The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Phlebothrombosis is the formation of a blood clot in the venous system, most commonly the deep veins of the lower extremities, with partial or complete disruption of blood flow. The term deep vein thrombosis (DVT) is often used in the international literature.
Epidemiology
The main cause of a blood clot formation is a disorder in one of the factors of Virchow’s triad: blood stasis, damage to the vascular wall, and hypercoagulability.
Causes of deep vein thrombosis
Etiologic factors can act individually or synergistically to lead to blood clot formation in the venous system.
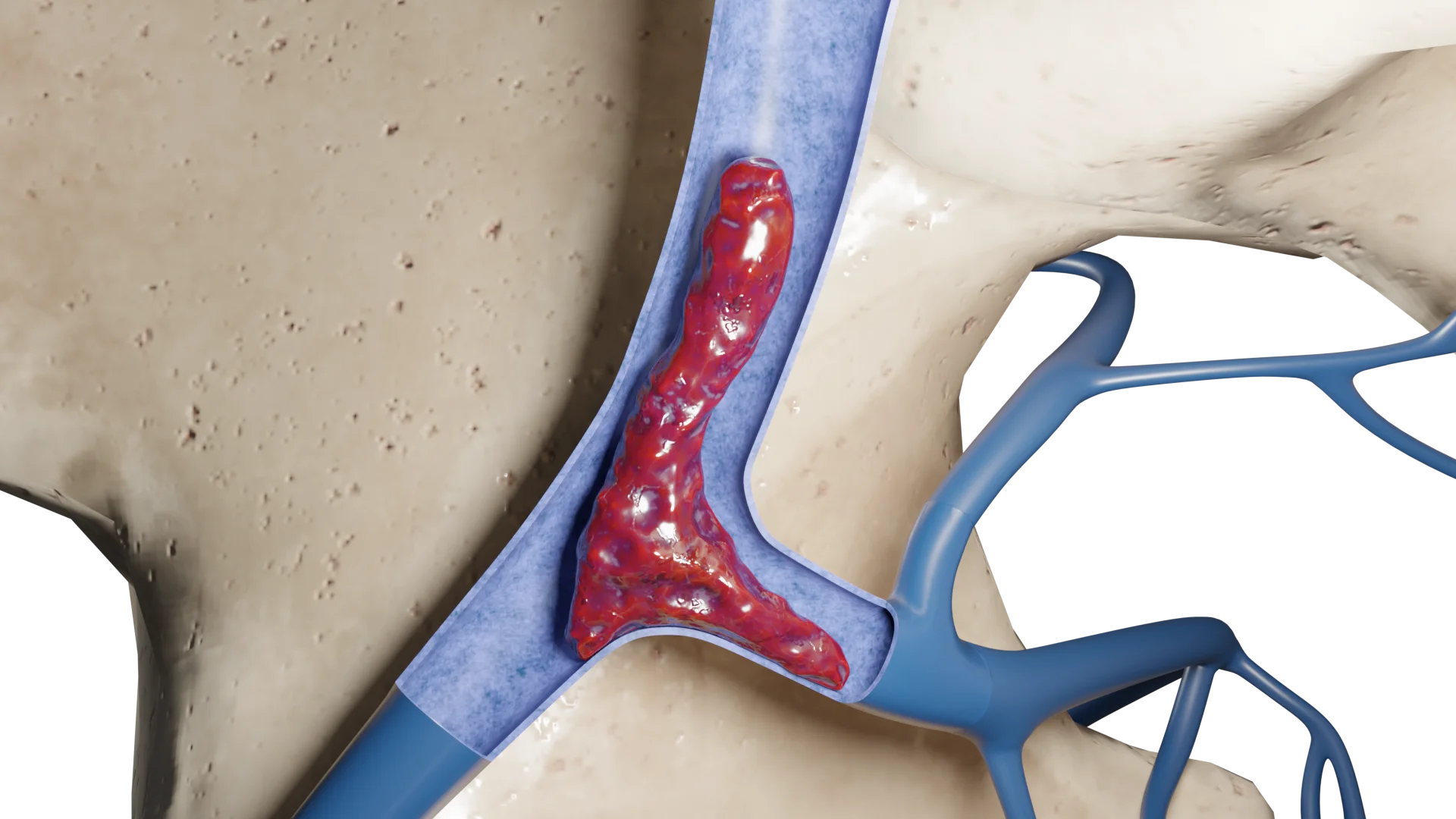
Blood clot formation begins with the activation of platelets and the coagulation cascade in response to damage to the vascular wall or blood stasis.
Stages of thrombosis
1. Platelet activation
Once the endothelium of the vein is damaged, platelets are activated and begin to adhere to the damaged area of the vascular wall. In this case, platelets:
Release substances that activate blood clotting (e.g., thromboxanes and serotonin).
Platelet activation promotes the release of adenosine diphosphate, which activates other platelets and increases aggregation.
A primary platelet plug forms, which begins to restrict blood flow in the injured area.
2. Activation of the coagulation cascade
Activation of the coagulation system leads to the formation of fibrin, the main component of the blood clot:
Thrombin, formed during coagulation activation, converts fibrinogen into fibrin, which forms a network that anchors platelets and stabilizes the plug.
This process occurs through several steps, including activation of clotting factors (V, VII, IX, X and prothrombin).
3. Primary and secondary blood clot formation
Primary blood clot: firstly, a fibrin-platelet plug forms, which is not structurally stable.
Secondary blood clot: the fibrin network stabilizes the clot. At this time, other blood components such as white blood cells and red blood cells begin to participate, resulting in a more organized and mature clot. The clot is thickened and better fixed in the vascular lumen.
4. The organization of the blood clot
Over time, fibroblasts and endothelial cells sprout into the clot, and collagen fibers are formed. This process can lead to the development of fibrosis and calcification of the blood clot, which can lead to chronic changes in the venous wall and the development of post-thrombotic syndrome.
5. Blood clot progression
The blood clot may spread proximally, increasing venous hypertension and impairing outflow.
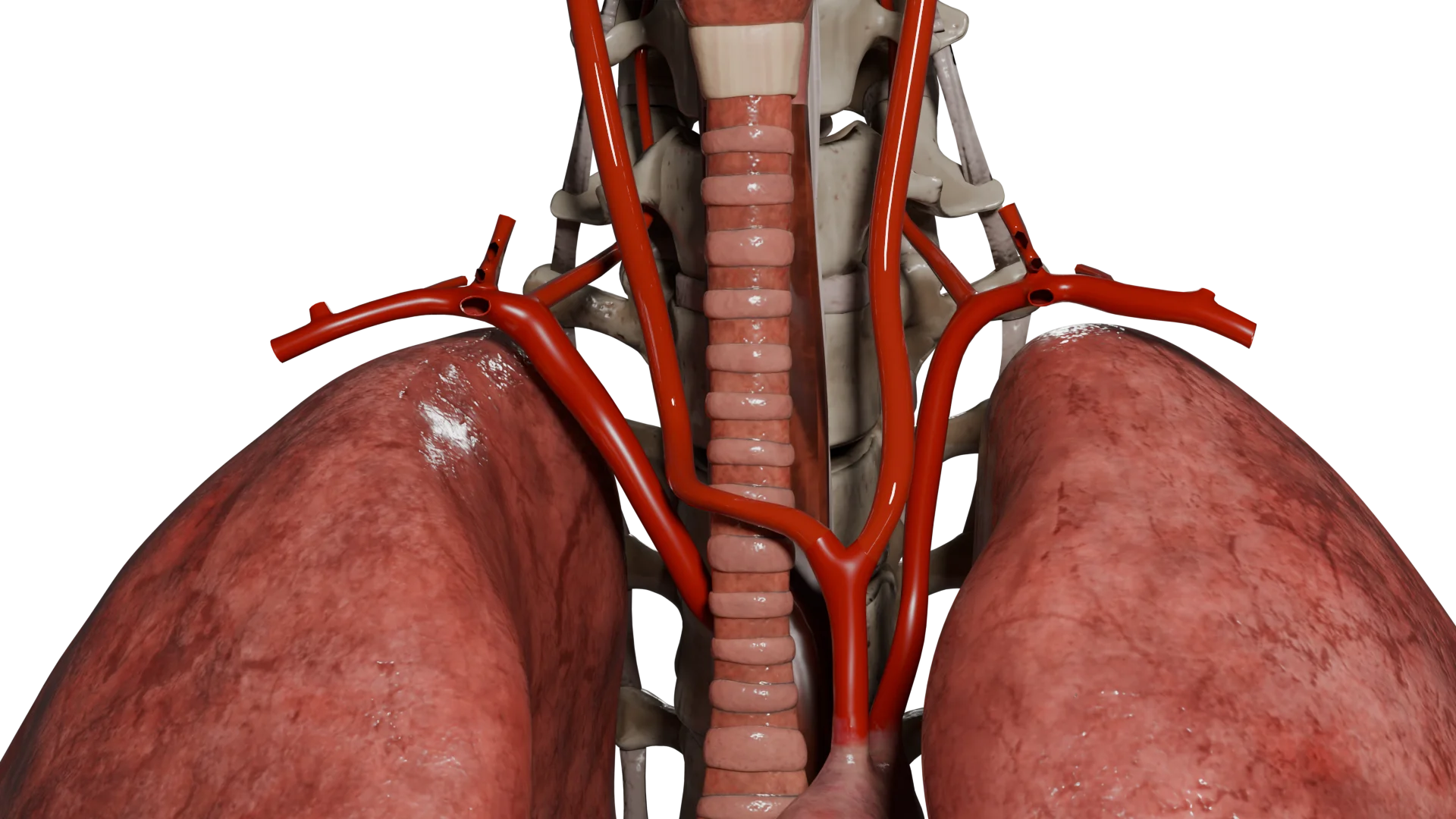
Its fragments (especially in the floating type of blood clot) can break off, entering the bloodstream and causing pulmonary embolism (PE), stroke, or infarction of internal organs.
In some cases, venous outflow is restored as a result of recanalization.
Phlebothrombosis is often asymptomatic and is detected only when complications develop, primarily pulmonary embolism.
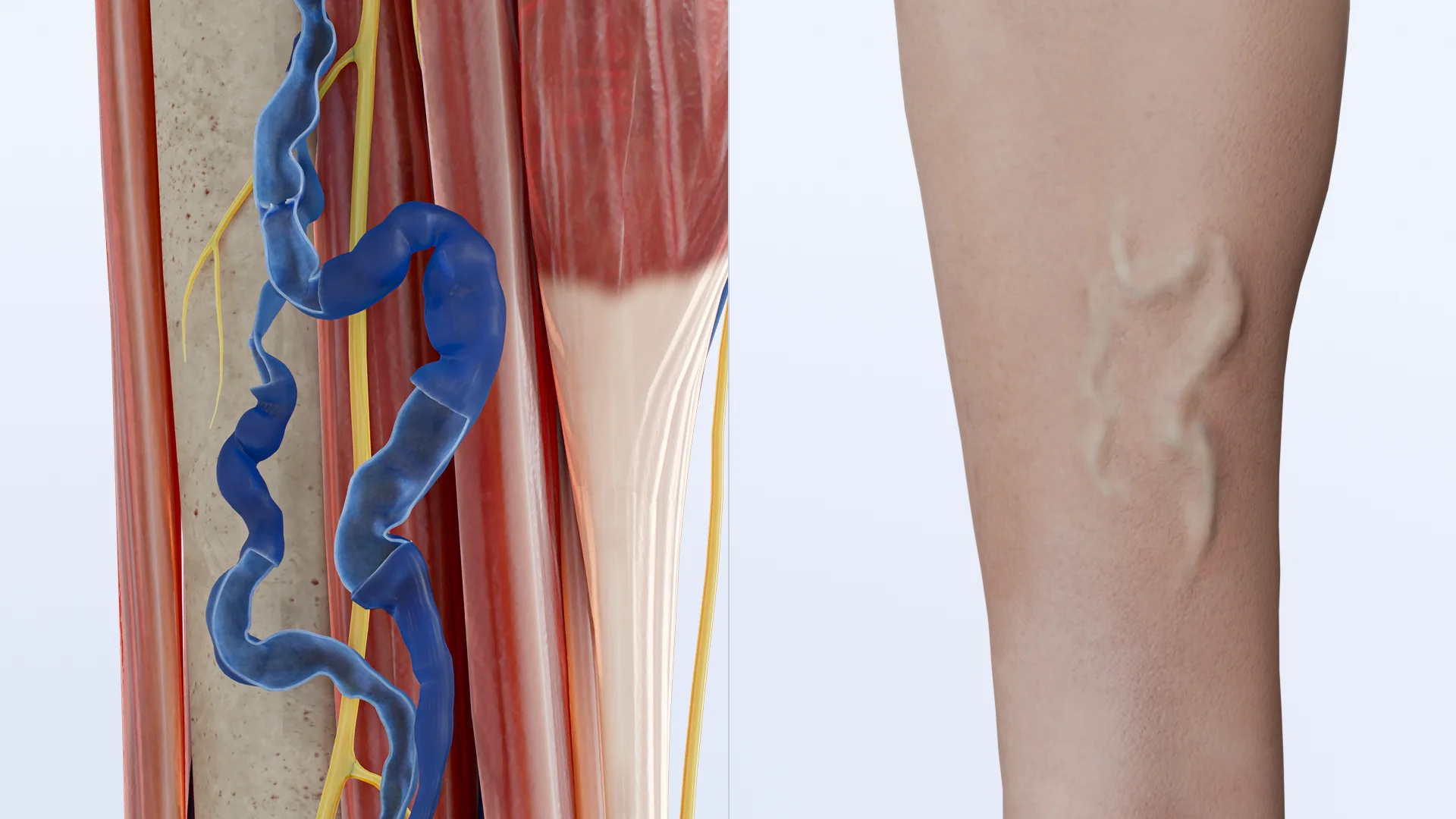
When symptoms are present, the leading signs are pain, swelling, and discoloration of the limb:
Pain: usually dull, pulling, worsens on exertion and palpation;
Edema: forms due to venous hypertension and is more often unilateral, involving the lower leg or the entire limb;
Skin discoloration: ranges from pallor to cyanosis, and, in massive thrombosis, marked venous stasis with threat of ischemia may occur.
These manifestations reflect impaired venous outflow and increased venous pressure.
Some patients have local hyperthermia and increased body temperature, which is associated with a systemic reaction to thrombosis. In rare cases, a severe course develops, blue phlegmasia (phlegmasia cerulea dolens), accompanied by sharp pain, massive edema and critical blood flow disruption.
Diagnosis of phlebothrombosis
Laboratory Methods
D-dimer detection is the primary screening test. A low level with a low to moderate clinical probability allows phlebothrombosis to be excluded. Its elevation is nonspecific and requires confirmation by imaging.
Coagulation profile (INR, PTT, prothrombin time) is used to evaluate the coagulation system and monitor anticoagulant therapy.
Thrombophilia screening (factor V Leiden mutation, protein C/S deficiency, antithrombin III, antiphospholipid antibodies) is performed for recurrent or unprovoked thrombosis when the result affects the duration of treatment.
Instrumental methods
Ultrasound duplex scanning is the method of choice. The diagnostic criterion is the absence of complete compression of the vein by the transducer; additional signs are visualization of echogenic masses and decreased blood flow.
CT and MR venography are used in cases of difficult visualization of pelvic veins or questionable ultrasound findings. They allow to accurately determine the localization and extent of the blood clot.
Phlebography is of limited use, mainly before interventional procedures.
Thus, the diagnosis of phlebothrombosis relies on a stepwise approach: clinical probability according to the Wells scale, laboratory screening by D-dimer and confirmation by instrumental methods, among which duplex scanning remains key.
Wells scale
Description
Score
Active cancer (treated in the last 6 months or continuous palliative therapy)
+1
Paralysis, paresis or recent immobilization of a limb
+1
Recent surgery (within 12 weeks) or immobilization for more than 3 days
+1
Soreness along the course of deep veins
+1
Swelling of the entire leg
+1
Tibial edema of more than 3 cm compared to the healthy tibia (measured 10 cm below the tibial tuberosity)
Presence of an alternative diagnosis more likely than DVT
-2
Probability of deep vein thrombosis:
Low: –2 to 0;
Moderate: 1 to 2;
High: >3.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Treatment of deep vein thrombosis
Prevention of phlebothrombosis
Prevention of thrombosis in at-risk patients is key. Early mobilization after surgery, adequate hydration, use of elastic compression during prolonged immobilization and flights are recommended. Prophylactic doses of anticoagulants (low-molecular-weight heparins or fondaparinux) are administered to high-risk patients in hospitals.
Medical Therapy
In the acute phase of phlebothrombosis, the key goal is to rapidly suppress the activity of the coagulation system to prevent thrombus growth and embolisation.
The following groups of parenteral anticoagulants are used for this purpose:
Low molecular weight heparins (LMWH) are the drugs of choice for starting therapy and are administered subcutaneously in therapeutic doses (e.g., enoxaparin, dalteparin).
Fondaparinux (a selective factor Xa inhibitor) may be used as an alternative to LMWH, especially when there are contraindications to heparin or a high risk of heparin-induced thrombocytopenia.
Unfractionated heparin is used less frequently, predominantly in patients with severe renal impairment or when rapid control (IV infusion with PTT monitoring) is required.
After 5–10 days of initial treatment, medications should be switched to oral anticoagulants:
Direct oral anticoagulants (DOACs): rivaroxaban, apixaban, dabigatran, edoxaban. They provide a stable anticoagulant effect and do not require routine monitoring.
Rivaroxaban and apixaban can be administered immediately after diagnosis, without an LMWH phase.
Dabigatran and edoxaban require a 5–7 day pretreatment with a parenteral anticoagulant.
Vitamin K antagonists (warfarin) are used if DOACs are contraindicated (e.g., severe renal failure, antiphospholipid syndrome, low drug availability). They require regular monitoring of INR (target values 2.0–3.0).
At least 3 months, followed by an assessment of the risk of recurrence; if the risk is high, an extension is recommended
Cancer patients
Prolonged anticoagulation preferably DOAC (apixaban, edoxaban) or LMWH
Recurrent thrombosis or severe thrombophilias
Lifelong therapy is often required
Surgical Therapy
Surgical and endovascular methods are used to a limited extent, in cases of massive ileofemoral thrombosis with the threat of ischemia or with a severe risk of post-thrombotic syndrome. The following are used:
Catheter-directed thrombolysis;
Pharmacomechanical thrombectomy;
Surgical thrombectomy for threatening conditions (e.g., phlegmasia cerulea dolens);
Placement of a cava filter is indicated only in contraindications to anticoagulation or recurrence of PE on adequate treatment.
FAQ
1. What is phlebothrombosis (deep vein thrombosis)?
Phlebothrombosis is the formation of a blood clot in the lumen of deep veins without significant inflammation of the wall, more often in the veins of the lower extremities.
2. How does phlebothrombosis differ from thrombophlebitis?
In phlebothrombosis, inflammation is minimal or absent, whereas in thrombophlebitis it is the leading process, usually in superficial veins.
3. What are the main causes of phlebothrombosis?
The key factors are venous stasis, endothelial damage and increased blood coagulation (Virchow’s triad). In the article, you can learn more about the etiologic factors.
4. What symptoms are most typical for deep vein thrombosis?
The most common symptoms are unilateral swelling, pain, a feeling of heaviness, and discoloration of the skin of the limb.
5. What is the danger of deep vein thrombosis, and what are its main complications?
The main immediate danger is pulmonary embolism (PE), a life-threatening condition in which a fragment of a blood clot breaks off and clogs the blood vessels of the lungs. The main long-term complication is post-thrombotic syndrome, which leads to chronic venous insufficiency, edema and trophic skin changes.
6. Does phlebothrombosis always have clinical manifestations?
No, in some patients the disease is asymptomatic and is detected accidentally or when complications develop.
7. Which laboratory test is most informative for deep vein thrombosis?
D-dimer: its low level with low clinical probability excludes thrombosis, while an elevated level requires confirmation by imaging.
8. Which method of instrumental diagnosis of phlebothrombosis is the “gold standard”?
Ultrasound duplex scanning of veins is the main method that allows to detect a blood clot and assess its extent.
9. What is the Wells scale and why is it needed?
This is a clinical scale to help assess the likelihood of thrombosis and determine if imaging should be done right away or if you should start with a lab test.
10. How is phlebothrombosis treated?
The basis of therapy is anticoagulants (LMWH, fondaparinux, direct oral anticoagulants, warfarin). In rare cases, endovascular or surgical interventions are used.
11. How long is deep vein thrombosis treated?
The duration of anticoagulant therapy is determined by the cause of thrombosis. For provoked thrombosis (e.g., after surgery), treatment duration is usually 3 months. For unprovoked or recurrent thrombosis, therapy may be extended or prescribed for life after risk assessment. In cancer patients, the treatment is also long-term.
12. Can phlebothrombosis be prevented?
Yes, prevention includes early mobilization, compression linen, and use of anticoagulants in high-risk patients.
References
1.
VOKA Catalogue. [Electronic resource].
https://catalog.voka.io/
2.
Kakkos, S. K., Gohel, M., Baekgaard, N., et al. (2021, January). Editor’s choice – European Society for Vascular Surgery (ESVS) 2021 clinical practice guidelines on the management of venous thrombosis. European Journal of Vascular and Endovascular Surgery, 61(1), 9–82. DOI: 10.1016/j.ejvs.2020.09.023.
3.
Wolf, S., Barco, S., Di Nisio, M., et al. (2024, September). Epidemiology of deep vein thrombosis. Vasa, 53(5), 298–307. DOI: 10.1024/0301-1526/a001145.
4.
Kim, K. A., Choi, S. Y., & Kim, R. (2021, June). Endovascular treatment for lower extremity deep vein thrombosis: An overview. Korean Journal of Radiology, 22(6), 931–943. DOI: 10.3348/kjr.2020.0675.
5.
Gil-Díaz, A., Martín Guerra, J., Parra Caballero, P., et al. (2024, May). Diagnosis and treatment of deep vein thrombosis of the lower and upper limbs: 2024 recommendations of the venous thromboembolism group of the Spanish Society of Internal Medicine. Revista Clínica Española (Barc), 224(5), 300–313. DOI: 10.1016/j.rceng.2024.04.004.
6.
Skeik, N., Smith, J. E., Jensen, J. D., et al. (2021, July). Literature review of distal deep vein thrombosis. Journal of Vascular Surgery: Venous and Lymphatic Disorders, 9(4), 1062–1070.e6. DOI: 10.1016/j.jvsv.2021.01.018.
7.
Lieberman, J. R. (2018, October). Deep vein thrombosis prophylaxis: State of the art. Journal of Arthroplasty, 33(10), 3107–3108. DOI: 10.1016/j.arth.2018.01.051.














.webp)

/aortic%20dissection_main.webp)



