Fractures of the Scapula: Classification, Clinical Picture, Diagnosis, Treatment
Aleksandr K.Orthopedic surgeon, MD
19 min read·September 02, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Thescapula is a flat triangular bone with four large bones (scapular process, articular process (glenoid), acromial process, and beak process) located in the upper back, forming the posterior part of the shoulder girdle.
The scapula plays a key role in:
Arm movement: involved in rotation and retraction at the shoulder joint – 1/3 of the range of motion is scapulothoracic, 2/3 of the range of motion is brachiofemoral;
Shoulder stability: realized by the shoulder joint itself, as well as the scapulothoracic, acromial-clavicular joints and the upper shoulder support complex.
Epidemiology
Scapula fractures are a rare injury, accounting for less than 1% of all fractures and 3-5% of shoulder girdle injuries. They occur most often in young men (25-50 years of age).
Prevalence by fracture type:
Body of the scapula: the most frequent type, 50-60% of all cases.
Extra-articular glenoid fractures: 20-25%. Often combined with a clavicle fracture (flotation shoulder condition).
Intra-articular glenoid fractures: 10%.
Acromial outgrowth: approximately 8%.
Clavicular outgrowth: 3-5%.
Scapular awn: less than 2-3%.
Because of the high energy of impact, scapula fractures are often accompanied by other serious injuries.
Chest trauma (80%): often includes lung contusion (40%) and hemo/pneumothorax (more than 30%).
Fractures of bones of the shoulder girdle (50%), including the clavicle (25%).
Rib fractures (50%).
Head trauma (35-50%).
Spinal fractures (25-30%).
Pelvic fractures (15%).
Vascular and nerve damage to the arm (10%).
Etiology
Scapula fractures are almost always the result of high-energy trauma, most commonly road traffic accidents (80-90%). This is due to the fact that the bone is well protected by the surrounding muscles.
Basic mechanisms of damage:
Direct Injury: a severe blow delivered directly to the shoulder.
Indirect injury: transferring a blow through the arm (e.g., falling on an outstretched arm – FOOSH).
Fracture mechanisms for different parts of the scapula:
Body of the scapula: the result of a direct blow, fall, or compression.
Glenoid neck: the result of indirect trauma, most commonly a fall on an outstretched arm.
Intra-articular glenoid fractures: usually occur during anterior dislocation of the shoulder (much less commonly posterior dislocation, such as electrocution or epileptic seizure).
Acromial spur: the result of direct trauma; also possible stress fractures in athletes.
Clubbing: can be caused by direct trauma, sudden muscle contraction, or ligament tension from shoulder dislocation.
Scapular bone: result of direct trauma; in rare cases may be pathologic fracture due to tumor metastasis.
Classification of scapula fractures
Fractures of the scapula are classified mainly according to the anatomical location of the fracture. In addition, each fracture is classified according to common terminology according to the presence of fragments, the shape of the fracture line.
The following are the most commonly used classifications.
Hardegger classification
This is the simplest and most commonly used system based on the localization of the fracture (Hardegger classification).
Hardegger’s anatomic classification of scapula fractures
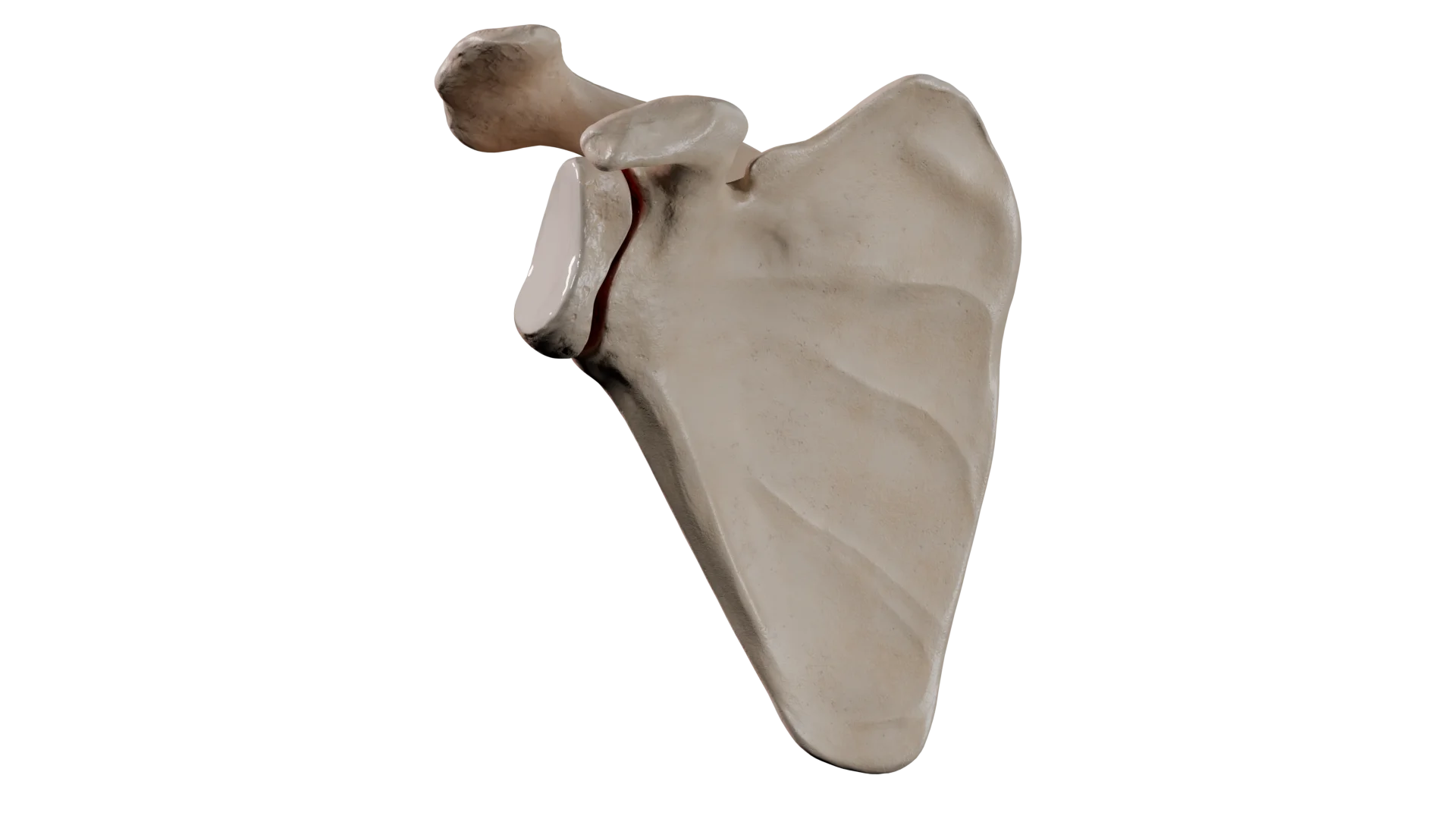
Type II: transverse fracture through the articular socket with extension to the neck of the scapula. In this type of fracture, the shoulder joint is unstable.
Type III: a rare oblique fracture passing through the upper part of the socket and extending to the body of the scapula.
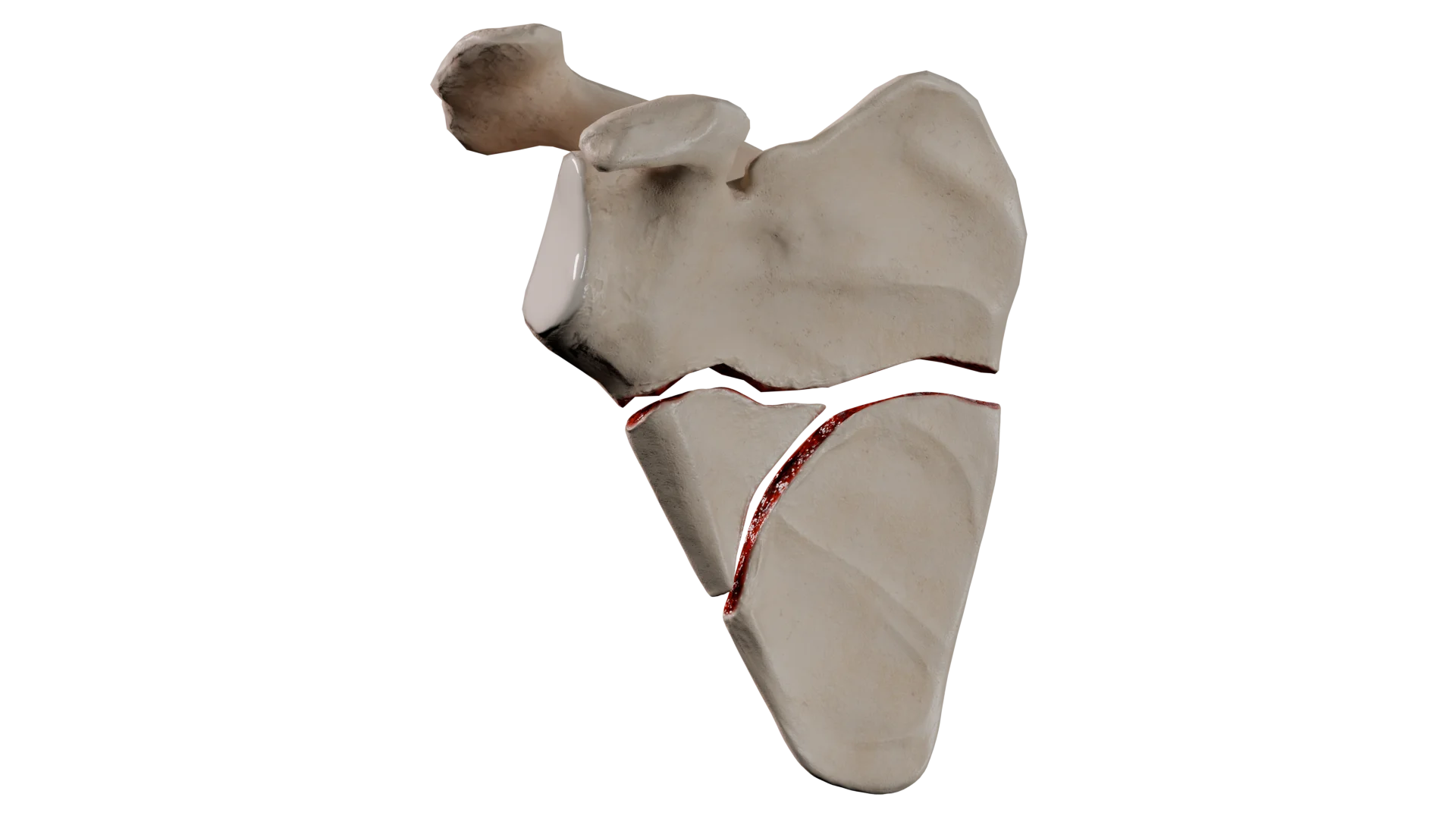
Type IV: transverse fracture extending to the medial edge of the scapula. It is the result of a high-energy impact.
Type V: a compound fracture, which is a combination of several types (II and IV, III and IV, or II, III and IV), divided into subtypes A, B, C. This fracture is extremely unstable. This fracture is highly unstable.
Type VI: severe multifocal injury to the entire articular process.
Kuhn classification of acromion fractures
Fractures of the acromial process of the scapula are classified according to the Kuhn classification. The classification identifies three types of fracture and determines treatment accordingly:
Type I: minimally displaced fracture not requiring surgical treatment.
Type II: displaced fracture without narrowing of the subacromial space. Both surgical and conservative treatment are possible for this type of fracture.
Type III: offsetfracture with narrowing of the subacromial space. This type of fracture requires surgical treatment.
Classification of fractures of the clavicular process
There are two main classifications for fractures of this area:
Ogawa classification
This classification (Ogawa classification) is based on the relationship of the fracture line to the attachment site of the clavicular ligaments:
Type I: the fracture line is proximal to the attachment site (base fracture);
Type II: the fracture line is distal to the attachment site of the clavicular ligaments.
This division is clinically and functionally justified. The first type of fracture is usually associated with instability of the upper shoulder support complex (SSSC).
Ayres classification
Eyres’ anatomical classification suggests 5 types of fracture:
Type I: fracture of the apex of the spinous process;
Type II: fracture of the middle segment of the ramus;
Type III: fracture of the base of the ramus;
Type IV: fracture involving the upper body of the scapula;
Type V: fracture with extension to the articular fossa of the scapula.
Comprehensive AO/OTA classification
Is a comprehensive and standardized classification of scaphoid fractures.
Diagnosis of scapula fractures
Diagnosis of scaphoid fractures is based on clinical evaluation and radial examination techniques.
Clinical evaluation
History: high-energy trauma or direct blow.
Examination: swelling, bruising, abrasions in the area of the scapula.
Palpation: localized soreness or step sensation subcutaneously.
Assessment of associated injuries: checking for chest, pelvic, head and spinal injuries or vascular and nerve injuries.
Radiologic diagnostics
Radiography: standard anteroposterior projection, lateral (Y-projection) and axillary projections of the shoulder.
CT (computed tomography) scan: provides detailed information, especially for intra-articular or complex fractures, and helps in preoperative planning.
Clinical Manifestations
Typical clinical pictureof a scaphoid fracture:
Symptoms: sharp pain in the shoulder or upper back, swelling and limited mobility of the shoulder.
Physical findings: visible swelling, soreness, crepitation (crunching) above the scapula, sometimes deformity.
Manifestations of concomitant trauma.
Treatment of scapula fractures
Due to the strong structure of the scapula and its protection by the surrounding muscles and thorax, many fractures are characterized by minimal displacement and can be treated conservatively. Fractures involving the articular socket that are significantly displaced and unstable usually require surgical treatment.
Conservative treatment
Conservative treatment is indicated for most fractures of the scapular body, spinous process, acromial and beak fractures without significant displacement. Intra-articular fractures of the articular socket with less than 2mm displacement and no shoulder instability can also be treated conservatively.
3D Animation: Scapula Body Fragmentation Fracture3D Animation: Fracture of the Neck of the Articular Process of the Scapula
Treatment consists of immobilization with a bandage for a period of 2-4 weeks. In order to prevent the development of adhesive capsulitis, early passive movements from the second week of injury, under pain control, are recommended. Active movements are allowed after 4 weeks of injury at the earliest. Healing is usually achieved within 6-12 weeks and is determined by the severity of the injury.
Surgical treatment
Surgical treatment is used in 10-20% of cases. Indications for surgery depend on the localization of the fracture and the degree of displacement.
Indications for surgical treatment of scaphoid fractures depending on localization
• Displacement of articular fragments > 2-4 mm • Involvement of articular surface > 20% • Recurrent shoulder dislocations after trauma
Acromial outgrowth
• Dislocation causing subacromial impingement • Progression of dislocation on control images
Beak-like process
• Instability of the upper shoulder support complex (SSSC) • Associated acromial-clavicular joint dislocation
Scapular awn
• Development of significant functional impairment
The technique for surgical treatment of a scaphoid fracture is as follows:
Open repositioning and internal fixation (ORIF) using plates and screws.
Arthroscopic fixation with sutures and screws for small articular socket fragments.
Early surgical treatment can improve functional outcome in appropriately selected patients.
Prognosis in scaphoid fracture
Scapula fractures generally have a high probability of fusion due to good blood supply and surrounding soft tissues. In most patients, shoulder function is fully restored. In cases of extensive soft tissue damage, the pain syndrome may persist for a long time.
Thus, fractures of the body of the scapula have an excellent prognosis. Fractures of the acromial and clavicular processes have a good prognosis. Glenoid neck fractures also have a generally favorable prognosis, but improper fusion may reduce shoulder strength and stability. Intra-articular glenoid fractures have a mixed prognosis. The outcome of the fracture may be posttraumatic osteoarthritis of the shoulder joint, instability of the joint, and restricted range of motion in the injured joint.
Timely diagnosis, comprehensive treatment of associated injuries, and patient compliance with rehabilitation programs are key to achieving optimal results.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Rehabilitation after scapula fracture
Although the process of fracture consolidation is favorable, restoration of full shoulder function is highly dependent on a structured and staged rehabilitation program.
The main goals of rehabilitation are:
Restoration of the volume of movement in the shoulder joint;
Restoring muscle tone;
Return to work and sports activity.
The basic principles of structured and sequential rehabilitation are as follows:
Initial immobilization to stabilize and heal the fracture.
Early mobilization.
Management of the effects of soft tissue injuries.
Progressive loading.
Stages of rehabilitation
The recovery program is divided into four sequential phases.
First stage (up to 2-3 weeks): immobilization of the injured limb is indicated. Active movements in uninvolved joints (hand, elbow) are allowed.
Early mobilization phase (3-6 weeks): early passive movements in the shoulder joint should be started, and isometric (static) exercises should be performed for the shoulder girdle muscles.
Functional recovery period (6-12 weeks): work begins to restore the full amplitude of active movements. Progressive loading of muscles using weights and expanders is introduced, avoiding forced movements.
Return to full activity (12+ weeks): consists of full recovery of lost endurance and strength through strength training, plyometric exercises and practicing activity-specific movements.
Expected recovery of full range of motion is expected by 3-4 months after injury. Symmetrical strength compared to the uninjured limb is usually restored by 4-6 months from the time of injury if all indicated rehabilitation measures are followed. Return to non-contact sports is allowed 3-4 months from the time of injury. Contact sports may be practiced after 6 months at the earliest.
FAQ
1. What are the dangers of a fractured scapula?
The main danger of scapula fracture is the high probability of damage to the chest organs, main vessels and nerves by bone fragments, as well as persistent impairment of the function of the upper limb on the side of the injury.
2. With which co-injury is a scapula fracture most commonly associated?
Since scapula fracture is a consequence of high-energy trauma, it is often accompanied by other injuries. The most common chest injuries are rib fractures with associated complications (pneumo/hemothorax, lung contusion), which occur in 80% of cases, as well as clavicle fractures and brachial plexus injuries, diagnosed in ~25% of cases.
3. When is standard radiography insufficient and a CT scan is required?
Computed tomography is necessary when an intra-articular or complex fragment fracture is suspected. CT provides detailed information on the degree of fragment displacement and is a key study for accurate preoperative planning.
4. How long does it take for a scaphoid fracture to heal?
The healing (consolidation) process of a scaphoid fracture usually takes 6 to 12 weeks. The time frame depends on the severity of the injury and the presence of associated injuries. Full functional recovery, including muscle strength, may take 4 to 6 months.
5. What are the main criteria for deciding on surgical treatment?
Surgical treatment is indicated in case of significant limb instability or displacement of the fragments. The key criteria are displacement of the glenoid articular fragments by more than 2-4 mm, displacement of the scapula body by more than 20 mm, angular deformity of more than 40°, and a “flotation shoulder” condition with concomitant clavicle fracture.
6. Which type of scaphoid fracture has the most equivocal prognosis?
Intra-articular fractures of the glenoid (joint socket) have the most ambiguous prognosis. The outcome of such injuries may be the development of post-traumatic arthrosis of the shoulder joint, chronic instability or permanent limitation of the range of motion.
7. What are the recommended timelines for immobilization and initiation of movement?
Immobilization of the limb is indicated for 2 to 4 weeks. To prevent the development of shoulder joint stiffness, it is recommended to start early passive movements from the second week, and active movements are allowed no earlier than 4 weeks after injury.
8. How long before the patient can return to sports?
Return to non-contact sports is possible after 3-4 months from the date of injury. Contact sports that require full power load can be practiced after 6 months at the earliest if rehabilitation is successful.
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io
2.
Lin IH, Lin TL, Chang HW, Lin CY, Tsai CH, Lo CS, Chen HY, Chen YW, Hsu CJ. Arthroscopy-Assisted Reduction and Internal Fixation versus Open Reduction and Internal Fixation for Glenoid Fracture with Scapular Involvement: A Retrospective Cohort Study. J Clin Med. 2022 Feb 21;11(4):1131.
3.
Sharifpour S, Mirghaderi P, Ghaseminejad Raeini A, Mirghaderi R, Moharrami A, Kalantar SH. Management of a floating shoulder accompanied by a scapular surgical neck fracture: a case report and review of the literature. Ann Med Surg (Lond). 2023 Mar 27;85(4):960-964.
4.
Matsuo T, Yoshikawa K, Oki S, Takeuchi D. Reconstruction surgery of intra-articular scapular fracture nonunion: a case report and literature review. JSES Rev Rep Tech. 2021 Oct 14;2(1):68-74.
5.
Berritto D, Pinto A, Russo A, Urraro F, Laporta A, Belfiore MP, Grassi R. Scapular fractures: a common diagnostic pitfall. Acta Biomed. 2018 Jan 19;89(1-S):102-110.
6.
Chen X, Deng YD, Qiu XS, Chen YX, Zhang ZT. Analysis of the curative effect and prognostic factors in patients with scapular fracture with surgical indications after conservative treatment: a case series and clinical outcomes. Quant Imaging Med Surg. 2023 Aug 1;13(8):5130-5140.
7.
Ogawa K, Inokuchi W, Honma T. Overlooked Fracture of the Inferior Scapular Angle Treated Conservatively. Case Rep Orthop. 2019 Jan 10;2019:9640301.
8.
Hefny AF, Mansour NA, Hefny MA, Masuadi E, Al Bahri S, Elkamhawy AA, Saber KS. Significance of Scapular Fracture Existence in Blunt Chest Trauma: A Retrospective Cohort Study. Surg Res Pract. 2024 May 20;2024:3550087.
9.
Chen L, Liu CL, Wu P. Fracture of the scapular neck combined with rotator cuff tear: A case report. World J Clin Cases. 2020 Dec 26;8(24):6450-6455.
10.
Neral M, Knapik DM, Wetzel RJ, Salata MJ, Voos JE. Scapular Body Fracture in the Athlete: A Systematic Review. HSS J. 2018 Oct;14(3):328-332.
11.
Chouhan V, Ladhania M, Vatsa A. Bilateral Scapular Fracture due to an Epileptic Seizure: A Case Report. J Orthop Case Rep. 2023 May;13(5):64-67.
12.
Ogawa K, Matsumura N, Yoshida A, Inokuchi W. Fractures of the coracoid process: a systematic review. JSES Rev Rep Tech. 2021 May 12;1(3):171-178.