Gastric and Duodenal Ulcers (Gastroduodenal Ulcers)
Gastric and Duodenal Ulcers (Gastroduodenal Ulcers): Symptoms, Etiology, Diagnosis, and Treatment
Aleksandr F.Abdominal surgeon, MD
24 min read·June 17, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Gastroduodenal ulcer is a defect in the stomach or duodenal wall, penetrating deeper than the submucosal layer.
In developed countries, this pathology is found in 15% of the adult population. The highest mortality rates are observed in Japan and Portugal, while the lowest rates are seen in the USA and Canada.
Duodenal ulcers occur 5–7 times more frequently than gastric ulcers. The male-to-female ratio is 3–4:1.
Anatomy
Stomach
The stomach is located in the upper part of the abdominal cavity. It is held in position by the fixation of the esophagus and duodenum, as well as ligaments with the liver, pancreas, spleen, and transverse colon. At the transition from the stomach to the duodenum lies the pyloric sphincter.
The stomach wall consists of serous, muscular, submucosal, and mucosal layers. In the muscular layer, fibers are arranged in different directions: longitudinal, oblique, and circular.
The gastric mucosa, 0.5–1.5 mm thick, has a complex structure (forming folds and gastric pits) and composition (mucocytes, tubular glands).
The structure of the gastric glands varies in different parts of the organ:
cardiac region — intermediate, mucoid, and argentaffin cells;
body and fundus — parietal (produce hydrochloric acid), accessory (mucoid, produce mucus), and chief (produce pepsinogen) cells;
pyloric region — glands mainly consist of mucoid and parietal cells.
Endocrine cells are scattered throughout the gastric mucosa. The gastric epithelium undergoes continuous renewal (on average every 3–5 days).
Blood supply to the stomach is provided via the branches of the celiac trunk:
left and right gastric arteries;
left and right gastroepiploic arteries;
short gastric arteries.
Innervation is provided by the vagus nerve and branches of the solar plexus. Three major nerve plexuses are located in the stomach wall:
subserosal;
intermuscular;
submucosal.
Daily, the stomach produces up to 2 liters of gastric juice, which contains proteolytic enzymes and mucus besides hydrochloric acid.
Duodenum
The duodenum (DPC) is a continuation of the stomach. It starts from the pyloric sphincter and ends at the duodenojejunal junction (in the region of the ligament of Treitz).
The wall of the intestine consists of layers:
serous (at sites of mesoperitoneal location);
muscular;
submucosal;
mucosal.
The muscular layer comprises two layers:
outer longitudinal (continuing the gastric layer, ensuring continuity of the peristaltic wave);
inner circular layer.
The mucosa of the duodenum forms villi (up to 40 per mm), covered with enterocytes. The mucosa also contains goblet cells, producing mucin, and endocrine cells (diffusely located).
The duodenum is divided into parts:
superior horizontal (duodenal bulb);
descending;
inferior horizontal;
ascending.
In the descending limb of the duodenum, through the major duodenal papilla (ampulla of Vater), opens:
common bile duct;
main pancreatic duct.
Through the minor duodenal papilla opens the accessory pancreatic duct (Santorini duct).
Blood supply to the duodenum is provided by branches of the superior mesenteric artery:
Giant ulcer at the border of the body and antral section of the stomach
By number
solitary;
multiple.
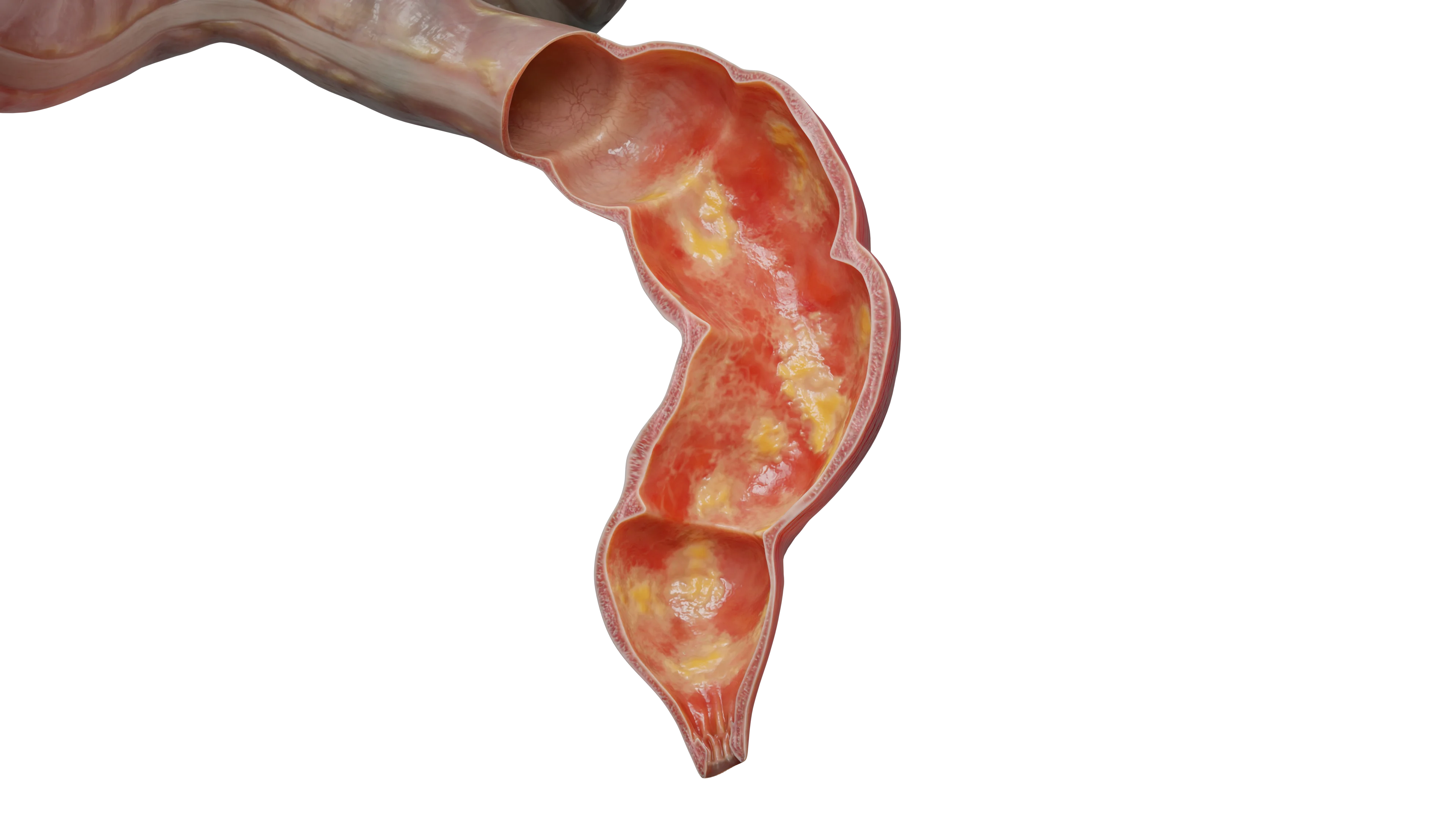
Multiple ulcers of the body and antral section of the stomach – 3D model3D animation – multiple gastric ulcers
Classification A.G. Johnson (1990):
Type I — chronic ulcers of the lesser curvature;
Type II — chronic ulcers combined with duodenal ulcer (including healed duodenal ulcer);
Type III — prepyloric chronic ulcers;
Type IV — acute superficial chronic ulcers;
Type V — chronic ulcers due to Zollinger-Ellison syndrome.
Forrest classification:
Type FI — active bleeding:
Ia – spurting arterial bleeding;
Ib – ooze.
Type FII — signs of recent hemorrhage:
IIa – visible (non-bleeding) vessel;
IIb – adherent clot;
IIc – flat black spot (black ulcer base).
Type FIII — ulcer with clean (white) base.
Factors contributing to peptic ulcer disease
Factors contributing to the development of peptic ulcer disease include:
Heredity: predisposition is predominantly transmitted through the male line; the incidence in first-line heirs is 3 times higher than in individuals without a burdensome heredity.
Alcohol: at high concentrations exerts a direct damaging effect, disrupts the protective mucinous layer, and stimulates gastric glands, thereby increasing hydrochloric acid production.
Smoking: nicotine leads to vasoconstriction of the stomach, stimulates hydrochloric acid production, provokes gastro-duodenal reflux, and reduces bicarbonate secretion (worsening the protective properties of the mucosa).
Dietary aspects: spicy, excessively hot or cold, as well as coarse food capable of physically injuring the walls of the gastrointestinal tract.
Irregular diet: fasting hypersecretion and acid-peptic damage to the mucosa.
Intake of certain medications: non-steroidal anti-inflammatory drugs (NSAIDs), glucocorticosteroids, anticoagulants, aspirin, alendronate.
Prolonged or regular stress: development of stress ulcers.
Etiology of ulcers
In the development of gastro-duodenal ulcers, the main pathogenetic mechanism is the predominance of aggressive factors over the protective properties of the gastric and duodenal mucosa. Over time, this leads to the formation of a mucosal defect, and in the absence of treatment, to the development of complications (the so-called “Shoy scales”).
Aggressive factors include:
Excessive production of hydrochloric acid: increased activity of the gastric parietal cells, hypertonia of the vagus nerve, increased gastrin secretion;
Helicobacter pylori: the microorganism secretes the enzyme mucinase, which disrupts the protective properties of the mucosa; it secretes catalase and urease, which directly lead to the death of epithelial cells. The presence of the bacteria itself in the submucosa causes an inflammatory reaction in the gastric wall;
3D animation – acute gastric ulcer with bleeding
Gastro-duodenal reflux: bile refluxed in this condition along with pancreatic juice destroys the protective lining of the stomach wall and subsequently leads to direct damage to the epithelial cells;
Hypergastrinemia (Zollinger-Ellison syndrome);
Cytomegalovirus infection;
Radiation and chemotherapy;
Crohn’s disease.
Protective factors include:
Mucous (mucinous) barrier: located directly on the mucosal layer and closely associated with it. Consists of mucopolysaccharides and glycoproteins, preventing the penetration of aggressive factors to epithelial cells;
Constant high-active epithelial regeneration: as noted above, gastric mucosal cells are renewed every 3–5 days, which promotes the rapid repair of mucosal damage.
Clinical Manifestations
Pain syndrome. Localized in the upper abdomen: in the epigastrium on the right — with duodenal or pyloric ulcer; in the epigastrium on the left or behind the sternum — with cardiac ulcer; with post-bulbar ulcer, the pain radiates to the back. The pain is caused by both direct irritation of nerve endings by acidic contents and spasm of the muscle layers of the stomach wall. For gastric ulcers, “hungry” pain is characteristic, which is relieved after eating or taking an antacid.
Heartburn. Manifests as burning behind the sternum due to reflux of acidic gastric contents into the esophagus. This reflux is caused by impaired gastric motility due to the irritating effect of the ulcer on the muscle wall of the organ.
Nausea and vomiting. Occur against the background of reflex irritation and contraction of the stomach. They may also result from the development of gastric outlet obstruction.
Decrease or absence of appetite (reflex origin).
Tenderness on abdominal palpation. Detected at the site of the ulcer projection, where muscle guarding of the anterior abdominal wall may also be noted. During abdominal percussion at the site of the ulcer projection, Mendel’s sign — tenderness on percussion — may be found.
It should be noted that asymptomatic progression of peptic ulcer disease is possible (according to several authors, up to 30% of cases).
Diagnosis of gastric and duodenal ulcer disease
Gastric secretion examination (basal and maximal acid output). Maximal acid output is determined after stimulation of gastric secretion (histamine, pentagastrin).
pH-metry. Normally, gastric juice acidity is 1.6–2.0. For a duodenal ulcer, increased acidity in the pyloric canal and DPC is characteristic.
Diagnosis of Helicobacter infection (breath test, blood test, stool test).
X-ray — the main diagnostic method in confirming perforated ulcer — detection of free air under the diaphragm.
Fluoroscopy. Main symptom — “niche” symptom: when the ulcer crater is filled with contrast, a characteristic indentation (“niche”) appears. Symptom of fold convergence — radially arranged stomach folds with an ulcer located in the center. Disturbed gastric peristalsis, retrograde food flow into the esophagus is also often detected. This method is most effective in diagnosing impaired evacuatory function and the development of gastric outlet obstruction. For diagnosing duodenal pathology, relaxation duodenoscopy is used (before the study, maximal relaxation and dilation of the intestinal muscles with metacin, aeronas, etc. are achieved) for complete filling of all sections and visualization of its contours.
Endoscopic study (FEGDS) — the gold standard of diagnostics at the current stage. The method allows:
to visualize the ulcer defect;
to determine the stage of the process and the localization of the ulcer;
to detect the presence of complications;
to perform a biopsy;
to diagnose Helicobacter infection;
to carry out endoscopic manipulations in complications (hemostasis, clipping of defects, argon plasma coagulation, endosutures).
Ultrasound. At the current level of development of this technology, it is possible to identify an ulcerative infiltrate and defect of the gastric wall, the presence of peptic ulcer complications (stenosis, perforation, cancer).
CT of the ABD — combines the advantages of fluoroscopy and ultrasound. It is possible to diagnose both the ulcer defect itself and the development of complications (perforation, stenosis, penetration, cancer).
Complications and treatment of gastric and duodenal peptic ulcer disease
Perforation (perforation)
According to various sources, this complication accounts for 3 to 30% of all complications in gastroduodenal ulcers. Among the patients, 95% are men.
Pyloroduodenal ulcers occur in 75% of cases. The combination of perforated ulcers and bleeding reaches 10%.
Three stages are distinguished in the clinical picture of a perforated ulcer:
first 4–6 hours — primary abdominal shock;
6–12 hours — period of apparent well-being;
more than 12 hours — peritonitis stage.
In case of perforation, the pain is acute and sudden (“stabbing pain”). In the initial hours, it is localized in the upper abdomen and then spreads to the right lateral canal and further throughout the abdomen.
In the first hours from the moment of perforation, the following are observed:
bradycardia (due to stimulation of the vagus nerve);
dryness of the tongue;
Frienic syndrome may occur (irradiation of pain to the right clavicle and scapula due to stimulation of the right phrenic nerve);
liver dullness on percussion may be absent (due to free gas in the abdominal cavity);
pain on rectal examination (Kühn’s symptom).
As noted above, free gas is detected on X-ray (in 70–80% of cases). For diagnosis clarification, it is possible to perform EGD, and if doubts about the presence of perforation persist, repeat radiography to identify free gas (in this case, the diagnostic value of the method is higher).
With the further progression of the disease, symptoms of intoxication and peritonitis become predominant:
tachycardia;
decrease in blood pressure;
abdominal distension;
intestinal paresis;
increasing leukocytosis.
Atypical forms of perforation (up to 4–6% of cases) include:
perforation of the posterior gastric wall (into the omental bursa);
perforation of the posterior duodenal wall (into the retroperitoneal tissue);
perforation of high ulcers of the cardia at the esophagus border;
covered perforations.
In these cases, the course of the clinical picture is blurred, without prominent main symptoms. The treatment of perforated ulcers is exclusively surgical (suturing of the ulcer, resection of the stomach).
Most often, ulcer sutures are performed:
simple suturing with interrupted stitches;
suturing by tamponade with an omentum according to Oppel — Polikarpov (performed in the presence of a large perforative opening and inability to resect);
excision of the ulcer with pyloroduodenoplasty.
Indications for gastric resection are:
callous ulcer;
gastric ulcers;
perforation of multiple ulcers;
combination of perforation and stenosis of the gastric outlet.
The most applicable types of resections are:
resection according to Billroth I and II (modified by Hofmeister — Finsterer);
Roux-en-Y resection;
Balfour resection.
After surgical treatment of a perforated ulcer, completing a full course of antiulcer therapy is mandatory.
Bleeding
This complication develops in 10–15% of patients. Men comprise up to 70%. Duodenal ulcers occur in up to 80% of cases. The mortality rate for this pathology reaches 7–10%.
Bleeding develops in case of erosion (destruction) of the large vessel wall at the base of the ulcer as the disease progresses. The severity of the clinical picture is characterized by the volume of blood loss — from mild (less than 20% of circulating blood volume) to severe (over 40% of CBV).
3D animation – bulbous duodenal ulcer complicated by penetration and bleeding
The variability of clinical manifestations depends on the severity of bleeding:
Of the symptoms of this complication, the following are most often encountered:
vomiting — vomiting of blood (hematemesis) or coffee ground vomiting (the brown-black color of vomitus is due to hematin, formed by the oxidation of hemoglobin by gastric hydrochloric acid);
tarry stool (melena) — stool of black-maroon color, unformed consistency; such a color is acquired as a result of the effects of digestive enzymes and microorganisms on hemoglobin, followed by degradation and color change of the spilled blood.
Bergman’s symptom is characterized by the alleviation of ulcerative pain at the onset of a bleeding episode.
The gold standard for diagnosis is EGD. The pathology requires mandatory hospitalization in a surgical department.
In cases of moderate and severe blood loss, patients are transported to the operating room, where all diagnostic manipulations and intensive therapy are carried out.
Conservative therapy includes:
fresh frozen plasma;
cryoprecipitate or platelet concentrate;
activators of thromboplastin formation (ethamsylate);
During ongoing treatment, emergency EGD is performed to specify the ulcer’s location and perform endoscopic hemostasis.
If the measures are ineffective and bleeding continues, surgical intervention is performed. The type of surgery is determined by the location and nature of the ulcer, as well as the patient’s condition.
The most pathogenetically justified intervention is the resection of 2/3 of the stomach (eliminating the ulcer and hypersecretion of hydrochloric acid). However, due to the severity of the condition, age, and comorbidity, not all patients can withstand such an intervention; in these situations, a reduced volume of intervention is performed:
excision of the ulcer with stomach or duodenal plastic surgery;
in cases of extreme severity, the patient is limited to suturing the ulcer defect to stop the bleeding.
Gastrointestinal tract obstruction
Gastrointestinal tract obstruction (stenosis of the gastric outlet, pyloroduodenal stenosis) can be compensated, subcompensated, and decompensated.
This complication can be of a:
temporary nature (during ulcer exacerbation due to edema and tissue infiltration with the development of intestinal lumen narrowing);
permanent nature (due to cicatricial deformity after healed ulcers).
With impaired gastric emptying, the stomach dilates and increases in volume, food stagnates in it, and regurgitation of contents occurs. Due to the described pathogenesis, the main clinical picture of the disease develops:
belching with a putrid smell;
vomiting of previously eaten “stale” food (provides relief);
periodic pain in the upper abdomen and sensation of stomach fullness even after a small meal;
progressive weight loss (due to the lack of nutrient entry into the intestines);
constipation.
With further disease progression and lack of treatment, electrolyte disturbances increase, which may lead to:
neurological disorders;
muscle dysfunction;
hypochloremic coma.
The gold standard for diagnosing this pathology is fluoroscopy. It allows for the determination of the degree of stenosis.
When performing EGD, stenosis can also be detected, however, determining the degree of compensation is extremely difficult; it can only be assessed indirectly by the passability of the narrowing for the endoscope:
normally the diameter is 2.5 cm;
in compensated stenosis — 1.5 cm;
in the subcompensated stage — 0.5–1.5 cm;
in decompensation — less than 0.5 cm.
Treatment in the initial stages is conservative with the aim of differentiating transient and cicatricial narrowing. During the course of conservative treatment over 7–10 days, healing of the ulcer defect and resolution of the inflammatory reaction occur, restoring patency of the gastric outlet in the case of temporary stenosis, whereas no improvement occurs in organic scar narrowing.
In persistent stenosis, treatment is exclusively surgical. After preoperative preparation for correcting electrolyte and protein imbalances, gastrectomy is performed (often in an extent of 2/3).
3D animation – chronic duodenal ulcer with the formation of decompensated stenosis
Ulcer penetration
Ulcer penetration is the penetration of the base of the ulcer defect into adjacent organs (hepatoduodenal ligament, liver, pancreas, less commonly — mesentery, wall of the colon, gallbladder, lesser omentum).
The main distinguishing feature of this complication in the clinical picture is the change in the character of the pain syndrome: the pain becomes localized and persistent regardless of food intake.
The clinical picture of the affected organ in which penetration occurred may appear:
pancreatitis;
cholecystitis;
reactive hepatitis;
mechanical jaundice;
omentum;
the formation of inflammatory infiltrates of the abdominal cavity.
Diagnosis is performed using the methods described above:
EGD — a deep ulcer with undermined edges is identified; sometimes an organ that has penetrated can be visualized at the base.
Radiography — a deep “niche” is determined, fixed, not displaced when changing body position.
Ultrasound — visualizes infiltrates, signs of inflammation of adjacent organs.
Computed tomography of abdominal organs (CT of the abdominal cavity) — allows visualization of the ulcer and infiltrate.
Penetration of the duodenal ulcer into the head of the pancreas – 3D model
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Malignancy
Against the backdrop of a prolonged chronic inflammatory process, cell dysplasia of the epithelium occurs with the development of malignant transformation and tumor formation.
Diagnosis:
EGD with visualization of the process and biopsy;
computed tomography of abdominal organs (CT of the abdominal cavity).
Treatment — exclusively surgical with subsequent specific oncological treatment.
FAQ
1. What is peptic ulcer disease?
Peptic ulcer disease is a chronic condition in which defects of varying depth form on the mucous membranes of the stomach or duodenum.
2. What are the causes of peptic ulcer disease of the stomach?
The causes of the disease are increased acidity of gastric juice, Helicobacter pylori infection, long-term use of non-steroidal anti-inflammatory drugs, stress, poor nutrition and hereditary predisposition.
3. What are the symptoms of peptic ulcer disease of the stomach and duodenum?
The main symptoms include pain in the upper abdomen (often related to food intake), heartburn, nausea, and vomiting. Loss of appetite and weight may also be observed. When complications develop, characteristic symptoms appear — bleeding (manifested by vomiting with blood or black stool), perforation (manifested by peritonitis), stenosis (disruption of gastrointestinal tract patency).
4. What complaints are associated with peptic ulcer disease of the stomach?
Patients complain of burning or cutting pain in the epigastric area, heartburn, nausea, belching, sometimes vomiting, and also a feeling of heaviness or fullness after eating. When complications develop, characteristic complaints appear: with bleeding — vomiting with blood and black stool, with perforation — acute abdominal pain, with stenosis — weight loss and frequent, profuse vomiting.
5. How does peptic ulcer disease of the stomach and duodenum manifest in children?
In children, ulcer disease is less common, but can develop due to Helicobacter pylori infection, hereditary factors, chronic gastrointestinal diseases, as well as under the influence of stress and poor nutrition. Symptoms in children are similar to those in adults.
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Ndidi K. Gastric ulcers: causes, symptoms, treatment, and prevention. J Wetenschap Health. 2020;1(1):1-4.
3.
Naidu K. Peptic ulcer disease. In: Emergency surgery for low resource regions. Cham: Springer Nature Switzerland AG; 2021. p. 179-183. 85.
4.
Sidzenka VM. Peptic ulcer disease. Minsk: Belarusian State Medical University; 2019. 24 p. [In Russian.]
Weber DG, Bendinelli C. Damage control surgery for emergency general surgery. In: Acute care surgery handbook. Vol. 1. Cham: Springer International Publishing AG; 2017. p. 179-183. 397-398.
7.
Grigoriev PY. Clinical gastroenterology. Moscow; 2001. 681 p. [In Russian.]
8.
Zavada NV. Emergency surgery of the abdominal organs. Minsk: Belarus; 2005. 117 p. [In Russian.]