Infectious Diseases of the External Ear Canal: Symptoms, Diagnosis, and Treatment of Otitis Externa
Afanasyeva D.Otorhinolaryngologist, MD
27 min read·April 11, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Infectious diseases of the external auditory canal (otitis externa) are localized inflammation of the skin and underlying tissues (hair follicles, subcutaneous fatty tissue, cartilage with cartilage, in some cases – temporal bone).
Classification of otitis externa
Furuncle of the external auditory canal (infiltration stage, abscessed stage);
Diffuse bacterial otitis externa;
Otomycosis(Aspergillus niger, Candida albicans);
Herpetic infection of the external ear canal;
Malignant necrotizing otitis externa;
Obturating keratosis.
Etiology
The etiologic factor in the development of infections of the external ear is a mixed flora (bacterial, viral, fungal), a prerequisite is also the presence of predisposing factors such as:
Traumatization and maceration of the skin;
Reduction of local acidity;
Reduced sulfur production;
Decrease in the general reactivity of the body;
Presence of extra-organ pathology (metabolic disorders), including immunodeficiency states.
Bacterial causative agents of external otitis media:
Staphylococci (St. aureus, St. aureus, St. epidermidis, St.saprophyticus );
Streptococci (β-hemolytic group A);
Escherichia coli;
Pseudomonas aeruginosa (Pseudomonas aeruginosa);
Protea(Proteus mirabilis);
Klebsiella.
Herpetic infection is caused by:
Herpes simplex virus type 1(Herpes simplex);
Type 3 virus(Varicella zoster).
Mycoses of the ear canals are caused by:
Candida albicans;
Aspergillus niger.
Anatomic Pathology
Herpetic infection
Herpetic infection of the external ear canal is a recurrent skin lesion with herpes viruses type 1 or 3.
Herpetic infection of the external ear canal – 3D model
After human infection , the herpes virus resides in the nerve ganglia in the latent phase(remission period), but when exposed to a number of factors (weakened immunity, stress, UV radiation, progression of chronic diseases, etc.) the virus becomes active and spreads along the course of nerve fibers with characteristic manifestations on the skin(exacerbation phase).
In the exacerbation on the background of erythematous edematousskin appear numerous vesicles that open on 2-3 days and covered with crusts, then the crusts fall off, there is complete healing.
Scratching the vesicles or crusts can cause bacterial infection, which complicates and prolongs the course of the disease.
Peculiarities of damage to the external ear by HPV type 1 (Herpes simplex):
Rashes are chaotic, there is no clear localization;
Occurs at any age;
Facial nerve damage is uncharacterized;
CNS damage is not characterized.
Peculiarities of lesions of the external ear by herpes virus type 3 (Varicella zoster):
A history of chickenpox;
Reactivates in old age or against a background of immunodeficiency;
It occurs as shingles(Herpes zoster oticus);
A clear localization along the course of the nerve is characteristic (the dermatome is affected);
Facial nerve damage in the form of paresis or paralysis is characteristic;
Ramsey-Hunt syndrome may develop when the patellar ganglion of the facial nerve is damaged;
The process may spread to the eardrum;
Complications are possible (CNS damage with the development of meningitis, encephalitis, generalized infection).
Furuncle of the external ear canal
External ear canal furuncle (limited otitis externa) is an inflammation of the hair follicle and surrounding tissues (skin, subcutaneous fatty tissue, sebaceous gland). It should be remembered that the hair follicles in the ear canal are located in the anterior, cartilaginous part. Infection gets in when trying to clean the ear canal with dirty hands or using improvised means, such as paper clips, toothpicks, matches and others.
This infectious process is characterized by stages.
Phase 1 ( infiltration stage):
Localized hyperemia of the skin;
Prominent limited swelling of the ear canal;
Sharp soreness in the affected area;
The deep portions of the ear canal and tympanic membrane are not visible or are partially visible.
Phase 2 ( abscessed stage):
At the center of the inflammation is a purulent necrotic rod;
Tissue fluctuation in the affected area;
The soreness may be decreasing.
During the recovery period, the decay cavity is replaced by scar tissue.
3D animation – furuncle of the external auditory canal in the stage of infiltration and abscessation
External diffuse bacterial otitis media.
External diffuse bacterial otitis media – inflammatory changes in the skin of the external auditory canal. By the nature of the course distinguish acute and chronic otitis externa (more than 6 weeks). The inflammatory process develops at:
Traumatization or maceration of the skin;
Scratching the skin with foreign objects;
Decreased acidity of the skin of the ear canal;
Atrophies of the ceruminous glands;
Carbohydrate metabolism disorder;
Prolonged exposure to moisture — often referred to as “swimmer’s ear”.
Separately, it should be emphasized the occurrence of otitis externa on the background of middle ear pathology, in which through the perforation of the tympanic membrane purulent discharge constantly enters the skin of the external ear canal and contributes to the development of the process.
On the background of bright hyperemic skin, pronounced edema of subcutaneous fatty tissue develops, mainly in the membranous-cartilaginous part of the ear canal, there is abundant impregnation of purulent discharge and desquamated epidermis. The edema may be so pronounced that the walls of the ear canal stick together, the lumen is obturated, the deep parts and the tympanic membrane are not visualized. In some cases, the changes extend to the tympanic membrane, and it becomes thickened, macerated, covered with sloughing epidermis and purulent discharge.
External diffuse bacterial otitis media – 3D model
Chronic course is characterized by less pronounced manifestations. In the presence of extra-organ pathology and a decrease in the overall immune status, the disease can turn into malignant otitis externa.
Otomycosis
Otomycosis is an inflammation of the skin of the external ear canal caused by fungi of the genus Candida albicans, Aspergillus niger. These pathogens are opportunistic and, when a number of factors combine, contribute to the development of the disease. Fungal infection is required for entry and spread:
Traumatization of the skin (when using cotton swabs and other handy tools to clean the ear canal);
Prerequisites for the development of the disease are increased moisture in the lumen of the ear canal;
Metabolic disorders (diabetes mellitus);
Uncontrolled topical application of preparations with antibacterial or hormonal component (resulting in dysbiosis of the skin of the external auditory canal).
In the lumen of the auditory canal against the background of insignificant edema and hyperemia of the skin there are deposits of characteristic color and consistency.
3D animation – otomycosis caused by Candida albicans
In the case of lesions Candida albicans(Candida albicans), the surface is covered with abundant white curds.
The pathogen Aspergillus niger is characterized by the formation of a thin friable film of black color, when magnified, the fungal mycelium can be seen. At the site of removal of pathologic contents, the skin is irritated, macerated.
Malignant necrotizing otitis ex terna (osteomyelitis of the skull base) – inflammation of the external auditory canal, in which the process spreads to the skin and deep underlying tissues (bone, cartilage, cranial nerves, parotid salivary gland). It is a complication of acute otitis ex terna in persons with impaired immune status, uncorrectable diabetes mellitus, oncologic diseases, and the elderly. The causative agent is more commonly Pseudomonas aeruginosa or MRSA (Methicillin-resistant Staphylococcus aureus).
Microorganisms spread through the natural openings (Santorini’s clefts) in the cartilage of the external ear canal along the base of the skull to the jugular opening. This leads to mastoiditis, osteomyelitis of the temporal bone, and inflammation of the cranial nerves. Inflammation is characterized by necrosis of bone and cartilage tissue, erosions, ulcers with the formation of granulation tissue in the lumen of the external auditory canal, the tympanic membrane remains intact.
3D animation – malignant necrotizing external otitis media
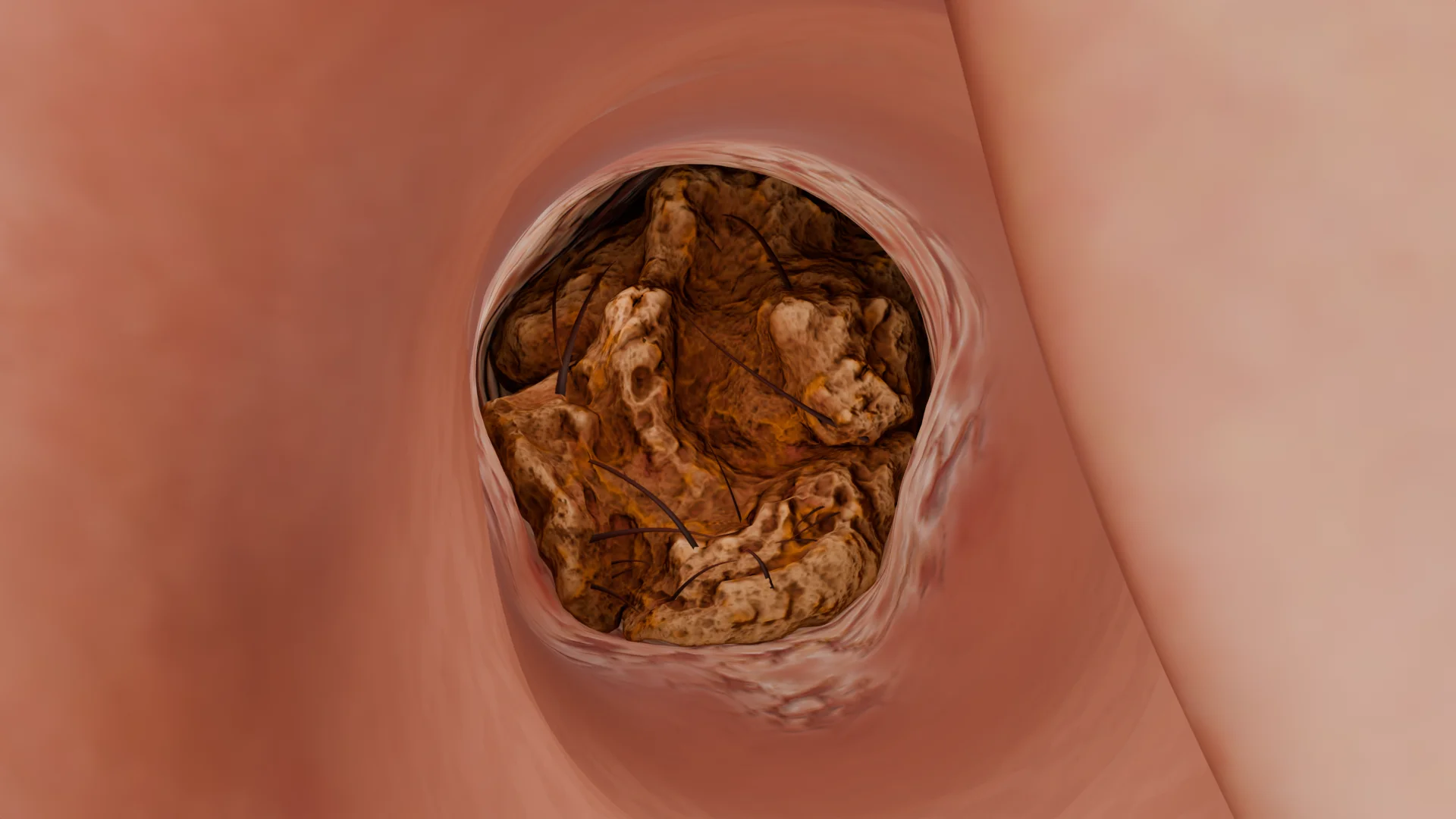
Obturating keratosis
Obturating keratosis – inflammatory changes in the skin of the external auditory canal due to excessive production of epidermal gray masses and obstruction of its lumen. Against the background of obstruction, edema and secondary bacterial infection of the skin in the affected area occur. After removal of pathological contents, thickened keratinized skin is visualized.
3D animation – obturator keratosis (otoscopic view)
Clinical Manifestations
Herpetic infection has different manifestations depending on the type of virus:
Characterization
HPV type 1 Herpes simplex
Herpes virus type 3 Herpes zoster oticus
Epidemiology
All people are susceptible to the disease
People who have had chickenpox are prone to the disease; Elderly people; Immunocompromised people
Local changes
On the background of hyperemic skin: vesicles chaotically (2-3 days) → erosions (3-4 days) → crusts → healing (5-7 days)
On the background of hyperemic skin: vesicles along the nerve (2-3 days) → erosions (5-6 days) → crusts (7 days) → healing, depigmentation zones
Local symptoms
Itching at the site of rashes; Pain is uncharacteristic
Severe itching, throbbing pain, burning at the site of future rashes
General symptomatology
Uncharacteristic; Rarely: headache, subfebrile a few days before rashes
Fever to febrile; Chills; Headache; Anxiety; Insomnia
Complications
Uncharacteristic
CNS involvement; Generalization of infection; Facial nerve paresis/paralysis
Cure
Prone to frequent relapses
Recurrence is possible; Postherpetic neuralgia (pain along the affected nerve after recovery) is characteristic
Features
–
The process is always one-way
Ramsey-Hunt syndrome – the appearance of characteristic clinical symptoms in the lesion of the patellar ganglion of the facial nerve. In this syndrome, in addition to specific herpetic rashes of the outer ear, against the background of severe earache develops paresis or paralysis of the facial nerve. Often may be accompanied by dizziness, disorder of taste sensitivity on the anterior ⅔ of the tongue (due to lesions of the tympanic string). Increased sensitivity to sounds on the side of the lesion – hyperacusis (paresis of the stirrup muscle innervated by the nerve of the same name – a branch of the facial nerve). Facial n erve paresis is peripheral – numbness of facial mimic muscles on the affected side, smoothing of the nasolabial fold, drooping of the corner of the eye and lip, widening of the eye slit, lacrimation.
Furunculus of the external auditory can al is characterized by severe ear pain, which is of constant aching nature, intensifies at night, as well as when palpating the ear drum, chewing, pressing on the goiter. The pain spreads to the temporal region, temporomandibular joint, teeth, neck area, in some cases affecting half of the head.
Symptoms of general intoxication appear: fever to febrile values, chills, increased fatigue, weakness. Regional lymphadenitis develops.
There is a conductive hearing loss , patients complain of congestion and noise in the affected ear, autophony. In some cases, when the furuncle is located in the posterior-upper parts against the background of pronounced edema and hyperemia of the behind-the-ear region, displacement of the cartilage of the auricle, there is a picture similar to mastoiditis, which requires careful differential diagnosis. When the process passes to the abscessing stage, purulent melting of tissues and formation of decay cavity occurs, the pain becomes pulsating, its intensity decreases. In some cases, on 5-7 days the furuncle self-discloses, patients note relief, purulent or purulent-hemorrhagic discharge from the ear canal appears, pain decreases and hearing is restored.
In external diffuse bacterial otitis media, patients complain of hearing loss and noise in the affected ear. There is abundant purulent discharge with an unpleasant odor. Pain occurs when chewing, pressing on the goiter and trying to pull the ear drum. Pain may also irradiate to the upper jaw. Otoscopy is often difficult. The pathologic process develops rapidly, within a few hours. Symptoms of general intoxication rarely appear, the temperature may rise to subfebrile values in the first few days, regional lymph nodes may increase.
3D animation – external diffuse bacterial otitis media
Otomycosis is a recurrent, chronic disease characterized by severe itching and pathological discharge from the external auditory canal. In some cases, in attempts to self-clean the ear canal and to alleviate the condition, scratching the skin with cotton swabs, patients form a plug in the lumen of the canal, which contributes to conductive hearing loss . Pain and manifestations of general intoxication are extremely rare and may appear at the beginning of the acute phase of the disease.
Malignant necrotizing otitis externa is clinically manifested by severe earache, which increases at night, headache on the affected side. It is characterized by abundant purulent discharge with an unpleasant odor, with the progression of the process – exposure of bone tissue.
Malignant external otitis media on the right side – 3D model
Hearing loss at the beginning of the process is conductive due to the obstruction of the ear canal by pathologic contents, but as the process progresses, a neurosensory component may be added due to damage to the preauriculo-cochlear nerve.
If the facial nerve is affected, its paresis or paralysis of the peripheral type appears (facial asymmetry, drooping of the corner of the eye, lip, smoothing of the nasolabial fold, lacrimation). Regional lymphadenitis develops, nearby lymph nodes increase in size, become dense and painful, the skin over them may become inflamed. Symptoms of general intoxication are not characteristic.
This infection is a potentially fatal disease due to the frequent development of complications such as sepsis, dura sinus thrombosis, brain abscess, and meningoencephalitis.
Obturating keratosis is characterized by constant ear pain , which increases with traction of the auricle and pressure on the cochlea, conductive hearing loss and noise in the ear on the affected side.
In order to make a diagnosis, it is necessary to perform:
History taking;
General Examination;
Otorhinolaryngologic examination, otoscopy;
Study of general and biochemical blood analysis;
Bacteriologic seeding of the discharge (to determine the causative agent and sensitivity to drugs);
If viral etiology is suspected – PCR, ELISA or serologic blood tests;
CT of the skull bones, MRI of the brain (in case of complications).
Patients with malignant external otitis media are recommended to perform:
CT scan of the temporal bones;
MRI of the brain;
Ultrasound of the parotid salivary glands;
Consultation with a neurologist to evaluate cranial nerve function;
Microbiologic studies of the excreta with determination of sensitivity;
Biopsy of the affected tissue;
Clinical and laboratory monitoring;
Maintaining a glucose profile;
Determination of HIV status;
If necessary – lumbar puncture;
If available, scintigraphy with technetium-99 or gallium-67.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Treatment of otitis externa
Antiviral drugs such as acyclovir, valacyclovir and famciclovir (the drug of choice) are used to treat herpetic infection. Symptomatically prescribe antihistamines,NSAIDs, infusion therapy, in severe cases – glucocorticosteroid drugs. To control pain syndrome, including postherpetic neuralgia , metamizole, gabapentin, pregabalin, tricyclic antidepressants are used, in severe cases opioid analgesics (tramadol, morphine) are prescribed.
In the treatment of otitis externa and furunculosis , the prescription of local preparations prevails. Combined preparations in the form of solutions with antibacterial, hormonal and analgesic components have a good effect. In case of pronounced swelling inside the ear canal insert a tampon and moisten it with the drug 3-5 times a day, thanks to which the drug penetrates deeper, then the tampon falls out and then the drug can be freely instilled into the ear canal. In case of severe pain syndrome, analgesics are administered internally. It is recommended to perform a regular toilet of the external ear canal by rinsing with antiseptic solutions or dry method.
Furuncle in the abscessed stage is subject to surgical treatment. Under local anesthesia at the site of the largest swelling, its opening and revision, with the help of antiseptic solutions remove caseous masses, followed by the installation of drainage and aseptic dressing, then perform daily dressings. Antibacterial drugs are administered internallyif there is no effect from local treatment, or in severe course.
For the treatment of pathology of the external auditory can al, it is recommended to use preparations in the form of solutions, because the placement of ointments contributes to the formation of plugs of ointment, wax, hair and sloughing epithelium, poor ventilation, which further leads to longer treatment and recurrence of infection. After treatment of acute symptoms to prevent reinfection is recommended to reduce the pH-environment of the external ear canal with solutions of acetic or boric acid to prevent reinfection. It should be remembered that otitis externa develop in the presence of predisposing factors, which must be excluded for a favorable result of treatment. To prevent otitis media of “swimmers” after bathing, it is recommended to remove moisture from the ear canal with a hair dryer or alcohol drops that dry the skin well.
In the treatment of fungal otitis ex terna, special attention is paid to the mechanical removal of pathological contents from the lumen of the external auditory canal, perform a dry toilet, and then topically apply antifungal drugs. For successful treatment of this infection, combined preparations that include antibacterial and hormonal drugs should be avoided. The lumen of the ear canal should not be covered with absorbent cotton or turundas to prevent the development of a greenhouse effect and recurrence of the process.
Treatment of malignant otitis externa is necessarily carried out in hospital conditions, in some cases in the intensive care unit or intensive care units. Until the results of microbiological studies, empirical antibiotic therapy with fluoroquinolones and penicillins is prescribed, then correction according to the results of studies. Local treatment of the lesion focus with antiseptic solutions, regular dressings with ointments with antibacterial and steroid component, if necessary, surgical excision of necrotized areas within healthy tissues is performed. An obligatory condition is the correction of glycemia level.
In the treatment of obturating keratosis it is necessary to remove pathological masses from the lumen of the ear canal, usually by mechanical means, beforehand it is necessary to anesthetize the patient adequately to achieve the best effect, in some cases anesthesia is used. After clearing the passage, local treatment with combined solutions containing an antibacterial and hormonal component is carried out . To prevent recurrences, this group of patients needs regular visits to the ENT doctor for timely cleaning of the ear canal, as well as periodic injection of 3% hydrogen peroxide into the lumen of the ear canal.
FAQ
1. What are the symptoms of otitis externa?
Otitis externa (outer ear infection) presents with the following symptoms: • Ear pain, which worsens when pressing on the tragus or pulling the auricle; • Itching and discomfort in the ear canal; Swelling and redness of the ear canal skin, sometimes with pus-like discharge; Hearing loss; • Ringing in the ear or a feeling of ear fullness.
2. How to identify otitis externa in a child?
Parents may suspect otitis externa in a child based on the following signs: • Complaints of ear pain (the child cries or touches the ear); • Crying when pressing on the tragus or pulling the ear — a characteristic diagnostic sign; • Discomfort during feeding (chewing increases the pain); • Ear discharge (yellowish or clear); • Fever (not always present, more common in purulent cases); • Hearing loss (the child asks to repeat things or doesn’t respond to quiet sounds).
3. What is “swimmer’s ear” and what is it caused by?
“Swimmer’s ear” is a type of otitis externa caused by prolonged contact of the ear with water. It is common in people who frequently swim in pools, the sea, or other bodies of water.
Why is it called that?
The name reflects the main cause of the condition — constant exposure to water, which leads to: 1. The removal of the protective earwax layer that normally creates an acidic environment to inhibit the growth of bacteria and fungi; 2. Maceration of the skin (softening due to moisture) → formation of microcracks → entry of infection (such as Pseudomonas aeruginosa, staphylococci, or fungi).
4. What is the difference between fungal otitis externa and bacterial otitis media?
• Fungal: itching, white curd-like or black discharge; • Bacterial: pus, intense pain.
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Total Otolaryngology—Head and Neck Surgery, Anthony P. Sclafani, Robin A. Dyleski, Michael J. Pitman, Stimson P. Schantz. Thieme Medical Publishers, Inc., 2015. ISBN 978-1-60406-646-3.
3.
Бербом Х. Болезни уха, горла и носа / Ханс Бербом, Оливер Кашке, Тадеус Навка, Эндрю Свифт; пер. с англ. – 2-е изд. – М. : МЕДпреcс-информ, 2016. – 776 с. : ил. ISBN 978-5-00030- 322-1.
4.
Medina-Blasini Y, Sharman T. Otitis Externa. 2023 Jul 31. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. PMID: 32310515.
5.
Jackson EA, Geer K. Acute Otitis Externa: Rapid Evidence Review. Am Fam Physician. 2023 Feb;107(2):145-151. PMID: 36791445.
6.
Bojanović M, Stalević M, Arsić-Arsenijević V, Ignjatović A, Ranđelović M, Golubović M, Živković-Marinkov E, Koraćević G, Stamenković B, Otašević S. Etiology, Predisposing Factors, Clinical Features and Diagnostic Procedure of Otomycosis: A Literature Review. J Fungi (Basel). 2023 Jun 13;9(6):662. doi: 10.3390/jof9060662. PMID: 37367598; PMCID: PMC10302809.
7.
Al Aaraj MS, Kelley C. Necrotizing (Malignant) Otitis Externa. 2023 Oct 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. PMID: 32310598.



.webp)
%20otitis%20externa_2.webp)