Brain Contusion: Etiology, Classification, Clinical Presentation, Diagnosis, and Treatment
Artur D.Neurosurgeon, MD
14 min read·February 12, 2026
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Traumatic brain injury is a condition characterized by damage to the skull and intracranial contents by mechanical energy.
The incidence of traumatic brain injury is 35% of the total body trauma, and the mortality rate from traumatic brain injury, according to various literature sources, can reach up to 60%.
Brain contusion is a form of focal traumatic brain injury where irreversible damage to the brain parenchyma occurs due to microvascular and macrovascular disorders. The injury is accompanied by the development of edema, the formation of contusion foci and intracerebral hematomas, leading to irreversible destruction of brain tissue.
Brain contusions of varying degrees occur in 17–50% of severe traumatic brain cases and can be both an independent form of traumatic brain injury and occur alongside other brain injuries. The mortality rate from brain contusions is 30–40% and directly correlates with the presence of concomitant brain injuries.
Etiology of brain contusions
The etiology of brain contusions directly correlates with the causes of traumatic brain injury in the adult and pediatric populations. The main causes of traumatic brain injury are commonly the following:
Road traffic accidents;
Falls;
Violent injuries;
Sports injuries.
Pathogenesis of brain contusions
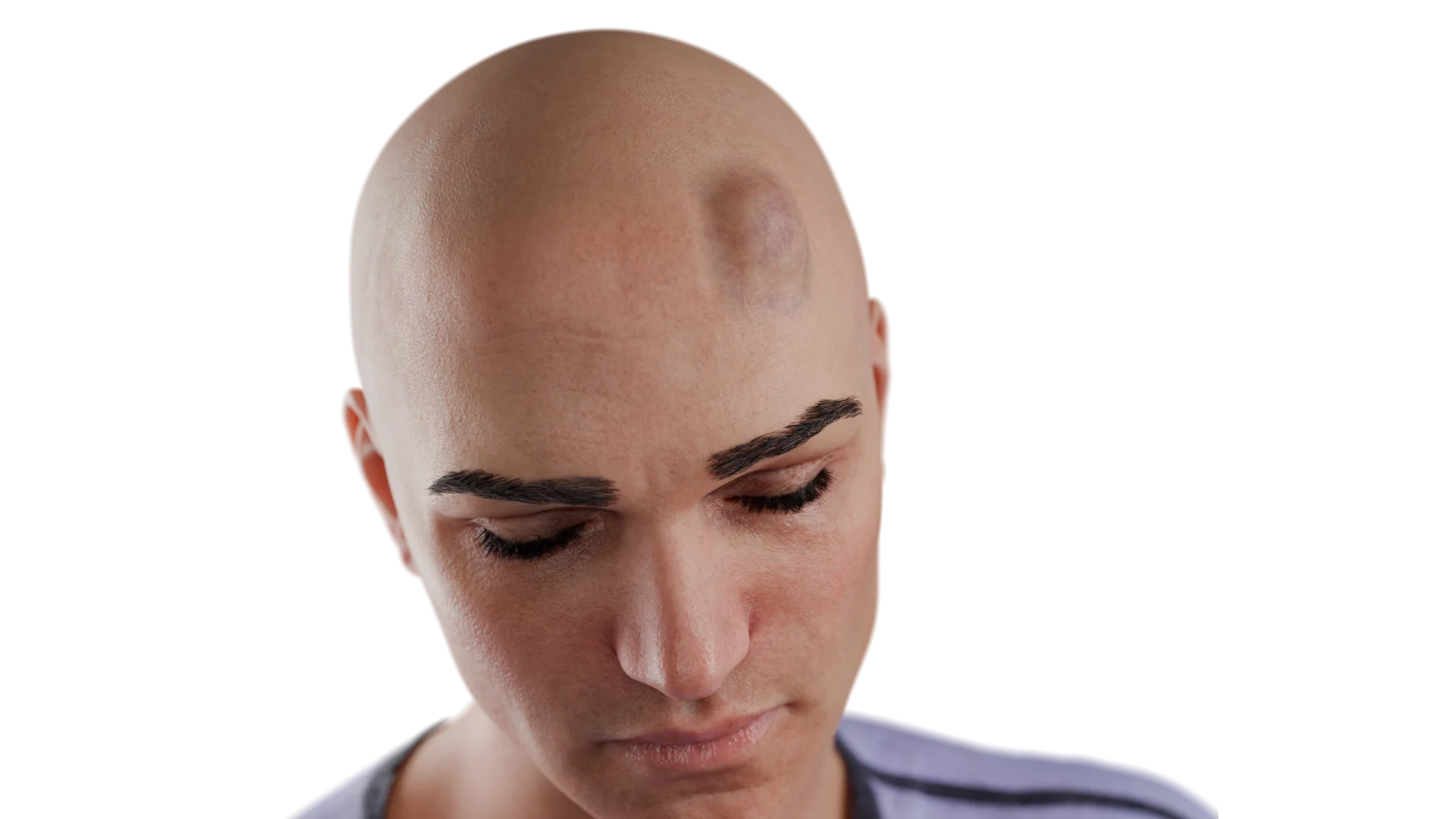
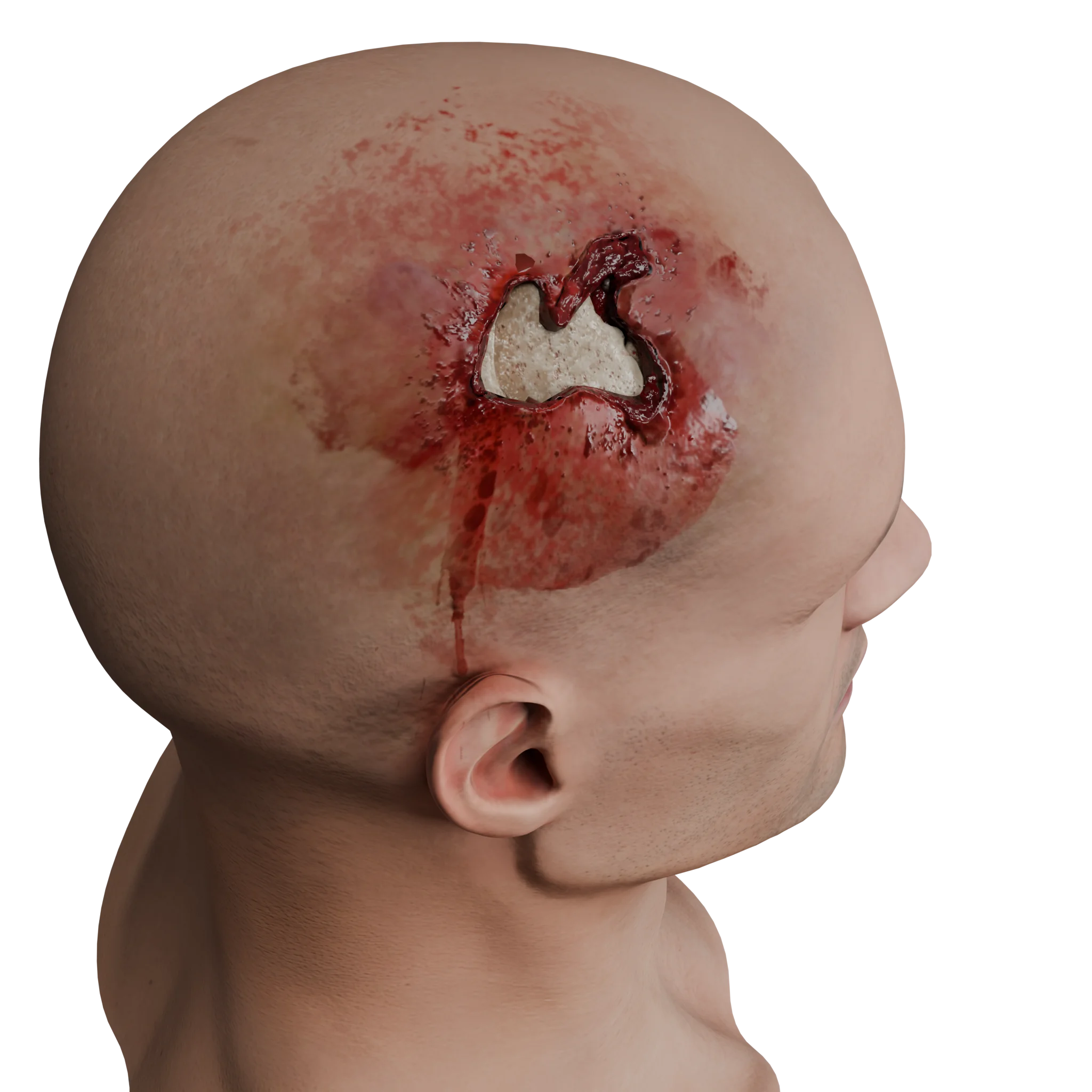
The pathogenetic mechanism of brain contusions is described by the coup-contrecoup theory, which involves the direct transfer of mechanical energy to the rigid bony structures of the skull, causing a focus of brain trauma at the point of kinetic energy application.
Brain contusions, occurring directly at the site of contact with the injurious agent, are caused by the brain’s contact with the rigid bones of the skull. Subsequently, due to the dissemination of energy in brain tissue and the pressure gradient changes, an opposite contusion focus forms due to cavitation interactions (contrecoup point).
After forming the primary contusion focus, part of the nerve cells in the focus die, leading to lysis and the release of chemokines and interleukins, reactive oxygen species, and proteases by the cells. These substances violate the permeability of the blood-brain barrier, inducing brain edema development.
Released free radicals damage DNA and disrupt mitochondrial function of the cells, exacerbating cellular edema and subsequent death of neurons and neuroglia.
The formation of brain edema begins with vasogenic edema due to damage to the blood-brain barrier, developing about 12–24 hours after injury. This is followed by cytotoxic edema resulting from the glial cell and neuron edema due to the release of free radicals and their subsequent death. This process’s progression is observed over 7–10 days after the injury.
The most common contusions are noted in the lower and inferolateral parts of the frontal and temporal lobes of the brain. These areas are most vulnerable to contusion due to the anatomical features of the skull and the distribution of kinetic energy in the structures of the anterior and middle cranial fossae.
An additional factor is the local deformation of the skull since the orbital, temporal, and sphenoidal regions demonstrate more intensive vibrations upon impact in experiments.
Classification of brain contusions
From a morphological substrate and clinical presentation perspective, brain contusions are classified into mild, moderate, and severe contusions.
3D animation: Cerebral contusions
Mild brain contusion
For a mild contusion, the following is typical:
Brief loss of consciousness lasting up to several minutes;
Autonomic reactions;
Mild neurological disorders in the form of coordination disturbances;
Nystagmus.
In instrumental studies, mild contusions are visualized on computed tomography. They are characterized by an area of reduced density in brain tissue (approximate density 16–20 Hounsfield units).
Upon more detailed examination, performing magnetic resonance imaging, foci of microhemorrhages can be visualized in this area. These changes typically disappear two weeks after injury and do not leave any post-traumatic changes.
Moderate cerebral contusion
For a moderate contusion, the following is characteristic:
Presence of small hemorrhagic foci clearly visible on neuroimaging, maintaining the differentiation of sulci and gyri.
Loss of consciousness from tens of minutes to several hours.
The entire spectrum of focal neurological disorders: mental impairment, motor function, sensory disturbances, etc.
In neuroimaging, such contusions are characterized by small foci of hemorrhagic soaking in the damaged brain tissue areas.
A severe brain contusion is clinically characterized by loss of consciousness from several hours to several weeks, accompanied by significant neurological deficits with dominant brainstem symptoms.
In neuroimaging, these contusions are characterized by dense tissue foci with areas of reduced density, presented with brain debris.
There is also a classification of brain contusions reflecting purely neuroimaging patterns.
In this classification, contusions are divided into:
Contusion type 1 is characterized by the presence of a brain CT focal area of decreased density (+18–25 HU).
Contusion type 2 is characterized by the presence on a brain CT of small, scattered hemorrhagic foci with a density of approximately 50 HU.
Contusion type 3 is characterized by the presence of the areas of heterogeneously increased density with compactly located hemorrhagic transformation foci of small and medium size fully around 64–76 HU.
Contusion type 4 is characterized by single or multiple foci of increased homogeneous oval-shaped density, up to 76 HU.
Clinical Manifestations
The clinical presentation of brain contusions directly consists of non-focal and focal neurological symptoms.
Non-focal symptoms include:
Headache;
Dizziness;
Nausea;
Vomiting;
Loss of consciousness.
Herewith, the loss of consciousness is a clinical criterion correlating with the severity of the brain contusion. Loss of consciousness after injury can last from a few seconds to a few weeks.
The manifestation of focal neurological symptoms directly depends on the localization of the contusion focus.
The most common brain contusion localizations are the frontal (40–50%) and temporal lobes (35–45%) of the brain.
In the case of frontal lobe contusion foci, the clinical picture can include:
Mental disorders;
Speech disorders in the form of motor aphasia;
Gaze paresis;
Anosmia.
Cortical damage may lead to:
Mono- and hemipareses;
Facial muscle paresis;
Hypoglossal nerve paresis.
For damage to the temporal lobe of the brain, the following is typical:
Sensory aphasia;
Higher nervous activity function disorders (alexia, acalculia, agraphia);
Homonymous hemianopsia due to visual tract damage.
The parietal lobe is a relatively rare site for brain contusions due to its superficial location and distance from the base of the skull. Contusions in this area are primarily developed due to the coup mechanism rather than the counter-coup mechanism. The clinical presentation of focal neurological symptoms of contusions in this area is characterized by sensory disturbances.
Occipital lobe brain injuries occur relatively rarely due to the cushioning properties of the cerebellar tentorium. Visual agnosia and homonymous hemianopsia, up to complete cortical blindness with injury to both occipital lobes, are often found when this lobe is damaged.
Contusions of the cerebellum are more often formed by the impact mechanism and are characterized by the development of unilateral or bilateral hypotonia and coordination disorders.
Diagnosis of brain contusions
Upon admission of the patient to the emergency room, the diagnostic algorithm for brain contusions consists of the following stages:
1. Assessment of consciousness level using the GCS (Glasgow Coma Scale)
This step allows for determining the patient’s level of consciousness and estimating the severity of brain structure damage, suggesting possible treatment options (surgical or non-surgical).
2. Medical history
It is necessary to specify the timing of injury onset, the mechanism of injury, and whether there was a loss of consciousness after the injury.
This step allows for understanding the dynamics of symptom progression and inferring possible injuries considering the injury mechanism. For certain injury mechanisms (e.g., fall from height), it’s essential to consider the possibility of combined head and body injuries, which may complicate the treatment prognosis.
3. Visual examination of the patient
Includes examination of the head area and checking for concomitant soft tissue damage in areas of the body other than the head.
This step helps highlight the location of soft tissue in head injuries, allowing inference of the brain contusion’s possible location. Additionally, this step is essential for patient care, treating soft tissue bruises, and performing primary surgical treatment if needed.
4. Neurological examination of the patient
Assessment of non-focal, focal, and meningeal symptoms is performed.
This stage enables preliminary topical diagnosis of brain injury to determine indications for neuroimaging studies. If the patient presents with non-focal, focal, or meningeal symptoms, neuroimaging is indicated.
5. Neuroimaging studies
Computed tomography (CT) of the brain is the “gold standard” in diagnosing traumatic brain injuries, including brain contusions.
The advantages of brain CT over other studies (including MRI) include the speed of the study, the ability to clearly assess the location, extent, and nature of brain injuries, the ability to assess associated bony structure injuries, and the possibility of rapidly scanning other body parts to exclude associated injuries.
Brain contusions on CT have several typical features:
Location of the contusion in cortical or basal brain regions;
The size of the contusion ranges from small hyperdense areas in the brain cortex to massive hyperdense areas;
Presence of a hypodense area around the contusion focus, which is explained by the initial formation of vasogenic edema followed by the addition of cytotoxic brain edema.
The characteristic density of hyperdense contusion foci on CT varies between 45–64 HU.
Magnetic resonance imaging (MRI) is generally not used in diagnosing brain contusions, though it may be applied to evaluate the progression of contusions. In brain contusions on MRI, the following are typical:
T1-weighted images: hyperintense signal;
T2-weighted images: hypointense signal;
SWI images: hyperintense signal.
6. Laboratory diagnostics
A complete blood count, urinalysis, coagulation profile, blood biochemistry, blood group, and Rh factor are necessary.
These tests do not confirm or suspect brain contusions, but they allow for the assessment of the patient’s overall condition, accompanying coagulation system disorders, and preparation for potential surgery.
Treatment of brain contusions
Medical therapy
Non-surgical treatment of brain contusions primarily involves maintaining adequate cerebral perfusion pressure, which may vary due to increased intracranial pressure (ICP) from developing or established contusion foci.
Anticonvulsant therapy: anticonvulsants are recommended only if there are symptoms of seizures. These medications are not recommended for preventive purposes.
In all patients with a GCS score below 8 when there is a substrate on CT or without it (in the presence of decerebration neurological symptoms), the installation of an intracranial pressure (ICP) sensor is indicated.
In cases of persistent intracranial pressure increase, ICP monitoring is used, and the following treatment is provided:
Sedative agents (in patients with traumatic brain injury, preference is given to propofol); Barbiturate derivatives in high doses are used only in case of refractory intracranial hypertension not responsive to non-surgical and surgical treatment;
Osmotic diuretics are used without ICP monitoring in the event of reported signs of life-threatening brain herniations and progressing neurological deterioration;
Hyperventilation;
Hypothermia.
Surgical Therapy
Surgical treatment of brain contusions primarily aims to reduce intracranial pressure to ensure adequate cerebral perfusion and prevent life-threatening brain displacement syndromes.
Indications for surgical treatment of brain contusions with supratentorial localization:
Contusion focus volume over 50 cm³;
Axial displacement of midline structures of 5 mm or more;
Compression of basal cisterns;
Compression of the third ventricle.
In this case, surgery is limited to performing a craniotomy and resection of brain contusion foci.
The indication for surgical treatment with intracerebral hematoma formation may be the following:
Hematoma volume of 40 ml in the frontal lobe of the brain;
Hematoma volume of 20 ml in the temporal lobe of the brain;
Axial displacement of 5 mm or more.
In this case, surgery also involves performing a craniotomy and resection of brain contusion foci.
In large contusions, progression of foci to surgically significant sizes, with an intracerebral hematoma volume of more than 140 ml, as well as with a patient consciousness level of less than 8 GCS points, decompressive craniotomy with resection of contusion foci is indicated.
Indications for surgical treatment of brain contusions with subtentorial localization:
Presence of a cerebellar contusion focus with a volume greater than 20 ml;
Signs of occlusive hydrocephalus;
Displacement of the fourth ventricle.
Surgical treatment tactics involve emptying and removing the contusion focus by craniotomy. In the absence of regression of occlusive hydrocephalus, the placement of an external ventricular drain is necessary.
FAQ
1. What is a brain contusion?
It is a type of focal traumatic brain injury where there is irreversible damage to brain parenchyma, forming foci of contusion, intracerebral hematomas, and edema.
2. How does a contusion differ from other forms of TBI?
Unlike concussion or diffuse axonal injury, brain contusions are characterized by morphologically confirmed tissue damage, visible on neuroimaging.
3. What are the main causes of contusions?
Traffic accidents, falls, violent injuries, and sports injuries.
4. How does a brain contusion develop?
By the mechanism of coup and countercoup: direct injury at the contact point with the injurious agent and secondary injury in the opposite area due to cavitation processes and pressure gradient changes.
5. What happens to brain tissue following a contusion?
Damaged cells release inflammatory mediators, free radicals, and enzymes, disrupting the blood-brain barrier, causing edema, and leading to neuronal and glial cell death.
6. Where are contusions most commonly located?
In the lower and inferolateral portions of the frontal and temporal lobes, due to skull anatomy and specific mechanical energy transmission.
7. What clinical signs are typical for contusions?
Non-focal symptoms (headache, vomiting, loss of consciousness) and focal ones, which depend on localization (aphasia, paresis, coordination disorders, visual disturbances).
8. How are brain contusions diagnosed?
Assessment of consciousness using the Glasgow Coma Scale, taking medical history, neurological examination, CT scan of the brain (gold standard), MRI if necessary, and laboratory tests to assess the patient’s general condition.
9. How are brain contusions treated without surgery?
Vital functions are supported, intracranial pressure is controlled, pain relief is provided, and if needed, anticonvulsant therapy, osmotic diuretics, hyperventilation, and hypothermia are used.
10. In what cases is surgical therapy necessary?
In case of large contusional foci, significant displacement of brain structures, extensive intracerebral hematomas, or signs of life-threatening complications.
11. What types of surgeries are used in severe injuries?
Craniotomy with the removal of the contusional focus, decompressive craniotomy, and external ventricular drainage (in cases of cerebrospinal fluid drainage impairment).
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Maës AIR, Menon DK, Manley GT. Traumatic brain injury: progress and challenges in prevention, clinical care, and research. Lancet Neurol. 2022;21(11):1004-1060. doi: 10.1016/S1474-4422(22)00309-X.
3.
Werner C, Engelhard K. Pathophysiology of traumatic brain injury. Prog Neurobiol. 2007;83(3):284-301. doi: 10.1016/j.pneurobio.2007.07.001.
4.
Freire MAM, et al. Cellular and molecular pathophysiology of traumatic brain injury: roles of brain edema, inflammation, excitotoxicity, and oxidative stress. Biology (Basel). 2023;12(8):1139. doi: 10.3390/biology12081139.
5.
Adatia K, Newcombe VFJ, Menon DK. Contusion progression following traumatic brain injury: a review of clinical and radiological predictors, and influence on outcome. Neurocrit Care. 2021 Feb;34(1):312-324. doi: 10.1007/s12028-020-00994-4.
6.
Jirlow U. Cerebral contusions – pathomechanisms, predictive factors, historical perspectives. Narrative review. Uppsala University; 2024.
7.
Khan MM, De Jesus O. Cerebral contusion. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023.
Available from: https://www.ncbi.nlm.nih.gov/books/NBK562147/
8.
Patel PP, et al. Decompressive craniectomy for traumatic brain injury. Review article. 2025.
9.
Habibi MA, et al. A comprehensive systematic review and meta-analysis: decompressive craniectomy versus craniotomy for acute subdural hematoma. Neurosurg Rev. 2024.
10.
Poblete RA, et al. Post-traumatic cerebral infarction: a narrative review of incidence, pathophysiology, diagnosis, and treatment. Medicines (Basel). 2024;16(1):6. doi: 10.3390/medicines16010006.
11.
Chen G, et al. An updated review for clinical and radiological predictors of traumatic brain injury outcomes. Review article. 2024.
12.
Wiles MD, et al. Management of traumatic brain injury: a narrative review of recent studies. Anaesthesia, 77(10), 1081–1088. 2022.
13.
Brain Trauma Foundation. Guidelines for the management of severe traumatic brain injury: revised guidelines and cost-benefit analysis. 2007.
14.
ACS Committee on Trauma. ACS TQP best practices guidelines: the management of traumatic brain injury. American College of Surgeons; 2024.
15.
Head trauma: background, pathophysiology, etiology. eMedicine [Internet]. Medscape; 2024.
Available from: https://emedicine.medscape.com/article/433855-overview
St. Petersburg FL 33702, 7901 4th St N STE 300, USA
Thank you!
Your message is sent! Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io
Cookie Consent
We use cookies to enhance your browsing experience, analyze site traffic, and deliver content. Please choose whether you accept all cookies or wish to reject non-essential tracking.
Cookie Preferences
Manage your cookie preferences below:
Essential cookies enable basic functions and are necessary for the proper function of the website.
Name
Description
Duration
Geolocation Config
This cookie is used to store the consent settings based on the visitor's location.
30 days
Cookie Preferences
This cookie is used to store the user's cookie consent preferences.
30 days
Google reCAPTCHA helps protect websites from spam and abuse by verifying user interactions through challenges.
Name
Description
Duration
_GRECAPTCHA
Google reCAPTCHA sets a necessary cookie (_GRECAPTCHA) when executed for the purpose of providing its risk analysis.
179 days
Statistics cookies collect information anonymously. This information helps us understand how visitors use our website.
Google Analytics is a powerful tool that tracks and analyzes website traffic for informed marketing decisions.
ID used to identify users for 24 hours after last activity
24 hours
_gat
Used to monitor number of Google Analytics server requests when using Google Tag Manager
1 minute
_gac_
Contains information related to marketing campaigns of the user. These are shared with Google AdWords / Google Ads when the Google Ads and Google Analytics accounts are linked together.
90 days
__utma
ID used to identify users and sessions
2 years after last activity
__utmt
Used to monitor number of Google Analytics server requests
10 minutes
__utmb
Used to distinguish new sessions and visits. This cookie is set when the GA.js javascript library is loaded and there is no existing __utmb cookie. The cookie is updated every time data is sent to the Google Analytics server.
30 minutes after last activity
__utmc
Used only with old Urchin versions of Google Analytics and not with GA.js. Was used to distinguish between new sessions and visits at the end of a session.
End of session (browser)
__utmz
Contains information about the traffic source or campaign that directed user to the website. The cookie is set when the GA.js javascript is loaded and updated when data is sent to the Google Anaytics server
6 months after last activity
__utmv
Contains custom information set by the web developer via the _setCustomVar method in Google Analytics. This cookie is updated every time new data is sent to the Google Analytics server.
2 years after last activity
__utmx
Used to determine whether a user is included in an A / B or Multivariate test.
18 months
_ga
ID used to identify users
2 years
_gali
Used by Google Analytics to determine which links on a page are being clicked
30 seconds
Clarity is a web analytics service that tracks and reports website traffic.