Liver Сirrhosis: Etiology, Clinical Manifestations, Diagnosis and Treatment
Aleksandr F.Abdominal surgeon, MD
12 min read·July 29, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Liver cirrhosis is a generalized liver lesion characterized by the presence of parenchyma necrosis, diffuse fibrosis, the appearance of abnormal zones of liver tissue regeneration, resulting in disruption of the external and internal structure of the liver, as well as impairment of its function.
Classification of cirrhosis
By classification, cirrhosis of the liver can be divided according to the presence of structural changes, as well as stages of compensation.
By the presence of structural changes:
Small nodal (diameter of nodes from 3 mm to 1 cm);
Large nodal (node diameter greater than 1 cm);
Mixed;
Biliary.
3D Models of forms of liver cirrhosis according to the presence of structural changes:
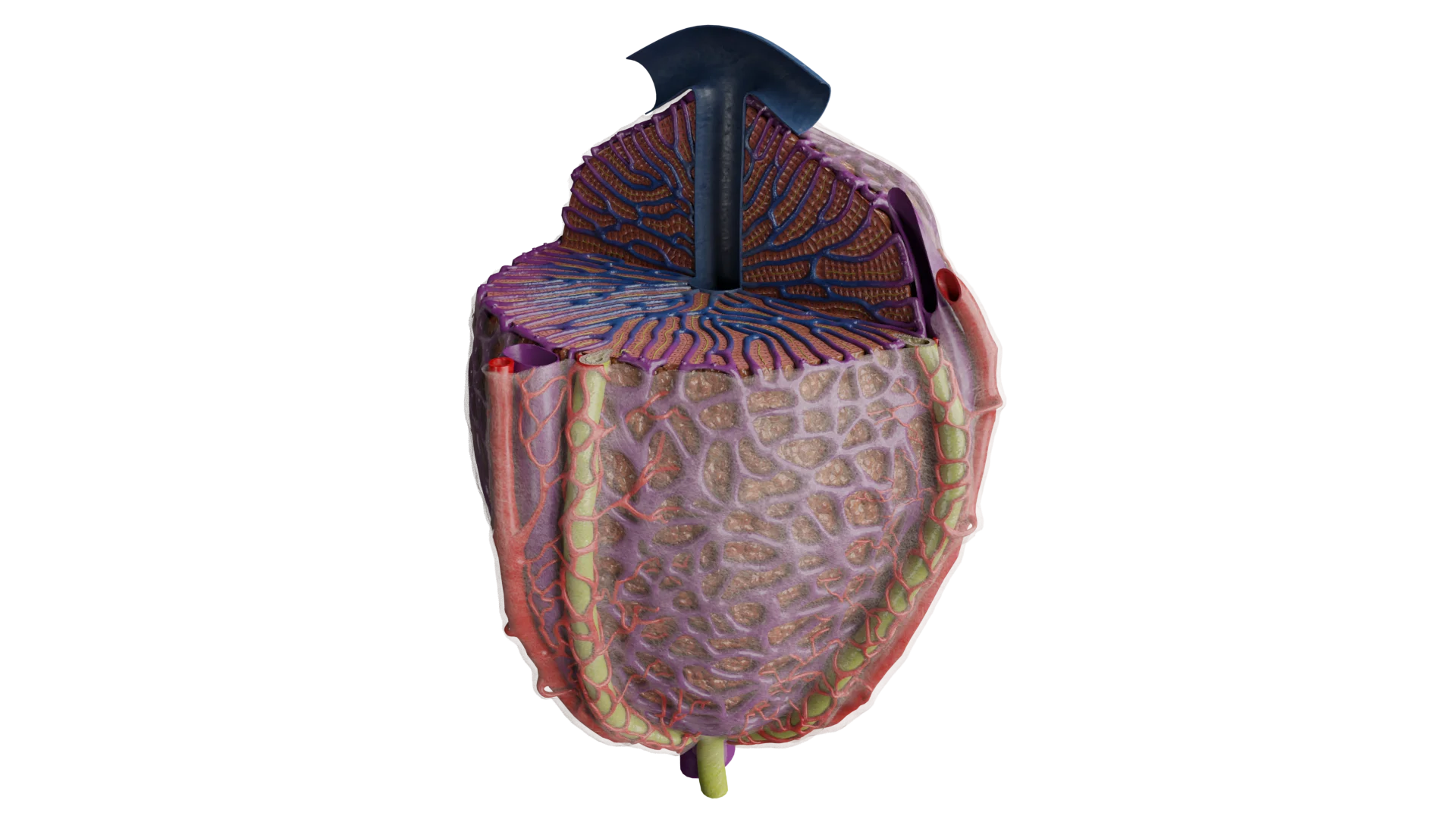
Small-nodal cirrhosis of the liver.
Large-nodal cirrhosis.
Mixed cirrhosis
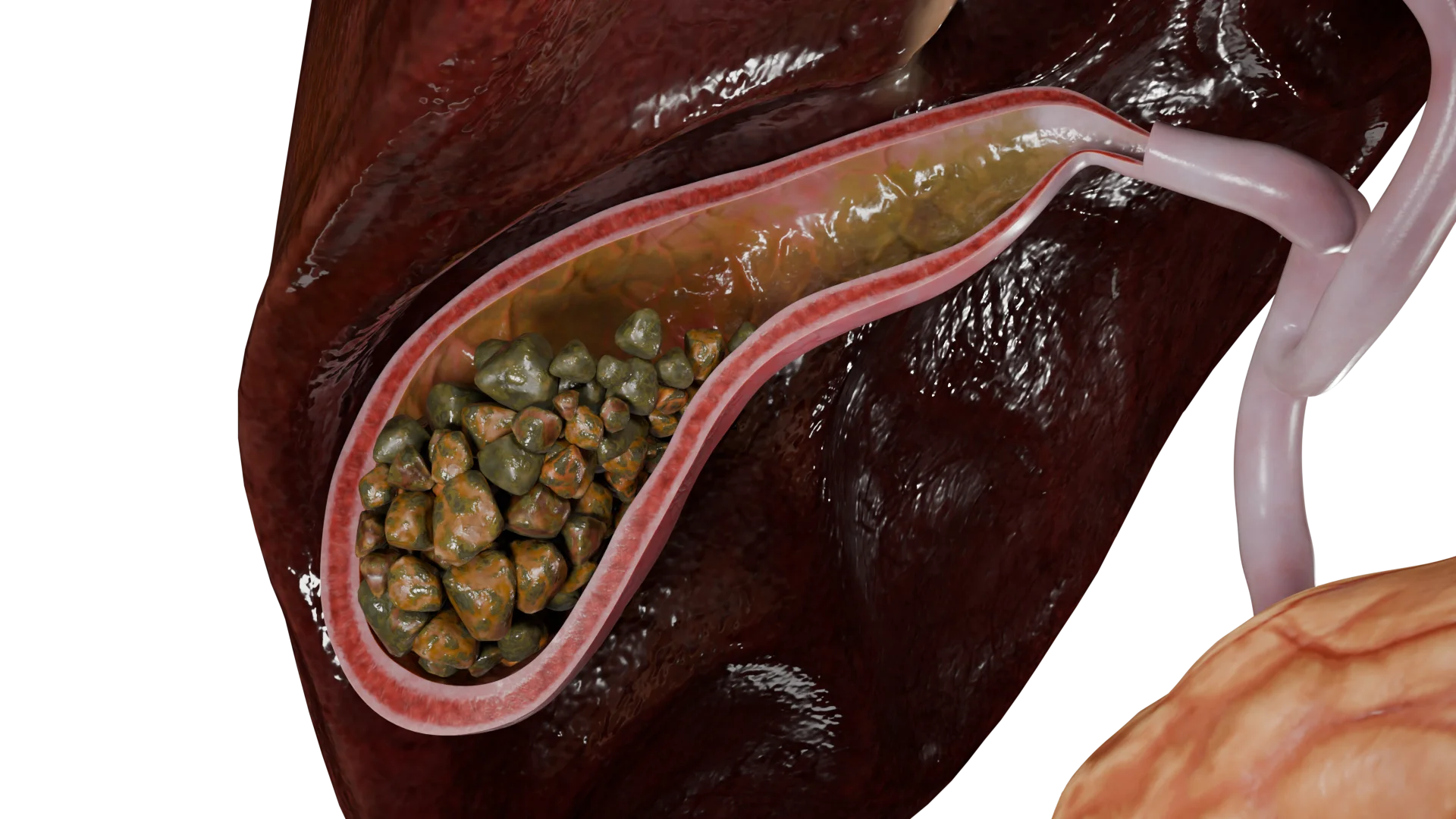
Biliary cirrhosis of the liver
By stages of compensation:
Compensated;
Subcompensated;
Decompensated;
Terminal.
There are clinical classifications that take into account clinical and laboratory manifestations (Child-Pugh).
According to the report of the European Association for the Study of the Liver, approximately 40% of liver transplants in Europe are performed for liver cirrhosis of viral etiology (viral hepatitis B, C, D), 33% – alcoholic, and 5% – due to a combination of these etiological factors.
Also the presence of autoimmune diseases or toxic effect of some drugs and systemic poisons affecting hepatic tissue contributes to the development of biliary cirrhosis associated with impaired outflow of bile through the intrahepatic and extrahepatic duct system.
Pathogenesis
The development of liver cirrhosis is based on direct damage to the hepatic lobule (structural and functional unit) by one of the etiologic factors.
The process of damage is long and can take a period of time from several months to several years. As a result of the lesion, areas of necrosis of hepatic parenchyma are formed. Around the areas of necrosis there are zones (nodules) of regeneration and chronic inflammation with the outcome in fibrosis.
In turn, regeneration nodules compress biliary tracts, which leads to congestion in the venous system of the liver with the formation of portal hypertension.
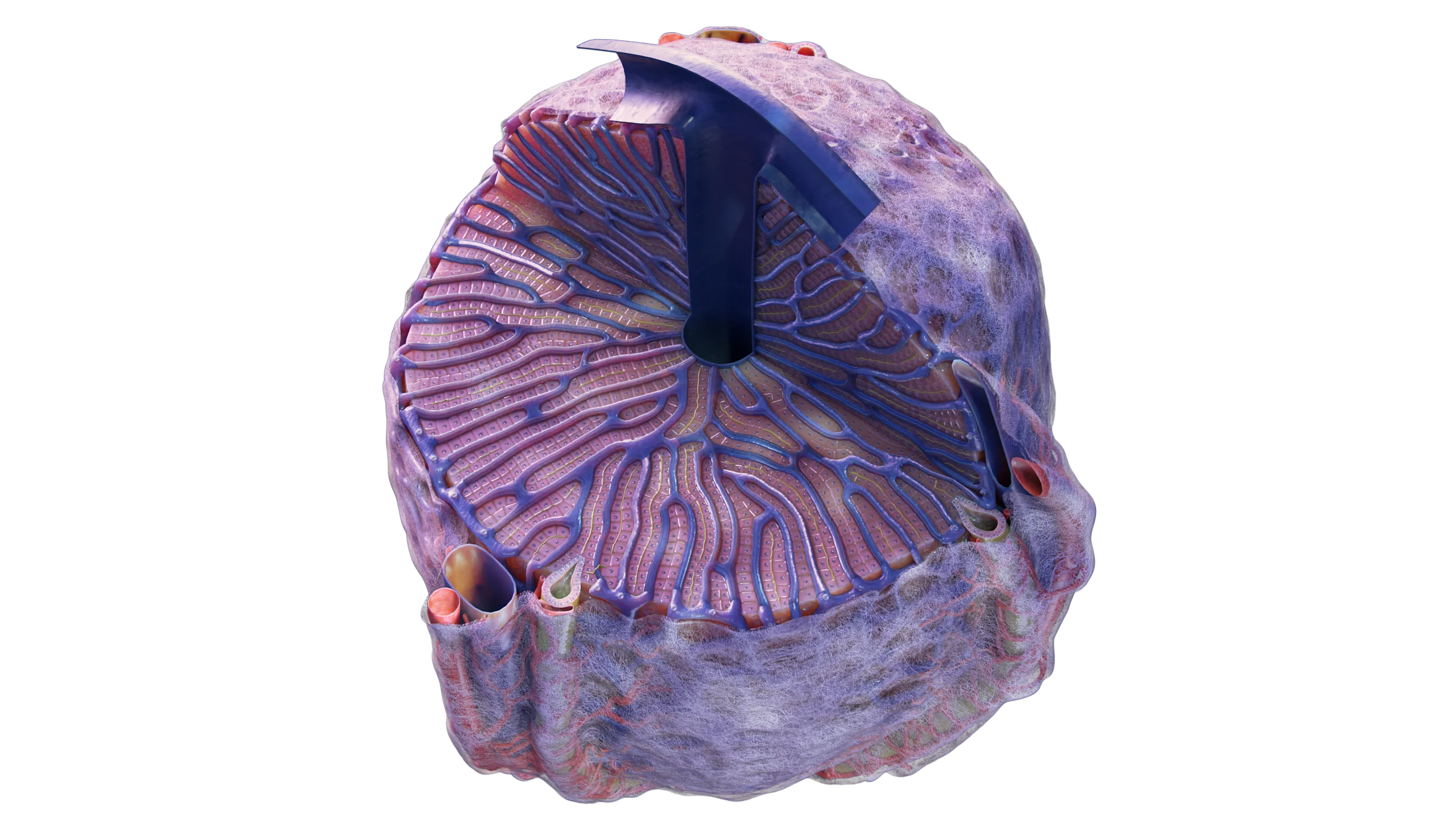
Structure of hepatic tissue (lobules, periportal tracts) – 3D Model
Clinical manifestations of liver cirrhosis
In the early stages of the disease, the disease may be asymptomatic.
With the progression of the disease, the following syndromes are distinguished:
A general syndrome characterized by weakness, headache, nausea, increased body temperature, arthralgia, a feeling of bitterness in the mouth, asthenia, and occasional abdominal pain;
Jaundice syndrome resulting from intrahepatic cholestasis (impaired bile outflow, increased blood concentration of direct bilirubin, increased concentration of bile acids). Increased concentration of bile acids in the blood is accompanied by pruritus;
Hepatomegaly and splenomegaly;
Portal hypertension syndrome occurs at the stage of decompensation. It is characterized by increased pressure in the portal vein system. Clinical manifestations of portal hypertension syndrome are: ascites, varicose veins of the esophagus, rectal veins, veins of the anterior abdominal wall. Often against the background of varicose veins bleeding occurs.
Abdominal appearance of a patient with liver cirrhosis: ascites and varices of the anterior abdominal wall – 3D Model
Pain syndrome arising against the background of biliary dyskinesia;
Liver encephalopathy, which occurs due to prolonged high concentrations of direct bilirubin. The latter, penetrating the blood-brain barrier, damages brain cells;
Violation of the synthetic and protective function of the liver.
It should be understood that the disease has stages and clinical manifestations will change with the progression of the disease. Thus, at the decompensation and terminal stages, not only the hepatobiliary system, but also other body systems (urinary, digestive, nervous, cardiovascular, etc.) are involved in the pathological process.
Diagnosis of liver cirrhosis
Diagnosis of the disease is based on the presence of clinical manifestations, etiologic factor, as well as instrumental and laboratory methods of investigation.
Instrumental methods of research
Ultrasound (fibroelastometry), Doppler ultrasound to assess blood flow in the portal vein system;
Computed tomography (CT) and magnetic resonance imaging (MRI);
Liver biopsy;
FGDS (fibrogastroduodenoscopy);
A review radiograph of the abdominal cavity.
Laboratory methods of research
Determination of antibodies to hepatitis B,C,D,E viruses;
Determination of alpha-fetoprotein in serum;
BAC (liver profile);
OAC;
Coagulogram;
OAM;
Determination of electrolyte composition.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Treatment of liver cirrhosis
Treatment of cirrhosis of the liver should be comprehensive and include the following measures:
Withdrawal from alcoholic beverages;
Diet (liver table), correction of electrolyte composition (sodium, potassium, chlorine), correction of protein imbalance;
Limiting medications that have hepatotoxicity.
Medical treatment
Infusion therapy (in the presence of symptoms of intoxication);
The use of ursodeoxycholic acid preparations;
S-adenosyl-L-methionine preparations;
Glucocorticosteroids;
Prevention of hemorrhagic complications;
Taking diuretics;
Treatment aimed at eliminating viruses tropic to hepatic tissue;
Treatment of associated pathology.
Surgical treatments include laparocentesis and liver transplantation.
Indications for liver transplantation are:
Presence of an irreversible pathologic process with a life prognosis of less than 12 months;
Lack of effect from conservative therapy;
Progressive cirrhosis with a life expectancy shorter than that of transplantation.
FAQ
1. What is cirrhosis of the liver in simple words?
Liver cirrhosis is an outcome of various chronic liver diseases in which normal liver cells are replaced by fibrous scar tissue, resulting in impairment of all functions of the organ.
2. How does cirrhosis of the liver manifest itself?
Liver cirrhosis may present with symptoms such as increased fatigue, nausea, bitterness in the mouth, abdominal pain (more often right subcostal), jaundice (yellowing of the skin and eyes), ascites (accumulation of fluid in the abdomen), and enlargement of the liver and spleen. In advanced stages of the disease, more severe symptoms develop, such as hepatic encephalopathy, bleeding, hepatarchy, and progressive liver failure, which can be fatal.
3. Can cirrhosis of the liver be cured?
Liver cirrhosis cannot be cured. However, in the early stages, with proper diet and treatment, it is possible to slow the progression of the disease and improve the quality and length of life.
4. How do you establish the presence of liver cirrhosis?
Diagnosis of liver cirrhosis is based on clinical manifestations, laboratory and instrumental methods of investigation, such as blood tests (general blood test, biochemical blood test, blood tests for viral hepatitis, etc.), abdominal ultrasound or CT scan, and in doubtful cases – liver biopsy.
5. What is the difference between liver cirrhosis and liver cancer?
Liver cirrhosis is a chronic liver disease associated with scarring of the liver tissue and impaired liver function, while liver cancer (hepatocellular carcinoma) is a malignant tumor.
6. What are the stages of cirrhosis of the liver?
Liver cirrhosis is divided into four stages depending on the degree of liver damage and organ function: compensated, subcompensated, decompensated and terminal.
7. Liver cirrhosis in women and men – are there differences?
Liver cirrhosis in women and men manifests similar symptoms, with hormonal disorders appearing earlier in women and symptoms of portal hypertension in men. From the peculiarities of origin, cirrhosis in women more often develops against the background of autoimmune diseases or exposure to toxins (alcohol), and in men more often against the background of viral hepatitis or alcoholism.
8. What are the dangers of cirrhosis of the liver?
Liver cirrhosis can cause a number of severe complications, including liver failure, portal hypertension, ascites, bleeding varices, and significantly increases the risk of hepatocellular carcinoma. In terminal stages, complications of cirrhosis can be fatal.
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Апросина З.Г.. Хронические диффузные заболевания печени (современные тенденции). Клиническая фармакология и терапия. №1. Том 5. 1996. С.14-18.
3.
Бакулин И.Г., Варламичева А.А. Гепаторенальный синдром: практические рекомендации по диагностике и лечению. Альманах клинической медицины. 2014, № 13, с 23-31.
4.
Ивашкин В.Т., Лапина Т.Л. Гастроэнтерология. Национальное руководство. – М.: ГЭОТАР-Медиа, 2015 – 480 с.
5.
Мехтиев С.Н., Гриневич В.Б., Чепур С.В., Ганчо В.Ю. Портальная гипертензия у больных хроническим гепатитом и циррозом печени. – СПб.: Бреста, 2004 – 320 с.
6.
Никитин И.Г., Сторожаков Г.И. Хронический гепатит С; актуальные вопросы диагностики и лечения. Клинические перспективы гастроэнтерологии, гепатологии. №3, 2001. С.7-11.
7.
Павлов Ч.С., Дамулин В.Д., Ивашкин В.Т. Печеночная энцефалопатия: патогенез, клиника, диагностика, терапия. РЖГГК 2016, 1, с 44-53.
8.
Пиманов С. Декомпенсированный цирроз печени: лечение с учетом международных рекомендаций. – М.: Практическая медицина, 2016 – 88 с.
9.
Юджин Р. Шифф, МайклФ. Соррел, УиллисС.Мэддрей. Болезни печени по Шиффу. Цирроз печени и его осложнения. Трансплантация печени// –М.: Изд. «ГЭОТАР- Медиа», 2012.
10.
Arroyo V., Moreau R., Jalan R., Ginès P. EASL-CLIF Consortium CANONIC Study Acute-on-chronic liver failure: A new syndrome that will re-classify cirrhosis // J. Hepatol. –2015 – Vol. 62 (Suppl.). – P. S131–S143.
11.
EASL Clinical Practice Guidelines: Wilson’s disease. J Hepatol. 2012 Mar; 56(3):671-85. European Association for the Study of the Liver. EASL Clinical Practice Guidelines on the management of hepatic encephalopathy // J. Hepatol. – 2022 – Vol. 77 –P. 807–824.
12.
European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Autoimmune hepatitis. Journal of Hepatology 2015 vol. 63(4): 971–1004.
13.
Sanyal A., Mullen K., Bass N. The treatment of hepatic encephalopathy in the cirrhotic patient. Gastroenterol Hepatol (NY) 2010; 6(4 Suppl. 8):1-12.