Infective Endocarditis: Etiology, Pathogenesis, Classification, Diagnosis, and Treatment Methods
Oleg K.Cardiovascular surgeon, MD
15 min read·May 27, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Infective endocarditis (IE) is a potentially life-threatening disease associated with inflammation of the endocardium, primarily the valve apparatus of the heart, caused by microbial invasion. Despite the development of antibiotic therapy and modern imaging techniques, the mortality rate of the total number of patients remains high.
3D animation – Infective endocarditis of the left side of the heart
3D animation – Infective endocarditis of the right side of the heart
Epidemiology
The incidence of infective endocarditis ranges from 3 to 15 cases per 100,000 population per year The incidence increases with age, peaking in those over 60 years due to the accumulation of risk factors such as valve prostheses, cardiac implants, chronic diseases, and frequent medical interventions. Men are about twice as likely to have the disease as women.
In recent decades, there has been a shift in the epidemiological profile: instead of patients with rheumatic heart disease and intravenous drug users, elderly patients, often with implanted valves, prostheses, and pacemakers, now predominate.
Etiology
Various microorganisms can be the cause of IE development.
Staphylococcus aureus is the most frequent, especially in nosocomial IE and in drug addicts.
Streptococcus viridans are classic pathogens in native valve disease in patients without obvious risk factors.
Enterococcus spp. – significant in elderly patients, often associated with urogenital interventions.
Coagulase-negative staphylococci are frequent causative agents in prosthetic valve infections.
HACEK group, fungi, gram-negative rod-shaped bacteria, and others are less frequent.
Risk factors include the presence of artificial valves, pacemakers, previous IE, heart defects, intravenous drug use, and chronic hemodialysis.
Pathogenesis
The pathogenesis of infective endocarditis involves several consecutive links:
Endothelial damage of valves (for instance, due to turbulent blood flow) → exposure of extracellular matrix.
Adhesion of platelets and fibrin → formation of a sterile thrombus (non-bacterial thrombotic endocarditis).
Microbial invasion – in transient bacteremia, microorganisms colonize the thrombus.
Formation of vegetations – dense clusters of fibrin, inflammatory cells, and bacteria protected from the immune response and antibiotics.
Destruction of valvular structures and possible embolization → systemic complications, sepsis, acute heart failure.
Immune mechanisms also contribute to the development of complications such as vasculitis and glomerulonephritis.
The key step is the formation of vegetations that promote persistence of infection and the development of embolic complications.
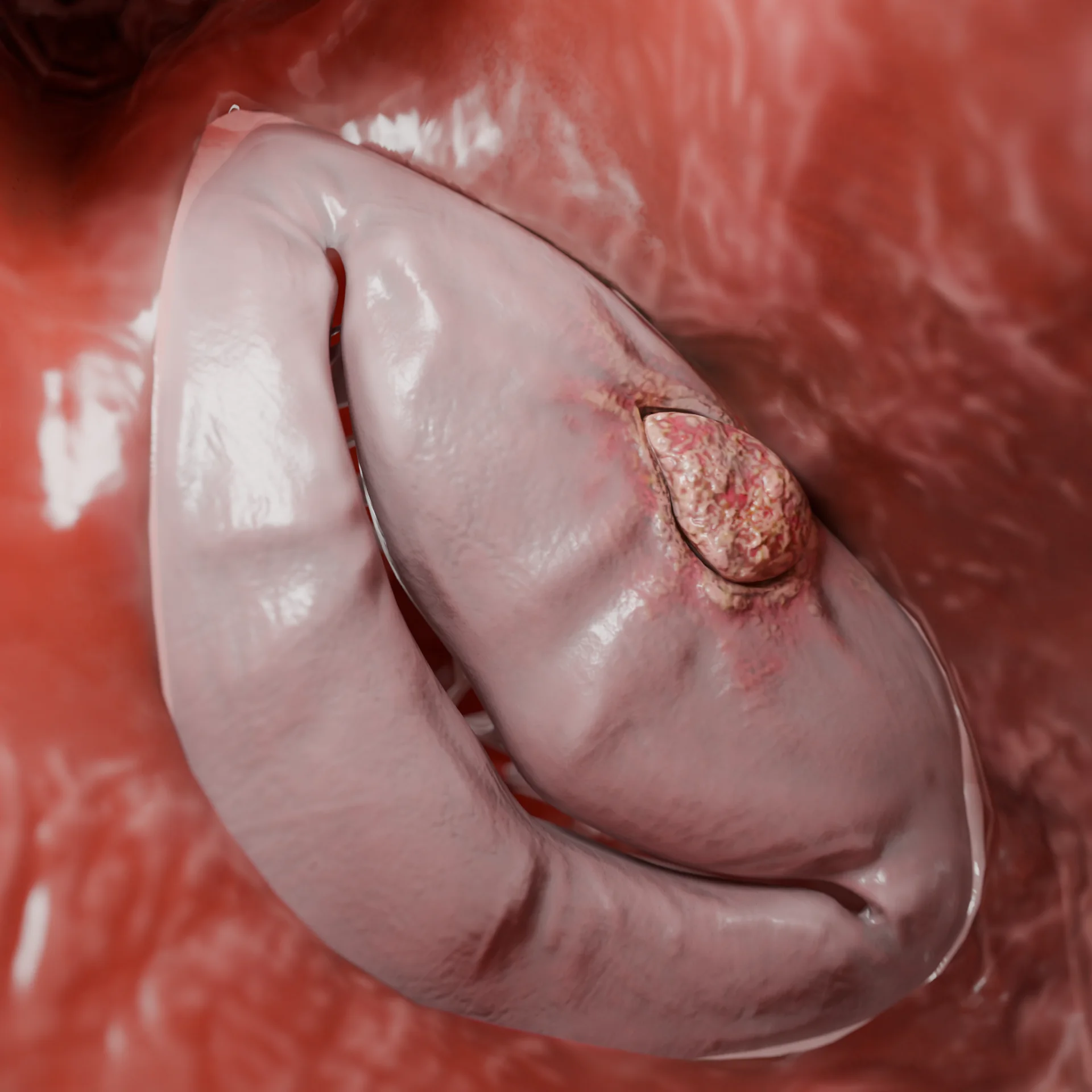
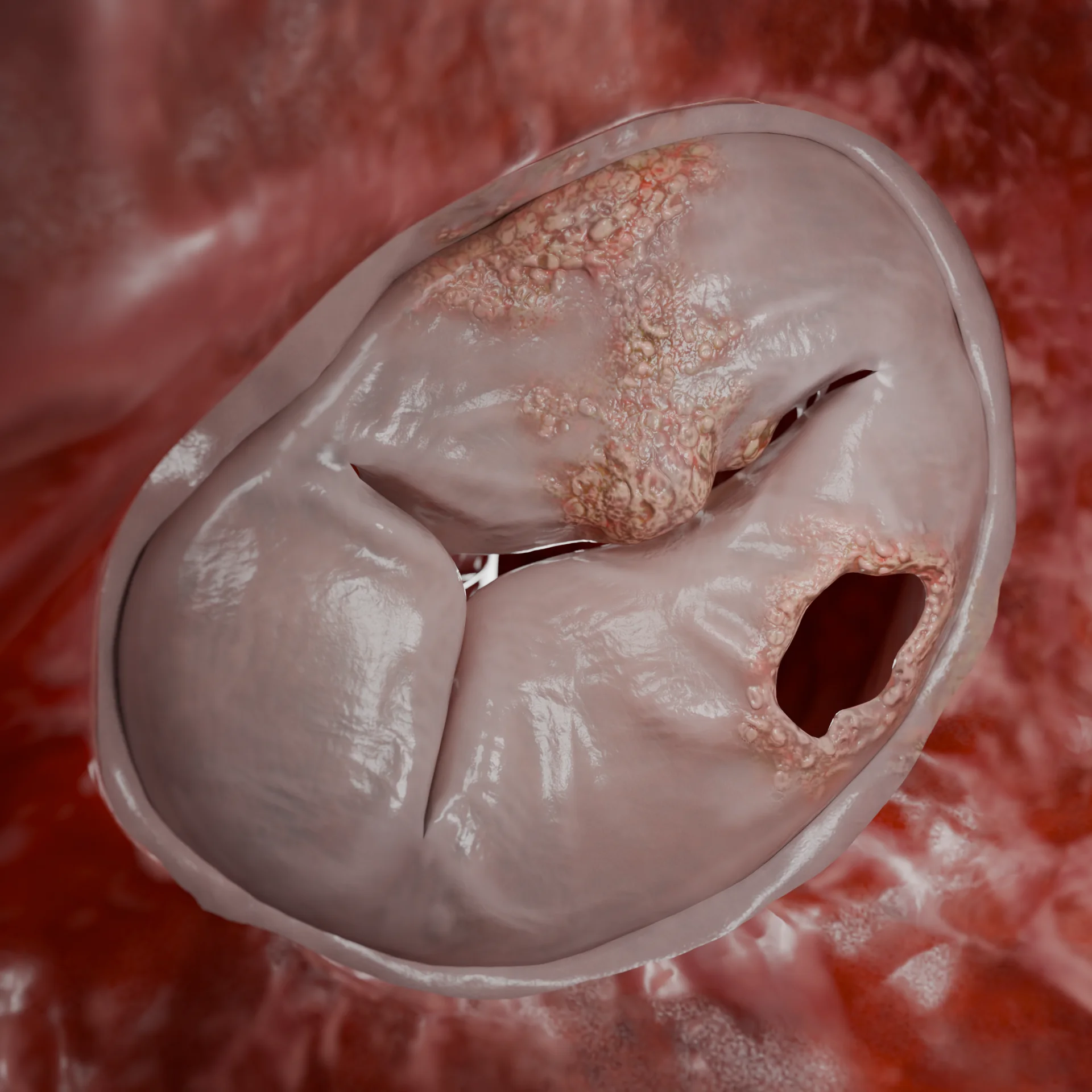
Vegetations on the mitral valveTricuspid valve leaflet perforation
Classification of infective endocarditis
By localization
Left-sided endocarditis
Involvement of the mitral and/or aortic valve (most common variant)
Right-sided endocarditis
Involvement of the tricuspid and/or (rarer) pulmonary valve (more common in injective drug users, patients with a central venous catheter)
Combined endocarditis
Simultaneous involvement of the right and left sides
Prosthetic endocarditis
Inflammation on a mechanical or biological valve prosthesis
Device-associated endocarditis
Infection associated with the leads of pacemakers, implantable cardioverter-defibrillators, etc.
Onset: prolonged (months) Course: latent or recurrent Pathogens (more often): low-virulence bacteria, culture-negative forms Features: prolonged inflammation, persistent valve changes, possible relapse after therapy
Left infective endocarditis (vegetations on valves and mitro-aortic junction) – 3D modelInfective right-sided endocarditis (vegetations and perforation on the tricuspid valve) – 3D model
Clinical manifestations
IE symptomatology is variable and can include both non-specific symptoms and life-threatening conditions.
General symptoms: fever, sweating, fatigue, weight loss.
Cardiac signs: new or altered murmur, signs of heart failure.
Embolic complications: stroke, limb ischemia, infarcts of internal organs.
Lesion of the conductive system: blockades, arrhythmias.
In severe course of IE may develop: septic shock, multi-organ failure.
In prosthetic endocarditis auscultatory murmurs may be less pronounced, periannular infection is more likely to develop: abscesses, pseudoaneurysms, fistulas.
Diagnosis of infective endocarditis
Laboratory methods:
General blood analysis: normocytic anemia, leukocytosis, thrombocytopenia.
Hemocultures: ≥3 samples ≥30 min apart before antibiotics (up to 95% sensitivity).
Serology/PCR: for culture-negative IE (Bartonella, Coxiella, Brucella, etc.).
Instrumental methods:
Echocardiography (PD echocardiography preferred over TT echocardiography): identifies vegetations, abscesses, pseudoaneurysms, perforations, prosthetic dysfunction. The sensitivity of transesophageal echocardiography exceeds 90%.
CT: allows detection of abscesses, pseudoaneurysms, emboli and complications of infective endocarditis.
PET-CT: detects areas of active inflammation and infection; especially valuable in prosthetic endocarditis and presence of devices.
Brain MRI: often reveals multiple emboli, even in the absence of neurologic symptoms.
Duke criteria
The Duke criteria — an internationally recognized diagnostic scheme for infective endocarditis, combining clinical, microbiological, and imaging findings.
The probability of having IE
Reliable: two major criteria, or one major and three minor, or five minor.
Possible: one major and one-two minor, or three minor.
Excluded: alternative diagnosis, lack of confirmation at autopsy, or complete resolution of symptoms without treatment.
Major criteria
Positive hemoculture (one of the following):
two or more positive blood cultures for typical microorganisms (e.g., S. aureus, S. viridans, Enterococcus spp.) from different samples;
repeated emboli or large vegetations with episode of emboli (> 10 mm), vegetations >15 mm, especially in left-sided IE even without emboli;
prosthetic endocarditis;
fungal IE, as well as IE caused by highly resistant microorganisms.
Contraindications:
decompensated general condition, multi-organ failure;
recent massive stroke with hemorrhagic component.
Types of operations (in the vast majority of cases, operations are performed under artificial circulation):
replacement (prosthetics) of the affected valve;
removal of vegetations, sanitation of abscesses;
reconstructive interventions (valve plasty, valve ring plasty, aortic root plasty): if the aortic root is involved, replacement with a conduit (artificial vascular prosthesis with artificial valve) or homograft (human donor valve with a section of ascending aorta) may be necessary;
removal of infected devices: if electrodes or pacemakers are involved, complete system removal is indicated; in TAVI-endocarditis, the operation is often associated with high mortality, but is indicated in case of treatment failure.
FAQ
1. What is infective endocarditis?
Infective endocarditis is an inflammatory disease of the heart’s inner lining (endocardium), most often involving the valves, caused by bacterial or fungal infection.
2. What symptoms are most characteristic of IE?
Most frequent symptoms: fever, chills, weakness, heart murmurs, weight loss. Complications can occur: strokes, emboli, heart failure.
3. Which bacteria most frequently cause IE?
The most common pathogens are: Staphylococcus aureus, Streptococcus viridans, Enterococcus spp. Staphylococcus epidermidis is frequently found in individuals with prostheses or intravascular devices.
4. How dangerous is infective endocarditis?
IE can lead to valve destruction, heart failure, embolic complications (strokes, organ infarcts), abscesses, and sepsis. Mortality reaches 20–30%.
5. Is it possible to cure IE without surgery?
Yes, in some cases — especially with native valves and sensitive microorganisms — complete cure with antibiotics is possible. However, surgery may be required in the event of complications.
6. When is surgery necessary in IE?
Surgery is indicated in cases of: • heart failure due to valve dysfunction; • abscesses, ruptures, perforations; • ineffective antibiotic therapy; • fungal infection; • recurrent emboli.
7. How long is antibiotic treatment administered?
The duration of therapy typically ranges from 4 to 6 weeks, depending on the pathogen, type of valve (native or prosthetic), and complications.
8. Can infective endocarditis be prevented?
Yes, in high-risk patients (e.g., with valve prostheses), antibiotic prophylaxis before certain dental or surgical procedures is recommended
9. Who is at high risk for IE?
Individuals with prosthetic valves, pacemakers, previous IE, congenital heart defects, as well as patients on hemodialysis and drug users.
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Delgado V, Ajmone Marsan N, de Waha S, Bonaros N, Brida M, Burri H, et al.; ESC Scientific Document Group. 2023 ESC guidelines for the management of endocarditis. Eur Heart J. 2023 Oct 14;44(39):3948–4042. doi:10.1093/eurheartj/ehad193
3.
Li M, Kim JB, Sastry BKS, Chen M. Infective endocarditis Lancet. 2024 Jul 27;404(10450):377–392. doi:10.1016/S0140-6736(24)01098-5
4.
Rajani R, Klein JL Infective endocarditis: a contemporary update Clin Med (Lond) 2020 Jan;20(1):31–35 doi:10.7861/clinmed.cme.20.1.1.
5.
Wang A, Gaca JG, Chu VH Management considerations in infective endocarditis: a review JAMA. 2018 Jul 3;320(1):72–83 doi:10.1001/jama.2018.7596.
6.
Baddour LM, Wilson WR, Bayer AS, Fowler VG Jr, Tleyjeh IM, Rybak MJ, et al.; American Heart Association Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young, Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and Stroke Council. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications: a scientific statement for healthcare professionals from the American Heart Association. Circulation. 2015 Oct 13;132(15):1435–1486. doi:10.1161/CIR.0000000000000296
7.
Iung B. Infective endocarditis: epidemiology, pathophysiology and histopathology Presse Med 2019 May;48(5):513–521 doi:10.1016/j.lpm.2019.04.009
8.
Chambers HF, Bayer AS Native-valve infective endocarditis N Engl J Med. 2020 Aug 6;383(6):567–576 doi:10.1056/NEJMcp2000400
9.
Jain A, Subramani S, Gebhardt B, Hauser J, Bailey C, Ramakrishna H. Infective endocarditis—update for the perioperative clinician J Cardiothorac Vasc Anesth 2023 Apr;37(4):637–649 doi:10.1053/j.jvca.2022.12.030
St. Petersburg FL 33702, 7901 4th St N STE 300, USA
Thank you!
Your message is sent! Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io
Cookie Consent
We use cookies to enhance your browsing experience, analyze site traffic, and deliver content. Please choose whether you accept all cookies or wish to reject non-essential tracking.
Cookie Preferences
Manage your cookie preferences below:
Essential cookies enable basic functions and are necessary for the proper function of the website.
Name
Description
Duration
Geolocation Config
This cookie is used to store the consent settings based on the visitor's location.
30 days
Cookie Preferences
This cookie is used to store the user's cookie consent preferences.
30 days
Google reCAPTCHA helps protect websites from spam and abuse by verifying user interactions through challenges.
Name
Description
Duration
_GRECAPTCHA
Google reCAPTCHA sets a necessary cookie (_GRECAPTCHA) when executed for the purpose of providing its risk analysis.
179 days
Statistics cookies collect information anonymously. This information helps us understand how visitors use our website.
Google Analytics is a powerful tool that tracks and analyzes website traffic for informed marketing decisions.
ID used to identify users for 24 hours after last activity
24 hours
_gat
Used to monitor number of Google Analytics server requests when using Google Tag Manager
1 minute
_gac_
Contains information related to marketing campaigns of the user. These are shared with Google AdWords / Google Ads when the Google Ads and Google Analytics accounts are linked together.
90 days
__utma
ID used to identify users and sessions
2 years after last activity
__utmt
Used to monitor number of Google Analytics server requests
10 minutes
__utmb
Used to distinguish new sessions and visits. This cookie is set when the GA.js javascript library is loaded and there is no existing __utmb cookie. The cookie is updated every time data is sent to the Google Analytics server.
30 minutes after last activity
__utmc
Used only with old Urchin versions of Google Analytics and not with GA.js. Was used to distinguish between new sessions and visits at the end of a session.
End of session (browser)
__utmz
Contains information about the traffic source or campaign that directed user to the website. The cookie is set when the GA.js javascript is loaded and updated when data is sent to the Google Anaytics server
6 months after last activity
__utmv
Contains custom information set by the web developer via the _setCustomVar method in Google Analytics. This cookie is updated every time new data is sent to the Google Analytics server.
2 years after last activity
__utmx
Used to determine whether a user is included in an A / B or Multivariate test.
18 months
_ga
ID used to identify users
2 years
_gali
Used by Google Analytics to determine which links on a page are being clicked
30 seconds
Clarity is a web analytics service that tracks and reports website traffic.

.webp)
.webp)





















