Rhinitis: Symptoms, Stages, Diagnosis, and Treatment
Danata A.Otorhinolaryngologist, MD
20 min read·April 14, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Rhinitis is inflammation of the nasal cavity mucosa. All types of rhinitis share common symptoms, such as nasal congestion and discharge, also known as rhinorrhea. However, each type also has specific symptoms that help distinguish it from the others.
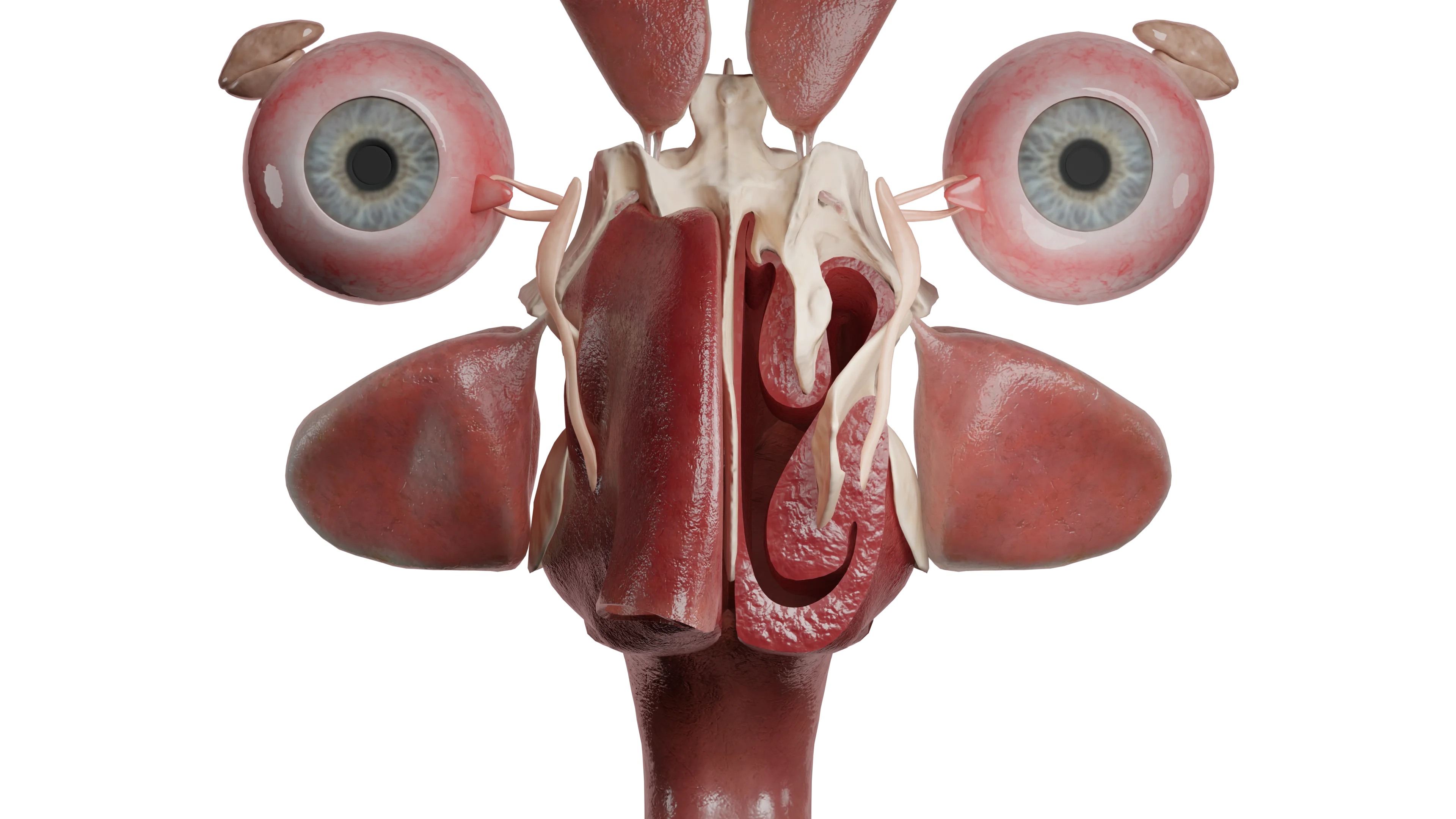
Nasal cavity (section)
Classification of rhinitis
Acute rhinitis:
Stage 1, irritation;
Stage 2, serous discharge;
Stage 3, seropurulent discharge.
Chronic rhinitis:
Infectious;
Allergic;
Hypertrophic;
Vasomotor;
Atrophic;
Ozena.
Etiology
Acute rhinitis is inflammation of the nasal cavity mucosa lasting no more than 12 weeks. It is caused by viruses or bacteria that reach the epithelial surface and trigger a pathological reaction. This disease is non-specific. The viruses most commonly causing acute rhinitis are: adenovirus, rhinovirus, RS-virus, influenza, and parainfluenza viruses. Among bacteria causing nasal mucosa inflammation are streptococci, staphylococci, and pneumococci. Acute rhinitis can be an initial manifestation of specific diseases such as measles, scarlet fever, diphtheria, and meningococcal infection. For the development of the pathological process, in addition to the presence of pathogenic microflora, mucosal changes such as dryness and crusting, decreased general or local immunity, and the presence of chronic infections in the decompensation phase are necessary.
Chronic inflammation is considered to last more than 12 weeks. If acute rhinitis persists beyond this period, it transitions into chronic infectious rhinitis, which is why the pathogens for these conditions are the same. This form of rhinitis can also accompany infectious diseases such as syphilis, tuberculosis, histoplasmosis, blastomycosis, leprosy, and others. These pathologies will be covered in more detail in respective sections.
Allergic rhinitis occurs when allergens affect the mucosa. The most common allergens are pet dander, dust mites, plant pollen, and mold spores. When allergens affect the mucosa, an IgE-mediated immune response develops with the release of inflammatory mediators that trigger pathological reactions. There is a hereditary predisposition and a general tendency towards atopy. Allergic rhinitis can also be a manifestation of helminth invasion, such as giardiasis, more common in children, pathogenetically explained by general sensitization of the body.
Hypertrophic rhinitis most often develops as a result of impaired nasal breathing of post-traumatic nature or chronic inflammation in the nasal cavity or paranasal sinuses.
Vasomotor rhinitis occurs when there is a disturbance in neuro-reflex processes, increasing hypersensitivity to various irritants).
Vasomotor rhinitis includes:
Medicamentous (due to prolonged use of nasal decongestants);
Hormonal (in pregnant women due to increased progesterone, in patients with thyroid diseases);
Professional (in contact with dust, wool, sawdust);
Emotional (during stress);
Nutritional (when consuming spicy, hot dishes, alcohol).
These forms of rhinitis have different etiologies but similar clinical and pathomorphological manifestations. The diagnosis is made based on a carefully collected medical history and identification of the causal factor.
Vasomotor rhinitis (left nasal cavity in section): 3D model
The etiology of atrophic rhinitis is not fully understood. Some authors attribute the causes of the disease to poor environmental conditions (dry air, dust), trauma or surgery in the nasal cavity, improper nasal hygiene, autoimmune diseases, hormonal changes (menopause, aging), and deficiencies in trace elements (particularly iron) and vitamins.
Ozena, or pruritic runny nose, is a special case of atrophic rhinitis. The causative agent is the bacterium Klebsiella ozaenae, but for the development of the disease in addition to pathogenic microflora, predisposing factors such as foci of chronic infection in the nasal cavity or perinasal sinuses, disturbance of aerodynamics, dryness and the presence of microcracks are necessary.
Anatomy
Acute rhinitis progresses through 3 stages, successively replacing each other. The first stage (dry irritation) is characterized by hyperemia and dryness of the mucosa. This stage lasts from several hours (more frequently) to several days.
The stage of serous discharge is characterized by hyperemia and edema of the mucosa, its hyperemia, and small foci of submucosal hemorrhages (petechiae), increased mucus formation.
By days 4-5 from the onset of the disease, the discharge becomes mucopurulent due to the overproduction of lymphocytes and desquamated epithelium. With a favorable course, by the end of 7-10 days, the inflammation resolves.
Chronic infectious rhinitis is characterized by non-specific changes, such as hyperemia of the mucosa, congestion of the nasal turbinates, and hyperplasia of goblet cells with increased secretion production.
Allergic rhinitis is characterized by pale mucosa with a cyanotic tinge and pronounced edema of the nasal turbinates, with abundant discharge of clear mucous secretions. Allergic rhinitis is often combined with chronic polyposis rhinosinusitis, and in such cases, rhinoscopy reveals polyposis-altered mucosa or polyps.
In hypertrophic rhinitis, an excess of bone tissue in the inferior nasal turbinate is most often found along its entire length. Less common are vascular and fibrous forms, in which there is proliferation of blood vessels or connective tissue within the nasal turbinates.
Vasomotor rhinitis is morphologically characterized by congestion of the cavernous tissue vessels in the nasal turbinates, which become purple-bluish, thickened, with the nasal passages rarely narrowed, and an increase in the number of goblet cells. When the parasympathetic system is disrupted, there is hyperproduction of mucus, while disruption in the sympathetic system leads to edema and nasal congestion.
In atrophic rhinitis, a large number of crusts are found in the nasal cavity, the mucosa is pale pink, thinned, matte, ‘parchment-like’, with scant serous-mucous discharge. As the disease progresses, atrophic processes affect the olfactory nerve and blood vessels of the mucosa.
Ozena is characterized by the same changes as atrophic rhinitis, but as the process progresses, deep-lying tissues are destroyed, including the bone part of the nasal turbinates due to osteoclasts. Blood vessels obliterate and scar. The number of goblet cells is sharply reduced, cilia are absent, resulting in non-functional mucociliary clearance, and nasal passages widen due to the deficit of nasal turbinate tissue. Tissue destruction contributes to the production of a foul odor. Rhinoscopy reveals a pathologically wide nasal cavity, with the posterior wall of the nasopharynx clearly visible. Gray-green crusts abundantly line the nasal cavity, forming so-called casts.
Symptoms of rhinitis
Acute rhinitis begins with marked difficulty breathing, sneezing, burning in the nose, corresponding to the first phase. General symptoms develop: headache, an increase in body temperature to subfebrile or febrile levels. In the transition to the next phase, there are abundant mucous discharges, which in contact with the skin in the area of the nasolabial triangle cause its maceration, due to its chemical composition. Nasal congestion worsens, lacrimation appears, some patients note congestion in the ears.
3D animation: Acute rhinitis
When moving to stage 3 nasal discharge acquires yellow-green color, becomes thicker, stuffiness decreases. In any of the stages there may be pain in the projection of the sinuses due to the development of marked edema of the mucosa in the sinuses themselves and in the places of their exit into the nasal cavity.
Acute rhinitis, stage 3 seropurulent discharge: 3D model
Chronic infectious rhinitis is a slow-progressing disease in which patients note difficulty in nasal breathing and constant mucous or mucopurulent discharge with an unpleasant odor. Sometimes it is accompanied by headaches or anosmia.
Allergic rhinitis is characterized by abundant serous discharge upon contact with an allergen, sneezing, itching in the nose and congestion, and may also include signs of allergic conjunctivitis with lacrimation and itching in the eyes. The aforementioned complaints manifest immediately upon contact with an allergen. Clinically, allergic rhinitis is subdivided into seasonal and perennial, persistent and intermittent, mild and moderate-severe. Seasonal rhinitis appears once or several times a year and is usually associated with the flowering of certain plants, while perennial rhinitis is constant and more often associated with household allergens (dust mites, pet hair, etc.). Intermittent rhinitis manifests up to 4 days a week or up to 4 weeks a year, while persistent rhinitis is characterized by continuity.
Mild rhinitis is not characterized by sleep disturbances or general activity impairment, while moderate-severe rhinitis, on the contrary, causes significant discomfort that disrupts the usual rhythm of life, negatively affecting sleep and work capacity. It is important to emphasize the close relationship between allergic rhinitis and bronchial asthma, due to a common pathogenetic mechanism. Allergic rhinitis is considered a risk factor in the development of bronchial asthma. It has been proven that without adequate treatment of allergic manifestations in the nose, the course of bronchial asthma significantly worsens. There is also a connection between this pathology and atopy. It manifests more frequently in childhood.
Hypertrophic rhinitis is characterized by persistent pronounced difficulty in nasal breathing, snoring, and less frequently, anosmia.
Vasomotor rhinitis is characterized by intermittent clinical manifestations. There is periodic itching in the nose, sneezing, nasal congestion, and watery or mucous discharge, often dripping down the posterior pharyngeal wall. Patients note the appearance of complaints with changes in air temperature or humidity, body position in space (marked worsening when lying on the side), increased blood pressure, strong odors, etc. It typically manifests in adulthood.
Patients with atrophic rhinitis complain of dryness and itching in the nasal cavity, difficulty breathing despite pathologically wide nasal passages, the so-called “empty nose syndrome”, poorly detachable crusts, after removal of which no relief occurs. In some cases, nosebleeds may occur. As the process progresses, the olfactory nerves are affected and anosmia develops, nasal septum perforation may form, and nosebleeds may develop. Since ozena is a subtype of atrophic rhinitis, all of the above complaints will be characteristic of it as well. A distinguishing feature is the persistent foul odor from the nose, not perceived by the patients themselves. As a result, people around them tend to avoid interaction, which affects the patients’ psychological state. When attempting to remove the crusts, they are rejected as casts, and bleeding is minimally expressed. The general symptoms include headache, marked weakness, and fatigue.
Diagnosis of rhinitis
To diagnose acute or chronic rhinitis, in most cases, a general examination (otorhinolaryngoscopy) is sufficient. The nature of complaints, condition of the mucosa, and discharge are assessed, and a thorough medical history is collected. In cases of prolonged course, lack of treatment effect, and presence of pain in the projection of the paranasal sinuses, an X-ray of the nasal sinuses is recommended.
For chronic infectious rhinitis, a bacteriological culture of nasal discharge is performed to identify the pathogen and determine sensitivity to antibacterial drugs.
For the diagnosis of allergic rhinitis, various tests are used depending on the clinic’s equipment. The rhinocytogram with quantitative determination of eosinophils in nasal mucus has lost its value today due to uncertain sensitivity, as the absence of eosinophils does not mean the absence of the disease, and their presence can also be found in patients with non-allergic rhinitis. The most common method is various skin tests (scarification, prick tests, etc.) where the allergen is applied to/under the skin, and the reaction at the contact site is recorded after a certain time. The “gold standard” for diagnosing allergic rhinitis is the determination of specific IgE to the most common allergens in blood serum.
To detect hypertrophic bony rhinitis, anemization of the nasal turbinates is performed. The diagnosis is valid with a negative test.
Vasomotor and atrophic rhinitis are diagnosed after rhinoscopy, collection of complaints, and medical history.
Vasomotor rhinitis (nasal shells in section): 3D model
In atrophic rhinitis and ozena, bacteriologic examination of the nasal cavity discharge is also performed. A blood test is performed to determine hemoglobin and serum iron levels. If perforation is present, a free edge biopsy with pathomorphologic examination is performed. If symptoms worsen rapidly, the patient should be evaluated for ANCA vasculitis. The diagnosis of ozaena is 100% when Klebsiella ozaenae is detected by microbiologic examination or blood examination with immunologic tests and antibody detection.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Treatment
Treatment of acute rhinitis is symptomatic. Nasal decongestants are prescribed (phenylephrine, xylometazoline, oxymetazoline), which reduce edema and mucous discharge, after which it is recommended to perform nasal toilet with saline solutions or seawater to evacuate pathologic contents from the nasal cavity. In the presence of pronounced general symptoms, it is possible to use NSAIDs (paracetamol, ibuprofen).
For the treatment of chronic infectious rhinitis, it is necessary to prescribe antibiotic therapy locally or systemically, taking into account sensitivity. Regular nasal lavage with saline solutions or sea water is also prescribed.
In the treatment of allergic rhinitis, the most important thing is the elimination of the causative factor (allergen). Depending on the severity of the course, combinations of different drugs are prescribed. As therapy, intranasal decongestants are used for a short course of no more than 7-10 days. Antihistamines for local or systemic use are necessarily prescribed. In case of severe symptoms it is recommended to use glucocorticosteroids intranasally for a long time (at least 1 month) or antileukotriene drugs systemically. Most patients achieve sustained remission with ASIT (allergen-specific immunotherapy), which is an etiotropic method (i.e., it combats the disease’s cause rather than its symptoms). The essence of treatment is the long-term introduction of allergens into the patient’s body in minimal quantities (sublingually or subcutaneously). This results in the development of “immunity” to subsequent contacts with the allergen, minimizing unwanted reactions.
Treatment of hypertrophic bony rhinitis is surgical. It involves performing a partial conchotomy, in which excess bone tissue is gently removed while preserving the anatomical landmarks and soft tissues of the nasal turbinates.
As therapy for vasomotor rhinitis, antihistamines of local or systemic action, topical hormonal preparations for a course of 1 month are used, and regular moisturizing of the mucosa with isotonic solutions is recommended. In the absence of an effect from conservative therapy, surgical intervention is performed using various devices (laser coagulation/submucosal vasotomy/radiofrequency or ultrasonic destruction, etc.), during which the nasal turbinates are partially damaged from the inside and then scar, reducing in size, while the mucosa remains intact and continues its function.
For atrophic rhinitis, treatment is aimed at moisturizing the mucosa. For this purpose, sprays based on isotonic solutions, sea water with the addition of dexpanthenol or hyaluronic acid are used. If there are no contraindications, lubricating the mucosa with iodine solutions is prescribed to irritate and stimulate goblet cells and increase the production of mucous secretion. A good effect is observed when treating the mucosa with oil solutions containing vitamins A, D, E, such as sea buckthorn, peach, or sesame oil, but they should be used in limited amounts as they impair the function of the ciliated epithelium. If pathogenic microorganisms are detected, topical antibacterial therapy is prescribed.
For the treatment of ozena, systemic (preferably parenteral) antibiotic therapy is necessary, based on sensitivity results. Locally, as with atrophic rhinitis, regular nasal rinsing with saline solution or seawater with iodine preparations is recommended, along with moisturizing with oil solutions. To achieve a therapeutic effect, after softening the crusts, they must be regularly removed and then the nasal cavity irrigated with local antibacterial preparations.
FAQ
1. What are the main symptoms of rhinitis?
Common symptoms include: • Nasal congestion; • Nasal discharge (mucous or purulent); • Sneezing, itching in the nose; • Reduced sense of smell; • Headache, weakness (in acute rhinitis).
2. What stages of acute rhinitis are identified?
Acute rhinitis progresses through three stages: 1. Stage of dry irritation (dryness, burning in the nose). 2. Serous discharge stage (profuse watery discharge). 3. Stage of mucopurulent discharge (thick yellow-green discharge).
3. What complications can arise with rhinitis?
• Sinusitis (inflammation of the nasal sinuses); • Otitis (inflammation of the middle ear); • Anosmia (loss of smell); • Nosebleeds.
4. How to differentiate rhinitis from sinusitis?
•Rhinitis is an inflammation of the nasal mucosa, accompanied by nasal congestion and discharge; •Sinusitis is an inflammation of the nasal sinuses, accompanied by pain in the sinus area, thick yellow-green discharge, fever.
5. What factors contribute to the development of rhinitis?
6. What complications can occur due to improper treatment of rhinitis?
• Transition to a chronic form; • Development of sinusitis, otitis; • Decreased quality of life (sleep disturbances, reduced performance).
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Sclafani AP, Dyleski RA, Pitman MJ, Schantz SP. Total otolaryngology—head and neck surgery. New York: Thieme Medical Publishers; 2015. ISBN: 978-1-60406-646-3.
3.
Behrbohm H, Kaschke O, Nawka T, Swift A. Bolezni ukha, gorla i nosa [Ear, Nose, and Throat Diseases]. 2nd ed. Moscow: MEDpress-inform; 2016. 776 p. [In Russian.]
4.
Green RJ, Feldman C, Van Niekerk A, McDonald M, Friedman R, Richards GA. Treating acute rhinitis and exacerbations of chronic rhinitis — a role for topical decongestants? S Afr Fam Pract (2004) [Internet]. 2020 Mar 24;62(1):e1–e5. doi:10.4102/safp.v62i1.5053. PMID: 32242436; PMCID: PMC8378128.
Available from: https://doi.org/10.4102/safp.v62i1.5053
5.
Akhouri S, House SA. Allergic rhinitis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jul 16 [updated 2025 Jan–]. PMID: 30844213.
Available from: https://www.ncbi.nlm.nih.gov/books/
St. Petersburg FL 33702, 7901 4th St N STE 300, USA
Thank you!
Your message is sent! Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io
Cookie Consent
We use cookies to enhance your browsing experience, analyze site traffic, and deliver content. Please choose whether you accept all cookies or wish to reject non-essential tracking.
Cookie Preferences
Manage your cookie preferences below:
Essential cookies enable basic functions and are necessary for the proper function of the website.
Name
Description
Duration
Geolocation Config
This cookie is used to store the consent settings based on the visitor's location.
30 days
Cookie Preferences
This cookie is used to store the user's cookie consent preferences.
30 days
Google reCAPTCHA helps protect websites from spam and abuse by verifying user interactions through challenges.
Name
Description
Duration
_GRECAPTCHA
Google reCAPTCHA sets a necessary cookie (_GRECAPTCHA) when executed for the purpose of providing its risk analysis.
179 days
Statistics cookies collect information anonymously. This information helps us understand how visitors use our website.
Google Analytics is a powerful tool that tracks and analyzes website traffic for informed marketing decisions.
ID used to identify users for 24 hours after last activity
24 hours
_gat
Used to monitor number of Google Analytics server requests when using Google Tag Manager
1 minute
_gac_
Contains information related to marketing campaigns of the user. These are shared with Google AdWords / Google Ads when the Google Ads and Google Analytics accounts are linked together.
90 days
__utma
ID used to identify users and sessions
2 years after last activity
__utmt
Used to monitor number of Google Analytics server requests
10 minutes
__utmb
Used to distinguish new sessions and visits. This cookie is set when the GA.js javascript library is loaded and there is no existing __utmb cookie. The cookie is updated every time data is sent to the Google Analytics server.
30 minutes after last activity
__utmc
Used only with old Urchin versions of Google Analytics and not with GA.js. Was used to distinguish between new sessions and visits at the end of a session.
End of session (browser)
__utmz
Contains information about the traffic source or campaign that directed user to the website. The cookie is set when the GA.js javascript is loaded and updated when data is sent to the Google Anaytics server
6 months after last activity
__utmv
Contains custom information set by the web developer via the _setCustomVar method in Google Analytics. This cookie is updated every time new data is sent to the Google Analytics server.
2 years after last activity
__utmx
Used to determine whether a user is included in an A / B or Multivariate test.
18 months
_ga
ID used to identify users
2 years
_gali
Used by Google Analytics to determine which links on a page are being clicked
30 seconds
Clarity is a web analytics service that tracks and reports website traffic.