects.
The extent of damage depends on the force of impact and the nature of the injury. Burns and frostbites occur due to thermal damaging factors (fire, cold).
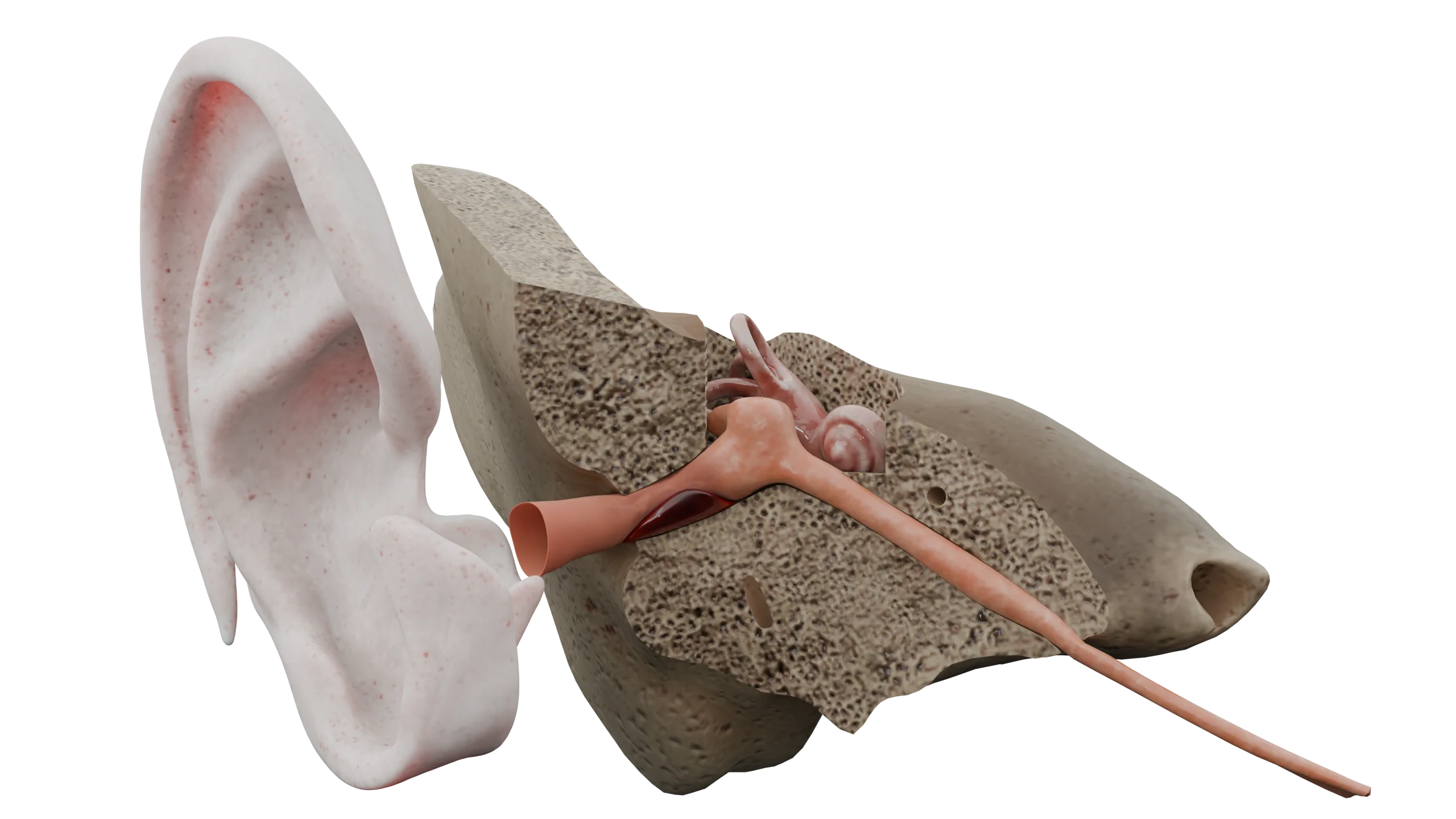
Anatomy of External Ear Injuries
Mechanical and thermal factors impact the auricle, causing tissue damage of varying depths.
Othematoma occurs after blunt trauma with significant force. In this situation, the walls of the vessels located between the cartilage and the perichondrium rupture, forming a limited blood accumulation that deforms the outer appearance of the auricle. The auricle itself gains a bluish tint and swells.
A contusion occurs with less severe blunt trauma. It is characterized by concussion of the soft tissues. Smaller vessels are more severely damaged, skin integrity is not compromised, and hyperemia and infiltration of the auricle is noted.
Auricular and external acoustic meatus abrasions are characterized by partial damage to the epidermis. They quickly become covered with hemorrhagic crusts, and slight bleeding may occur.
A hematoma of the auditory canal is characterized by damage to the subcutaneous vessels. This results in localized blood accumulation that protrudes and narrows the canal’s lumen, with varying degrees of compromise. The skin at the hematoma site becomes cyanotic.
Deep injuries of the auricle occur from various causes: sports and household injuries, workplace incidents (improper handling of tools), animal or human bites, falls, as well as careless wearing of piercings.
Auricular avulsions in daily life are rare; they typically occur due to traffic accidents, combat sports (e.g., boxing), or street fights. This type of injury is characterized by compromised skin integrity, damage to the underlying tissues, subcutaneous fat, vessels, sometimes cartilage, as well as pronounced bleeding and swelling.
Burns occur under extreme high temperatures, open flames, hot objects, and substances.
A first-degree burn is characterized by superficial epidermis damage, the skin becomes locally hyperemic.
In second-degree burns, all epidermal layers are damaged, resulting in a hyperemic and infiltrated skin appearance with blisters filled with serous or hemorrhagic fluid.
Third-degree burns are characterized by necrosis of all skin layers and subcutaneous fat, leading to deep wounds and blisters containing hemorrhagic fluid.
Fourth-degree burns result in total necrosis with involvement of underlying tissues, bones, and cartilage.
Auricular burns may also damage the external auditory canal.
3D animation – burn of the auricle
Auricular frostbites frequently happen in extremely low temperatures, as the auricles are among the body’s most protruding parts.
First-degree frostbite affects superficial skin layers, causing paleness and mottling of the auricle with hyperemia of peripheral and protruding areas.
Second-degree frostbite also affects the superficial skin layers, and serous blisters may appear against a hyperemic background.
Third-degree frostbite results in necrosis of the entire skin layer. The auricle becomes hyperemic, infiltrated, and blisters are filled with serous-hemorrhagic content. Sensitivity of the auricle is absent.
Fourth-degree frostbite is characterized by the involvement of the full thickness of the skin, subcutaneous fat, and underlying tissues (bones, cartilage). The skin becomes vividly hyperemic, cyanotic, and dry gangrene develops in the distal areas. Sensitivity is also absent.
Clinical manifestations
With superficial ear injuries, acute pain occurs at the moment of trauma, with subsequent discomfort and dull pain. The auricle swells, changes color, and then gradually returns to its normal appearance during recovery. When abrasions compromise the skin integrity, scant bleeding occurs; later, they become covered with hemorrhagic crusts and heal under a scab.
Othematoma is characterized by pronounced pain and alteration in the appearance of the auricle. It protrudes, fluctuates at the site of effusion, more often on the outer surface, in the area of the scaphoid and triangular fossae. The skin acquires a cyanotic color. Without appropriate treatment and drainage of the hematoma, the auricle often becomes misshapen due to cartilage transformation resembling ‘cauliflower ear’ or ‘boxer’s ear’. If a large hematoma occurs in the ear canal, obstructing the lumen, conductive hearing loss may occur.
3D animation – othematoma of the external ear
Deep auricular injuries are characterized by severe tenderness and profuse bleeding. The wound edges gape, revealing underlying tissues, and in some cases, cartilage or bone. The configuration of the wound edges varies depending on the injuring factor, with foreign objects, dirt, and earring remnants possible inside.
Burns of the auricle manifest differently according to the stage, as described above. It’s noteworthy that isolated ear burns are extremely rare, often accompanying injuries to the scalp, face, neck, and other body parts. Severe burn areas can lead to burn disease development. Common symptoms include severe tenderness, although bleeding is absent. In third and fourth-degree burns, the bottom of the wound is painless, and a necrotic scab forms.
Clinical changes in frostbite have also been described earlier. A characteristic feature is the absence of pain during frostbite. Discomfort arises upon warming the affected tissues: itching, burning, significant pain, numbness, or paresthesia may occur.
Diagnosis
For the diagnosis of traumatic injuries to the auricle and external auditory canal, in most cases, collecting the medical history and examination are sufficient. Sometimes an X-ray or CT of the temporal bone and temporomandibular joint is conducted to assess the extent of injury.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Treatment
Treatment of superficial injuries of the external ear
Auricular and acoustic meatus abrasions are treated with antiseptic solutions. If infection occurs, antibiotic ointments may be used. Under the crusts, wounds rapidly epithelize and heal.
Otohematoma needs to be punctured under sterile conditions, drained, and a compression dressing applied, which is sutured to the auricle for large hematomas. Systemic antibacterial drugs are prescribed to prevent secondary infection and development of perichondritis.
Ear canal hematomas are also drained, and the canal is tightly packed with ear tampons that are soaked with antiseptic solutions daily.
Treatment of deep external ear injuries
For deep ear injuries, primary surgical treatment is performed, and the wound edges are sutured. In case of partial avulsion, non-viable tissues are excised as sparingly as possible, and the cartilage, subcutaneous fat, and skin are sutured separately.
For complete auricle avulsions, the viability of the amputated section is assessed. It is recommended that no more than 6 hours pass since the trauma and that the avulsed auricle segment is kept cold. If all necessary conditions are met, replantation is performed, with prescribed antibiotic therapy, thromboembolic prophylaxis, and daily dressings.
Burn treatment
Burns are washed, remnants of burnt clothing and hair are removed, non-viable tissues are excised, then the wounds are treated with antiseptic solutions, cooled, and covered with sterile dressings. Before dressing changes, it is mandatory to adequately anesthetize the patient.
For 2nd and 3rd-degree burns, large blisters are opened and excised; for 3rd and 4th-degree burns, the scab is excised to expose viable tissues. During daily dressings, antimicrobial and wound-healing ointments are used.
To prevent cicatricial stenosis of the external auditory canal, it must be tightly tamponaded with sterile dressings and daily soaked with antiseptic solutions. If bacterial infection occurs, systemic broad-spectrum antibacterial therapy is prescribed based on sensitivity. Patients with 3B or 4th-degree burns or extensive burns are admitted to surgical or burn departments for suitable treatment. Skin grafting is performed later if necessary.
Frostbite treatment
The treatment scheme for frostbite corresponds to that for burns, but initially, the frostbitten body part needs to be warmed. The victim is placed in a warm room and given plenty of warm drinks. The auricle should be gradually rewarmed without harsh methods or rubbing. Sterile warmed solutions of furacilin, saline, warm compresses, and gentle massage with warm clean hands can be used for this purpose.
In case of severe pain, the patient needs adequate analgesia. Damaged tissues are rinsed and treated with antiseptic solutions. If blisters and scabs are present, necrotic tissues are excised and dressings with antimicrobial and wound-healing ointments are applied.
For 3rd and 4th-degree frostbite, systemic antibacterial therapy is prescribed. If indicated, these patients are also admitted to surgical or burn departments. Over time, neuropathy may develop, accompanied by numbness and cold sensitivity.
All patients with wounds, burns, or frostbite receive urgent tetanus immunization; rabies prophylaxis is administered in cases of bites.
FAQ
1. What complications may arise from ear injuries?
•Infections: perichondritis (inflammation of the cartilage), abscesses. •Auricle deformation: “cauliflower ear”. •Conductive hearing loss: due to ear canal damage. •Tissue necrosis: in cases of severe burns or frostbite. •Scarring: narrowing of the ear canal or ear deformation.
2. How can complications after an ear injury be prevented?
To prevent complications after an ear injury, seek medical attention promptly even for minor injuries, follow care recommendations (regularly treat wounds and change dressings), take prescribed medications (antibiotics, anti-inflammatory drugs), avoid re-injury, and refrain from self-treatment, as this could lead to infection or ear deformation.
3. When is surgical intervention necessary?
Surgery is necessary in the following cases: •deep wounds: to suture the damaged tissues; •auricle avulsion: for replantation (reattachment of the avulsed portion); •othematoma: to drain the accumulated blood; •severe burns and frostbite: necrotic tissues need to be removed; •scarring: to correct deformities or narrowing of the ear canal.
4. Is it possible to restore the auricle after injury?
Yes, restoration is possible, but it depends on the severity of the damage: •superficial injuries: the auricle naturally restores itself with proper treatment; •deep injuries and avulsions: surgical intervention is required. If an avulsed portion of the ear is brought to the hospital within 6 hours, successful replantation is possible; •deformities: reconstructive surgery can restore the shape and function of the ear.
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Sclafani AP, Dyleski RA, Pitman MJ, Schantz SP. Total otolaryngology—head and neck surgery. New York: Thieme Medical Publishers; 2015. ISBN: 978-1-60406-646-3.
3.
Behrbohm H, Kaschke O, Nawka T, Swift A. Bolezni ukha, gorla i nosa [Ear, nose, and throat diseases]. 2nd ed. Moscow: MEDpress-inform; 2016. 776 p. [In Russian.] ISBN 978-5-00030-322-1.
4.
Hohman MH, Jamal Z, Krogmann RJ, et al. Auricular Hematoma. [Updated 2024 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-.
Available from: https://www.ncbi.nlm.nih.gov/books/NBK531499/
5.
Trauma Management of the Auricle. Facial Plast Surg. 2015 Aug;31(4):382-5. doi: 10.1055/s-0035-1562882. Epub 2015 Sep 15. PMID: 26372713.
6.
Kraenzlin FS, Mushin OP, Ayazi S, Loree J, Bell DE. Epidemiology and Outcomes of Auricular Burn Injuries. J Burn Care Res. 2018 Apr 20;39(3):326-331. doi: 10.1097/BCR.0000000000000586. PMID: 28557871.
St. Petersburg FL 33702, 7901 4th St N STE 300, USA
Thank you!
Your message is sent! Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io
Cookie Consent
We use cookies to enhance your browsing experience, analyze site traffic, and deliver content. Please choose whether you accept all cookies or wish to reject non-essential tracking.
Cookie Preferences
Manage your cookie preferences below:
Essential cookies enable basic functions and are necessary for the proper function of the website.
Name
Description
Duration
Geolocation Config
This cookie is used to store the consent settings based on the visitor's location.
30 days
Cookie Preferences
This cookie is used to store the user's cookie consent preferences.
30 days
Google reCAPTCHA helps protect websites from spam and abuse by verifying user interactions through challenges.
Name
Description
Duration
_GRECAPTCHA
Google reCAPTCHA sets a necessary cookie (_GRECAPTCHA) when executed for the purpose of providing its risk analysis.
179 days
Statistics cookies collect information anonymously. This information helps us understand how visitors use our website.
Google Analytics is a powerful tool that tracks and analyzes website traffic for informed marketing decisions.
ID used to identify users for 24 hours after last activity
24 hours
_gat
Used to monitor number of Google Analytics server requests when using Google Tag Manager
1 minute
_gac_
Contains information related to marketing campaigns of the user. These are shared with Google AdWords / Google Ads when the Google Ads and Google Analytics accounts are linked together.
90 days
__utma
ID used to identify users and sessions
2 years after last activity
__utmt
Used to monitor number of Google Analytics server requests
10 minutes
__utmb
Used to distinguish new sessions and visits. This cookie is set when the GA.js javascript library is loaded and there is no existing __utmb cookie. The cookie is updated every time data is sent to the Google Analytics server.
30 minutes after last activity
__utmc
Used only with old Urchin versions of Google Analytics and not with GA.js. Was used to distinguish between new sessions and visits at the end of a session.
End of session (browser)
__utmz
Contains information about the traffic source or campaign that directed user to the website. The cookie is set when the GA.js javascript is loaded and updated when data is sent to the Google Anaytics server
6 months after last activity
__utmv
Contains custom information set by the web developer via the _setCustomVar method in Google Analytics. This cookie is updated every time new data is sent to the Google Analytics server.
2 years after last activity
__utmx
Used to determine whether a user is included in an A / B or Multivariate test.
18 months
_ga
ID used to identify users
2 years
_gali
Used by Google Analytics to determine which links on a page are being clicked
30 seconds
Clarity is a web analytics service that tracks and reports website traffic.