Aberrant Subclavian Artery: Etiology, Pathogenesis, Classification, Diagnosis, and Treatment
Oleg K.Cardiovascular surgeon, MD
10 min read·May 27, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Aberrant right subclavian artery (ARPA) is the most common aortic arch anomaly, occurring in approximately 0.5-2% of the population. The vast majority of cases involve the aberrant right subclavianartery (arteria lusoria). The anomaly can be detected at any age, but is more commonly diagnosed either in childhood in the presence of symptoms or incidentally in adults on imaging studies.
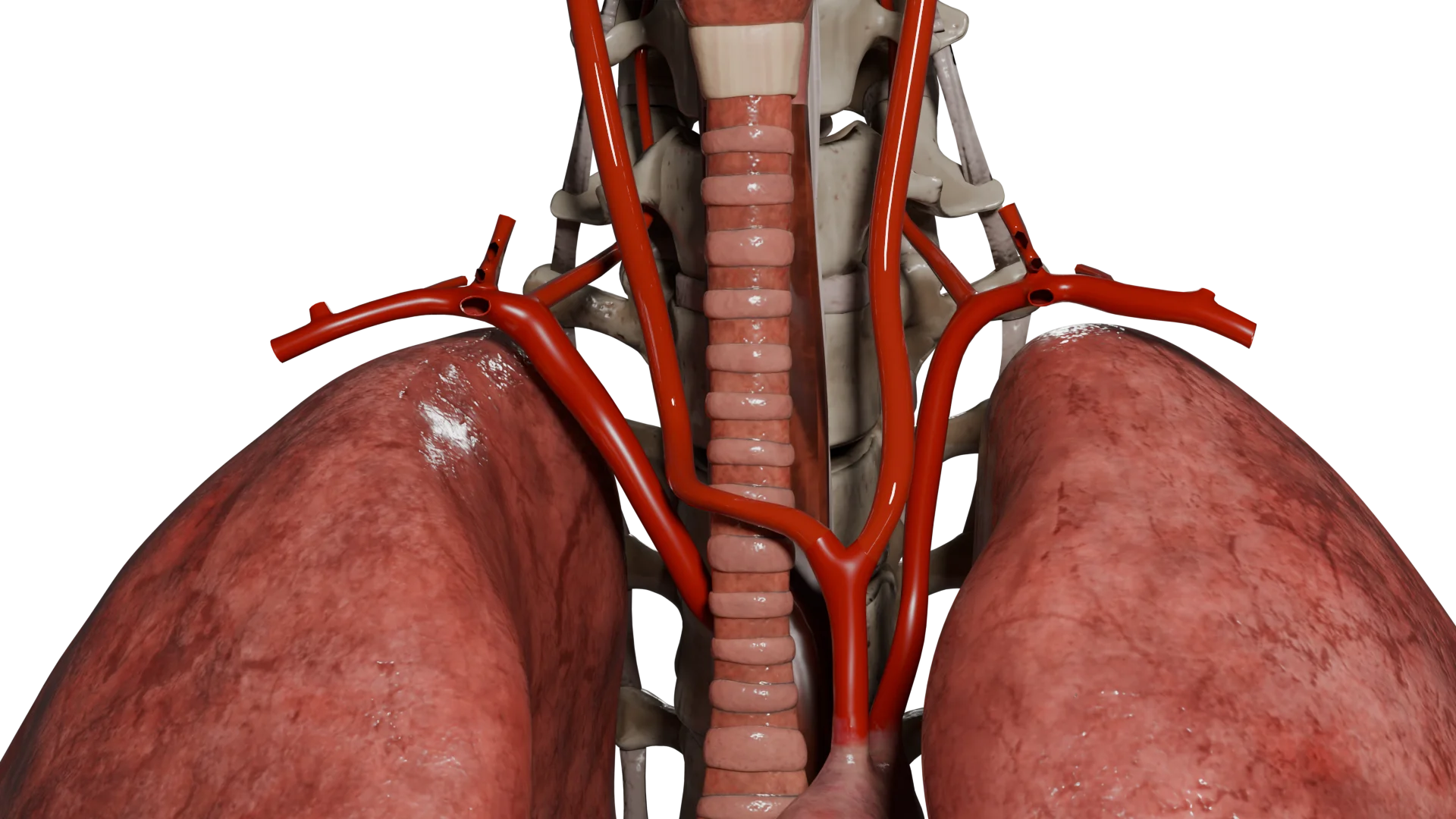
Aberrant right subclavian artery in combination with bicarotid trunk (left and right common carotid arteries branch from the aortic arch with a single trunk) – 3D Model
Etiology
ARPA is the result of abnormal embryologic development of the 4th and 7th interaortic arches. The main cause is the preservation of the right 7th interaortic arch with regression of the right 4th arch, resulting in the right subclavian artery branching off the distal aorta, most often after the left subclavian artery, and passing behind the esophagus.
Risk Factors:
Genetic abnormalities (e.g., 22q11.2 deletion);
Syndromes with vascular malformation (Di Giorgi, Turner);
It is often combined with congenital heart defects (tetrada Fallo, transposition of the main vessels);
Hereditary predisposition is possible, especially when a similar anomaly is present in first-degree relatives.
3D-animation – aberrant right subclavian artery combined with bicarotid trunk
Pathogenesis
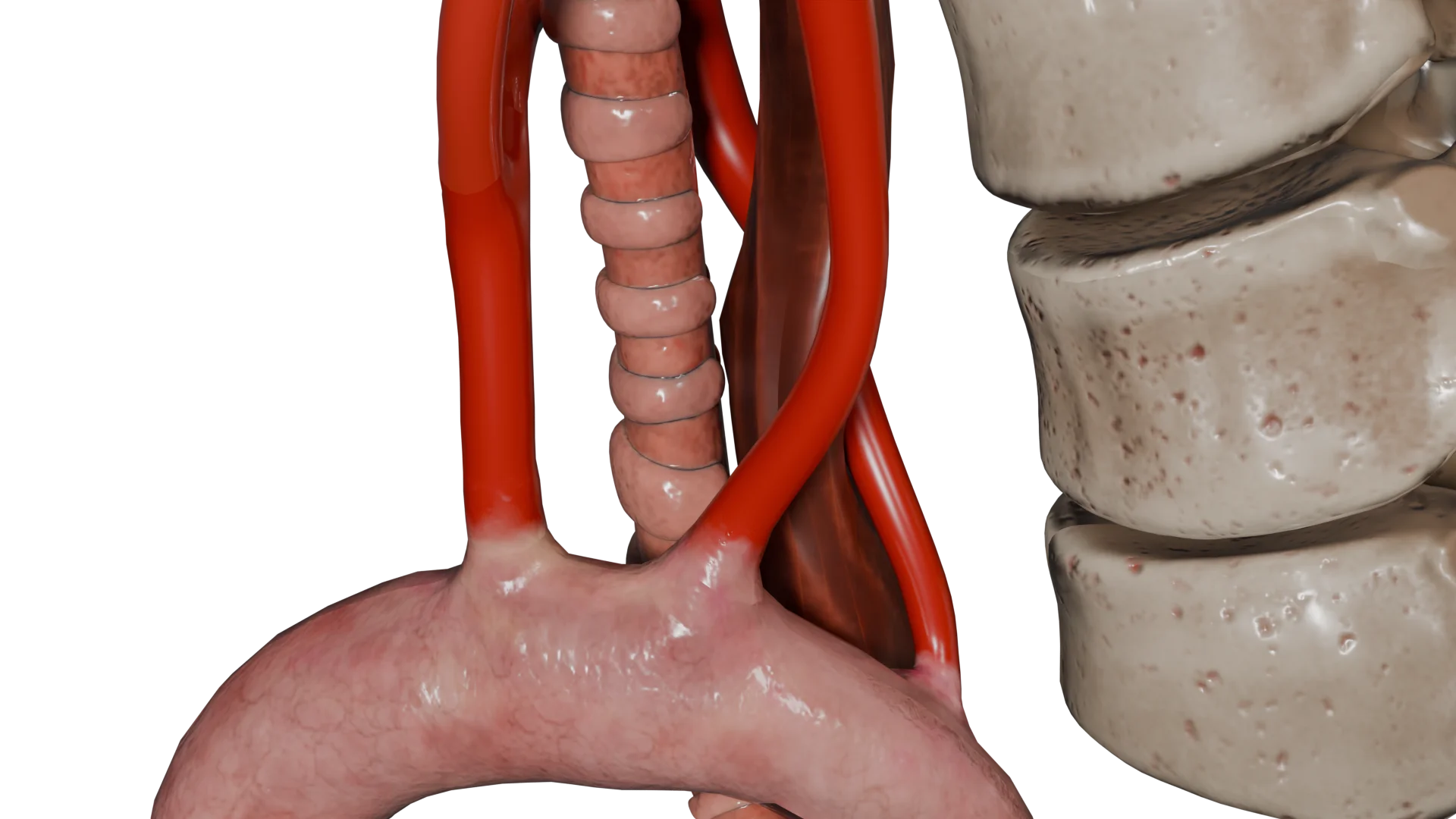
An aberrant right subclavian artery can cause compression of nearby structures.
The artery causes compression of the esophagus → dysphagia.
In severe tracheal compression → respiratory symptoms (cough, dyspnea, stridor).
In rare cases, arterial ring formation (especially in the presence of a persistent right aortic arch and ductus arteriosus).
Aneurysmal dilation of the aberrant vessel (Kommerel’s diverticulum) → risk of rupture or thrombosis.
Passing behind the esophagus, the aberrant right subclavian artery causes its compression
Classification
Along the course of the artery relative to the trachea and esophagus: Retroesophageal
Behind the esophagus (85% of cases)
Tracheoesophageal
Between the trachea and esophagus (10-15% of cases)
Pretracheal
In front of the trachea (less than 5% of cases)
Presence of an aneurysm at the mouth of the artery (Commerel’s diverticulum): Without diverticulum
Often asymptomatic
With a Kommerel’s diverticulum
The mouth of the ARPA is aneurysmatically dilated. Increased risk of rupture, thrombosis, dysphagia
By type of aortic arch: Left-sided aortic arch
Normal arc position, ARPA is the last to depart (the most frequent type)
Right-sided aortic arch
ARPA withdraws as the first vessel → increased risk of vascular ringing
Bilateral aortic arch
Both arcs are preserved, forming an arterial ring
By presence of vascular ring: Without ring
More often asymptomatic
Partial ring
When an arterial duct is present but without a complete loop (symptoms may be present)
Full arterial ring
Combination with persistent ductus arteriosus and right arch. Tracheal and esophageal compression, indication for surgery
In this case: retroesophageal type, without diverticulum, with left-sided aortic arch, without arterial ring
Clinical Manifestations
Most adult patients are asymptomatic with ARPA. Symptomatology is more common in children, especially with combined anomalies.
Major manifestations:
Dysphagia (strained swallowing, more often of solid food) is the main symptom in adults;
Dyspnea, coughing, wheezing – with tracheal compression;
Recurrent respiratory tract infections – in children;
Chest pain, hoarseness, Gorner’s syndrome – in case of compression of neighboring neurovascular structures;
Symptoms may increase with aneurysmal dilatation of the vessel.
Diagnosis
The diagnostic approach depends on the severity of symptoms and the presence of associated anomalies. Modern methods allow visualization of the anomaly with high accuracy.
CT angiography (gold standard). Visualization of the arch anatomy, confirmation of aberrancy, assessment of compression.
MR angiography. An alternative to CT for contraindications to iodine.
Esophagography with barium. Indicated for dysphagia. Characteristic deformation of the posterior wall of the esophagus.
Fibrobronchoscopy. For respiratory symptoms. Diagnosis of tracheal compression.
Echocardiogram. Evaluation of associated cardiac malformations. Visualization of the anomalous artery as well as evaluation of blood flow.
Treatment of an aberrant subclavian artery
Conservative treatment
Eliminating factors that exacerbate dysphagia (e.g., hard or dry food);
Condition monitoring with imaging in asymptomatic course;
In the presence of esophagospasm or esophageal inflammation may be used:
Prokinetics (high level obstruction, e.g., Commerel’s diverticulum with marked compression, must be ruled out before prescribing);
Proton pump inhibitors (if concomitant gastroesophageal reflux or esophagitis is present or suspected).
Surgical treatment
Indications:
Symptomatic dysphagia or respiratory obstruction;
Aneurysm of Commerel’s diverticulum;
Combination with other heart defects requiring correction.
Methods:
Ligation and reimplantation of the artery into the right common carotid artery or brachial trunk (via supraclavicular access or lateral thoracotomy).
Resection of Kommerel’s diverticulum:
Removal of the aneurysmal segment, often combined with reimplantation of the artery;
Preferably via thoracotomy;
In severe calcinosis/thrombosis of Kommerel’s diverticulum in the elderly: stent-graft or hybrid approaches are preferred.
Hybrid procedures: use of stent grafts with prior switch of the aberrant subclavian artery to the carotid artery.
FAQ
1. What is an aberrant right subclavian artery?
An anomaly in which the right subclavian artery branches from the aorta at an atypical location and passes behind the esophagus, sometimes causing esophageal compression.
2. How common is an aberrant right subclavian artery?
Approximately 0.5-2% of the population. It is the most common isolated aortic arch anomaly.
3. What symptoms can occur with an aberrant right subclavian artery?
Dysphagia (difficulty swallowing) is most common. Coughing, wheezing, recurrent respiratory tract infections, especially in children, may also occur.
4. How is the diagnosis confirmed?
CT angiography, the most accurate method of visualizing the course of the artery and its effect on the esophagus/trachea. Barium esophagography and MRI are also used.
5. Is an aberrant artery life-threatening?
In most cases, no. But if there is aneurysmal enlargement (diverticulum of Kommerel), there may be a risk of thrombosis, rupture or embolism.
6. Should this anomaly always be operated on?
No. Surgical treatment is indicated only if symptoms are severe, an aneurysm is present, or there is an arterial ring causing compression.
7. Can symptoms be treated without surgery?
In mild cases, yes. Dietary measures, proton pump inhibitors, prokinetics, treatment of concomitant esophagitis are used.
8. What is a diverticulum of Kommerel?
It is a sac-like enlargement at the site where the aberrant artery branches from the aorta. It may be the source of symptoms or pose a surgical risk.
9. What are the consequences of a right aberrant subclavian artery in the fetus?
The consequences of a right aberrant subclavian artery in the fetus are usually associated with possible esophageal compression, which can lead to swallowing disorders and difficulty in the passage of food. In most cases, the anomaly is asymptomatic and does not seriously affect fetal development. However, if there is severe compression or complications such as aneurysmal dilatation, more serious problems may arise, requiring observation and, in rare cases, intervention after birth.
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
The aberrant subclavian artery: approach to management. Karangelis D, Loggos S, Tzifa A, Mitropoulos FA. Curr Opin Cardiol. 2020 Nov;35(6):636-642. doi: 10.1097/HCO.0000000000000793.
3.
Aberrant subclavian artery in Heritable Aortopathies: One Size Does Not Fit All. Isselbacher EM, Bloom JP. J Am Coll Cardiol. 2023 Mar 14;81(10):992-993. doi: 10.1016/j.jacc.2023.01.020.
4.
Hybrid management of aberrant subclavian artery: A systematic review and meta-analysis. Kordzadeh A, Mouhsen MI, Chan DM, Singh A, Gadhvi VM. Vascular. 2024 Nov 28:17085381241303330. doi: 10.1177/17085381241303330.
5.
A systematic review of open, hybrid, and endovascular repair of aberrant subclavian artery and Kommerell’s diverticulum treatment. Loschi D, Santoro A, Rinaldi E, Bilman V, Chiesa R, Melissano G. J Vasc Surg. 2023 Feb;77(2):642-649.e4. doi: 10.1016/j.jvs.2022.07.010.









.webp)

/aortic%20dissection_main.webp)



