The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Aortic dissection (dissection) is an acute condition characterized by rupture of the inner sheath (intima) of the aorta with subsequent penetration of blood into the middle layer (media) and formation of a false lumen. This condition is associated with a high risk of aortic rupture, acute organ ischemia and death and requires urgent diagnosis and treatment.
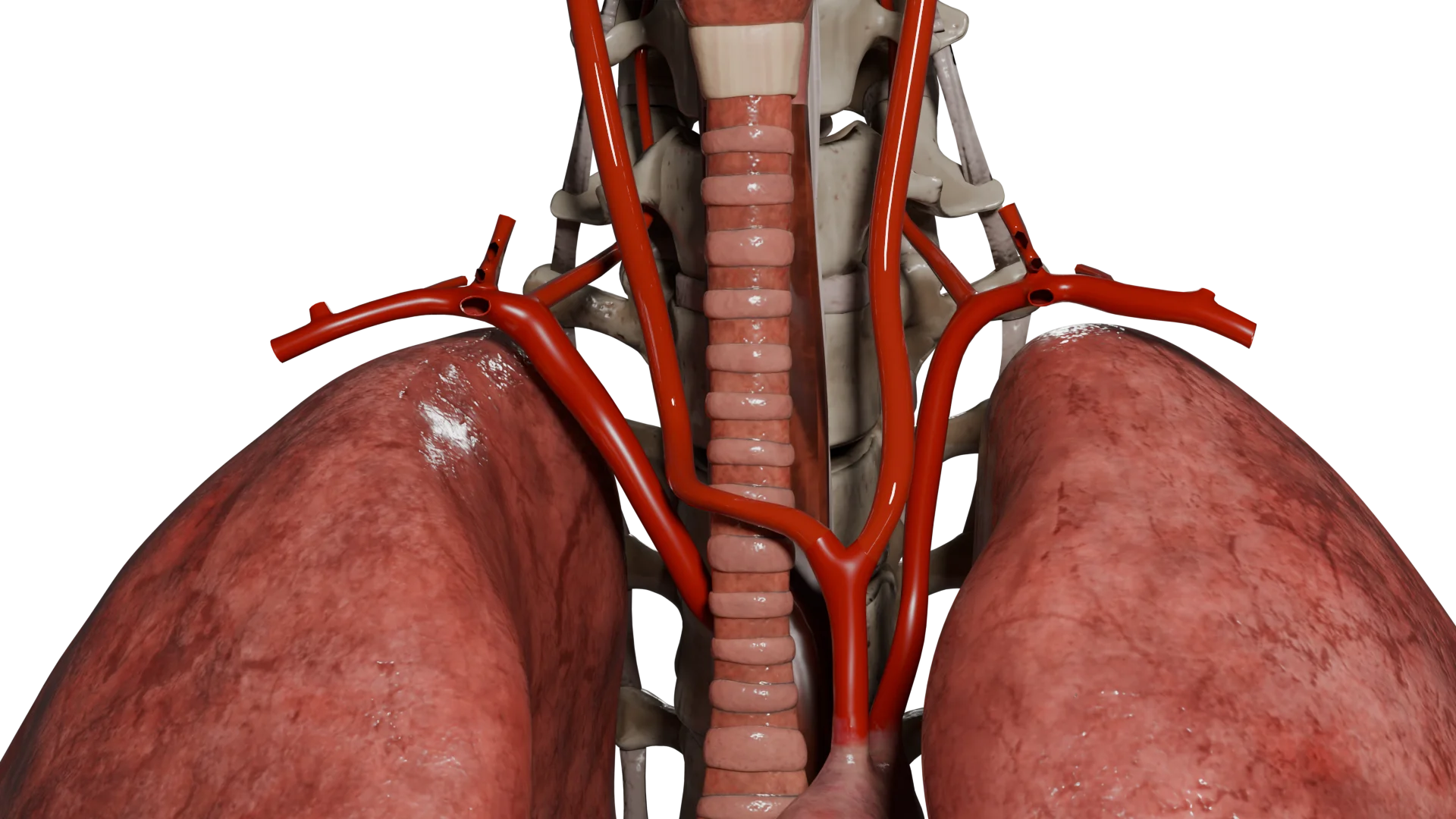
Ascending aortic dissection with involvement of aortic arch branches – 3D Model
Epidemiology
Frequency: 3-6 cases per 100,000 people per year. However, autopsy data suggest that the actual prevalence is higher.
Gender: Men are affected more often than women (≈2:1).
Age: Peak at 60-70 years (for sporadic forms); syndromic forms (e.g., in Marfan syndrome) at younger ages (20-40 years).
Geography/race: African Americans demonstrate earlier age of onset and higher mortality; incidence is higher in countries with poorly controlled arterial hypertension.
Etiology
Arterial hypertension is the main factor (up to 80% of cases).
Atherosclerosis: weakening of the intima due to inflammation and damage.
Inflammatory diseases (vasculitides) – for example, gigantocellular arteritis.
Infections (such as syphilis or mycotic lesions).
Pathogenesis
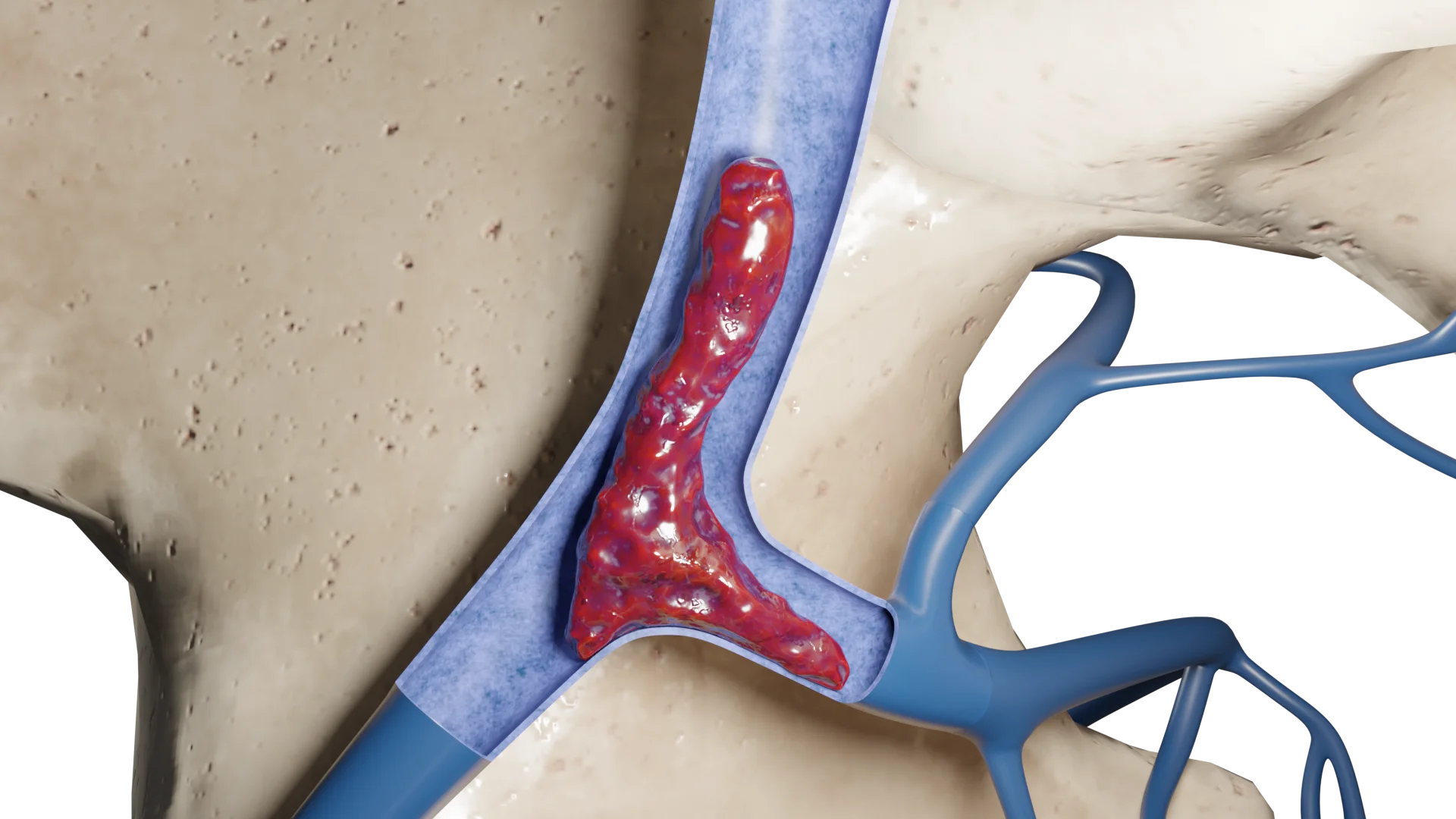
The primary link is rupture of the aortic intima due to high systolic pressure or disruption of the structural integrity of the wall.
Entry of blood into the media (middle layer) → formation of a false channel between the layers of the aortic wall.
The longitudinal spread of dissection is proximal or distal to the site of primary rupture, often involving aortic branches.
Flap of detached intima distal to the left subclavian artery orifice, false and true lumen – 3D Model
Possible Consequences:
Compression of the true lumen → ischemia of organs (kidneys, liver, intestines, limbs, brain).
If spread to the aortic root, it may cause acute aortic valve insufficiency or acute myocardial ischemia with involvement of the coronary artery orifices.
Rupture of the outer layer (adventitia) → massive bleeding into cavities (pericardium, pleura, retroperitoneum).
Formation of repeated inlets – maintains circulation in the false channel.
Markers of remodeling:
Activation of metalloproteinases (MMP-2, -9), collagen and elastin degradation.
Endothelial dysfunction and inflammatory response (TNF-α, IL-6).
Classification of aortic dissection
Stanford classification
Type A: affects the ascending aorta (with or without involvement of the aortic arch).
Type B: limited to the descending aorta.
Due to the fact that this classification did not take into account isolated lesions of the aortic arch or lesions of the arch in combination with the descending branch, the concept of a third type, Non-A non-A and non-B (non-A non-B), was proposed in 2019.
DeBakey classification
Type I: dissection from the ascending aorta to the aortic arch or below.
Type II: limited to the ascending aorta.
Type III: lesion of the descending aorta only (IIIa – up to the diaphragm, IIIb – spreading below).
Symptomatology depends on the localization of the dissection, the degree of involvement of aortic branches and the presence of complications.
Acute pain: sharp, retching, “dagger” pain, may be migratory, localization depends on the location of the dissection (type A: chest or back pain; type B: low back or abdominal pain).
Hypotension or shock with massive bleeding.
Asymmetry of pulse and BP in the arms.
Neurological disorders: weakness, loss of consciousness, symptoms of cerebral ischemia.
Cardiac tamponade with bleeding into the pericardial cavity.
Acute limb ischemia due to arterial occlusion.
Diagnosis
Physical examination (BP difference at the extremities; pulse deficit; aortic regurgitation murmur).
Lab Tests:
Elevation of D-dimer levels in the first few hours.
Biomarkers of myocardial injury (troponin, CK-MB).
Renal, liver enzymes, lactate – in organ ischemia.
General and biochemical blood tests – anemia, inflammation.
Instrumental studies:
CT angiography (gold standard): high sensitivity and specificity (>95%). Rapid and accurate detection of dissection, identification of false and true channels, primary inlet, extent of dissection, areas of malperfusion.
Transesophageal ultrasound: High sensitivity, especially for type A. Allows evaluation of the intimal flap, size of the ascending aorta, aortic insufficiency, signs of ischemia, pericardial effusion.
MRI: An alternative to CT for chronic stratification or contraindications to contrast. High sensitivity, especially for assessing dynamics.
Treatment of aortic dissection
Conservative treatment (more common for type B):
Optimal antihypertensive, antianginal, and hypolipidemic therapy. In the acute period, constant monitoring in intensive care.
β-blockers (esmolol, metoprolol) – first line: they reduce HR and dp/dt (decrease the force and velocity of blood hitting the wall).
Sodium nitroprusside, uropidil, clonidine, nitroglycerin – BP reduction (after β-blockers) to 100-120 mmHg. Art.
Morphine – anesthesia and decreased sympathetic activation.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Surgical treatment (more common for type A):
Open surgery (usually using a ventilator and hypothermia techniques).
The affected segment of the aorta is resected with subsequent suturing of the prosthesis.
If the aortic arch is involved, the brachiocephalic arteries are reimplanted into the prosthesis (if the brachiocephalic arteries themselves are involved in the dissection process, they are also prosthetized).
If the dissection spreads to the aortic valve, aortic valve replacement is performed, and in some cases valve-preserving surgery is possible.
If spread to the coronary artery orifices, reimplantation or aortocoronary bypass surgery may be performed.
When spreading to the arch and descending branch, a hybrid prosthesis (Frozen Elephant Trunk) is possible in some cases.
Endovascular intervention (TEVAR): Placement of a stent graft to isolate a false lumen (especially in organ malperfusion). Suitable for stable patients with complications or type B with uncontrolled hypertension/pain and/or at risk of rupture.
In case of aortic rupture or cardiac tamponade, immediate surgery is required.
FAQ
1. How does an aortic dissection differ from an aneurysm?
An aneurysm is an enlargement of the wall of the aorta, and a dissection is a tear in its inner layer where blood gets trapped between the layers of the wall, creating a false channel.
2. What are the first symptoms of aortic dissection?
The most characteristic symptom is a sudden, tearing pain in the chest or back, often “migrating”. Fainting, numbness of the limbs, shortness of breath, weakness, or stroke symptoms may occur.
3. How dangerous is aortic dissection?
It’s a life-threatening condition. Without treatment, mortality in ascending aortic dissection (type A) reaches 50% in the first 48 hours. Timely intervention significantly reduces the risks.
4. Who is at risk?
Patients with arterial hypertension, Marfan syndrome, aortic aneurysm, close cases of dissection, pregnant women (in the third trimester), smoking men over 60 years of age.
5. Is surgery necessarily necessary?
If the ascending aorta is involved (type of A) – surgery is almost always necessary. In dissection of the descending aorta (type of B) surgery is only necessary if there are complications (pain, ischemia, rupture, etc.).
6. What pressure is considered safe?
Target level: systolic BP <120 mmHg, pulse rate 50-60 beats per minute. Beta-blockers are first-line drugs for lifelong control.
7. Can my relatives be at risk?
Yes, especially if you have an inherited connective tissue disorder (Marfan syndrome, Loeys-Dietz, etc.). Genetic counseling and routine screening ultrasound or CT scan for the next of kin is recommended.
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Reed MJ. Diagnosis and management of acute aortic dissection in the emergency department. Br J Hosp Med (Lond). 2024 Apr 30;85(4):1-9. doi: 10.12968/hmed.2023.0366.
3.
Hameed I, Cifu AS, Vallabhajosyula P. Management of Thoracic Aortic Dissection. JAMA. 2023 Mar 7;329(9):756-757. doi: 10.1001/jama.2023.0265.
4.
Tchana-Sato V, Sakalihasan N, Defraigne JO. Aortic dissection. Rev Med Liege. 2018 May;73(5-6):290-295.
5.
JCS/JSCVS/JATS/JSVS 2020 Guideline on Diagnosis and Treatment of Aortic Aneurysm and Aortic Dissection. Circ J. 2023 Sep 25;87(10):1410-1621. doi: 10.1253/circj.CJ-22-0794.
6.
Zeng T, Shi L, Ji Q, Shi Y, Huang Y, Liu Y, Gan J, Yuan J, Lu Z, Xue Y, Hu H, Liu L, Lin Y. Cytokines in aortic dissection. Clin Chim Acta. 2018 Nov;486:177-182. doi: 10.1016/j.cca.2018.08.005.
St. Petersburg FL 33702, 7901 4th St N STE 300, USA
Thank you!
Your message is sent! Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io
Cookie Consent
We use cookies to enhance your browsing experience, analyze site traffic, and deliver content. Please choose whether you accept all cookies or wish to reject non-essential tracking.
Cookie Preferences
Manage your cookie preferences below:
Essential cookies enable basic functions and are necessary for the proper function of the website.
Name
Description
Duration
Geolocation Config
This cookie is used to store the consent settings based on the visitor's location.
30 days
Cookie Preferences
This cookie is used to store the user's cookie consent preferences.
30 days
Google reCAPTCHA helps protect websites from spam and abuse by verifying user interactions through challenges.
Name
Description
Duration
_GRECAPTCHA
Google reCAPTCHA sets a necessary cookie (_GRECAPTCHA) when executed for the purpose of providing its risk analysis.
179 days
Statistics cookies collect information anonymously. This information helps us understand how visitors use our website.
Google Analytics is a powerful tool that tracks and analyzes website traffic for informed marketing decisions.
ID used to identify users for 24 hours after last activity
24 hours
_gat
Used to monitor number of Google Analytics server requests when using Google Tag Manager
1 minute
_gac_
Contains information related to marketing campaigns of the user. These are shared with Google AdWords / Google Ads when the Google Ads and Google Analytics accounts are linked together.
90 days
__utma
ID used to identify users and sessions
2 years after last activity
__utmt
Used to monitor number of Google Analytics server requests
10 minutes
__utmb
Used to distinguish new sessions and visits. This cookie is set when the GA.js javascript library is loaded and there is no existing __utmb cookie. The cookie is updated every time data is sent to the Google Analytics server.
30 minutes after last activity
__utmc
Used only with old Urchin versions of Google Analytics and not with GA.js. Was used to distinguish between new sessions and visits at the end of a session.
End of session (browser)
__utmz
Contains information about the traffic source or campaign that directed user to the website. The cookie is set when the GA.js javascript is loaded and updated when data is sent to the Google Anaytics server
6 months after last activity
__utmv
Contains custom information set by the web developer via the _setCustomVar method in Google Analytics. This cookie is updated every time new data is sent to the Google Analytics server.
2 years after last activity
__utmx
Used to determine whether a user is included in an A / B or Multivariate test.
18 months
_ga
ID used to identify users
2 years
_gali
Used by Google Analytics to determine which links on a page are being clicked
30 seconds
Clarity is a web analytics service that tracks and reports website traffic.

/aortic%20dissection_main.webp)
/aortic%20dissection_02%20(1).webp)
/aortic%20dissection_03%20(1).webp)
/aortic%20dissection_04%20(1).webp)
/aortic%20dissection_05%20(1).webp)
/aortic%20dissection_06%2B07%20(1).webp)