




Acute Sinusitis (Acute Rhinosinusitis): Classification, Clinical Manifestations, Diagnosis, and Treatment
A detailed review of rhinosinusitis, including classification, symptoms, diagnostic approaches, and current treatment strategies.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Injury to the middle and inner ear – Anatomo-functional damage to the middle and/or inner ear caused by pathologic force and resulting in hearing loss or vestibular disorders.
Traumatic perforation of the tympanic membrane is a violation of the integrity of the tympanic membrane caused by an external stimulus and accompanied by hearing loss.
Auditory ossicle chain damage is a pathologic condition in which the integrity of the auditory ossicle chain is compromised, resulting in impaired sound transmission to the structures of the inner ear.
Hemotympanum – accumulation of blood in the tympanic cavity when the tympanic membrane is intact.
Fracture of the pyramid of the temporal bone is a violation of the anatomical integrity of the temporal bone, caused by mechanical impact, in which the structures located inside the pyramid are damaged.
Posttraumatic mastoiditis – inflammatory changes in the mucosa and bone of the mastoid mediated by trauma.
All injuries to the middle and inner ear are caused by an external pathological stimulus. The most common causes are motor vehicle accidents or self-inflicted injuries due to the use of improper objects to clean the ear canal (ingestion of foreign bodies). In addition,
Hemotympanum may occur during violent coughing or sneezing due to rupture of small blood vessels in the tympanic mucosa. This condition can also occur after posterior nasopharyngeal tamponade for massive bleeding or adenotomy. In addition, hemotympanum may be a manifestation of a fracture of the temporal bone pyramid.
Temporal bone fractures are a special case of skull base fracture. In addition to road traffic accidents, the leading cause is fights, beatings. Longitudinal fractures are caused by the application of force to the temporal region on the affected side, while transverse fractures occur when mechanical impact is applied to the frontal or occipital region.
It should be noted that all the mentioned types of injuries can be combined with each other.
In case of insufficient diagnosis, untimely diagnosis or lack of adequate treatment against the background of the above conditions, post-traumatic mastoiditis may develop. This occurs when pathogenic microflora joins from the nasopharynx or through a perforated tympanic membrane.
Perforation of the tympanic membrane is characterized by the disruption of the integrity of all its layers: epithelial, fibrous and mucous layers. A hole is formed at the site of the lesion, along the edges of which hemorrhagic drips are determined, and blood is found in the external auditory canal. When the temporal bone is damaged, liquor may also flow. The localization and size of the perforation are important for the appropriate management of these patients.
Centralperforations are perforations that are located in the tense part of the tympanic membrane.The central perforations are those that are located in the taut part of the tympanic membrane, most often in the antero-inferior quadrant, and do not involve the cartilaginous fibrous ring.
The marginal perforations are located in the unstretched portion perforations are located in the non-tensioned part of the tympanic membrane (posterior-upper quadrant) and extend to the fibrous ring. Perforations of these localizations can be either rounded or slit-shaped. A total perforation is a defect that covers almost the entire area of the PD. This leaves small flaps around the periphery, usually they are wrapped inside the middle ear cavity. Even with minor damage to the tympanic membrane, dislocation of the auditory ossicles is possible. Traumatic perforation in the posterior-upper quadrant is most often combined with a rupture of the auditory ossicle chain.
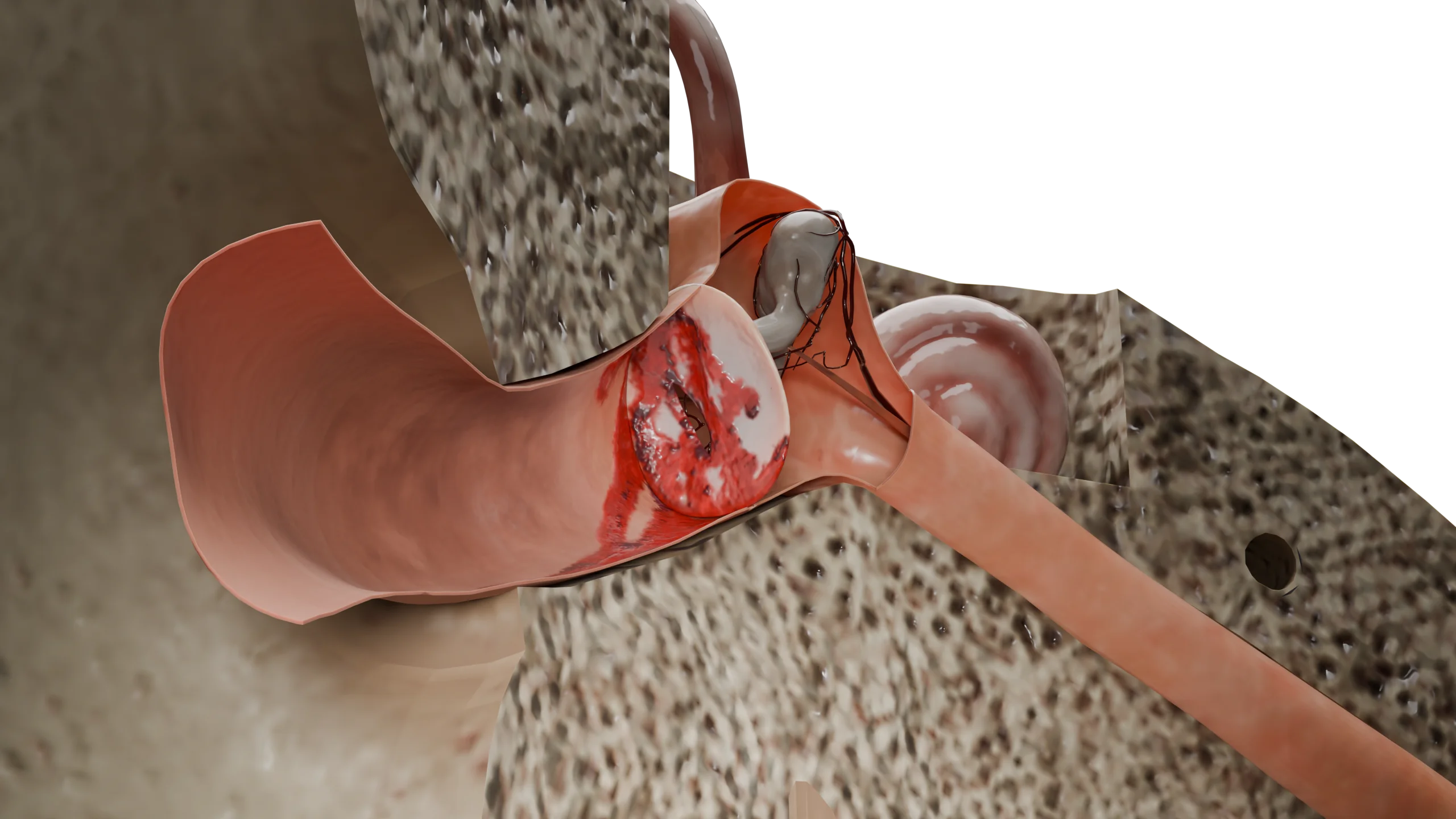
Fractures of the auditory ossicle articulation are much more common than fractures of the auditory ossicles and can occur either in combination with traumatic perforation of the tympanic membrane or independently. The most common lesion of the auditory ossicle chain following blunt or penetrating trauma to the middle ear is a rupture of the anvil-hammer junction. The anvil-hammer joint is better protected by the supratympanal recess, but its dislocation is the second most common injury to the auditory ossicles. The anvil is the heaviest of the three ossicles of the middle ear and is supported by two weak ligaments, and is therefore more likely to be dislocated and fractured. Fixation of the malleus is provided by its attachment to the tympanic membrane, to the muscle that tenses the tympanic membrane, as well as the presence of three ligaments: anterior, posterior and superior. All of these protect the malleus as much as possible from damage and dislocation. The ramus is also tightly fixed by the annular ligament to the foramen ovale, but traumatic dislocation of the ramus from the foramen ovale is quite common.
Fractures of the auditory ossicles are rare and can be localized anywhere. The most common are fracture of the long anvil leg and fracture of the stapes. Fracture of the malleus handle has also been described in isolated cases. Fracture of the ossicles results in displacement of the preserved chain to the ligamentous attachment sites.
In hemotympanum, the tympanic membrane remains intact, but hemorrhagic contents accumulate in the tympanic cavity. As a consequence, the tympanic membrane becomes purplish-blue in color and may bulge into the lumen of the ear canal. There may be several sources of hemorrhage: traumatized vessels of the tympanic cavity mucosa or blood entering the middle ear through the auditory tube from the nasal cavity or nasopharynx after surgical interventions or nosebleeds.
Fractures of the temporal bone pyramid are classified according to the axis of injury and are subdivided into:
In practice, combinations of the two are also found.
The most common type of fracture (about 80% of cases) is the longitudinal type, in which the structures of the inner ear remain intact, but the chain of the auditory ossicles is damaged. There is also a rupture of the tympanic membrane and a fracture of the bony wall of the ear canal. In addition, the canal of the facial nerve may be traumatized with the subsequent development of edema. It is not uncommon to see fluid or blood oozing from the external auditory canal (otoliquorrhea or otogematorrhea, respectively).
Transverse fractures damage the cochlea or semicircular canals, resulting in a perilymphatic fistula. The internal auditory canal and the facial nerve canal are also affected. The tympanic membrane remains intact, but there may be hemotympanum.
Posttraumatic mastoiditis is an inflammation that occurs against the background of traumatic changes in the middle ear and, as a rule, in the presence of pathologic contents (blood) in the cells of the mastoid process. This inflammatory process spreads to the mucous membrane and bone tissue of the tympanic cavity and temporal bone. As it progresses, bone caries is observed with the formation of sequestrations surrounded by purulent contents. In the presence of perforation in the tympanic membrane is determined by the oozing of pus into the external ear canal. The tympanic membrane may remain intact, but its bulging is observed, and the identifying signs are smoothed. The posterior wall of the ear canal may also be overhanging.
The leading symptoms in all middle and inner ear injuries are hearing loss, noise and congestion in the ear, and pain at the time of injury and afterwards. Conductive hearingloss is characterized by damage to the tympanic membrane and middle ear. If the inner ear is damaged, there is sensorineural or mixed hearing loss.
If the tympanic membrane is damaged, a small amount of blood may ooze from the ear canal. If the middle ear is damaged, the amount of hemorrhagic discharge increases, hearing may be reduced to the point of deafness in the damaged ear. The
Longitudinal fractures are characterized by slight conductive hearing loss, bleeding or liquor from the ear canal through the damaged tympanic membrane, delayed temporary paresis of the facial nerve, and brief dizziness.
In transverse fractures, the clinic is more vivid: it is characterized by sensorineural hearing loss up to deafness, pronounced labyrinthine disorders (prolonged and intense vertigo, nausea, vomiting), spontaneous nystagmus in the direction of the healthy ear, facial nerve paralysis occurring immediately after the injury and liquor flow into the nasopharynx through the Eustachian tube. In both cases, Battle’s symptom of behind-the-ear hematomas may be identified. Fractures of the temporal bone have early and late complications. The most formidable of these are carotid and facial nerve injuries, mastoiditis and meningitis.
In traumatic mastoiditis, inflammatory symptoms appear against the background of general manifestations of trauma: body temperature rises to febrile values, behind-the-ear pain has a constant throbbing character and increases with palpation of the mastoid process. In the presence of perforation, there is also pus flowing from the ear canal.
Diagnosis is based on otorhinolaryngologic examination and carefully collected anamnesis. Otomicroscopy is an important diagnostic step.
Vestibular functions must be evaluated, audiometry, tympanometry, valvular and vestibular tests are performed. Hearing tests with whispered and spoken speech are performed. Among the instrumental methods, CT-diagnosis of temporal bones with thin slices to determine the volume of the lesion is mandatory. In some cases, consultation with a neurologist, neurosurgeon and ophthalmologist is recommended. Electroneuromyography is used to assess the function of the facial nerve.
Find more scientifically accurate content on our social media








In the treatment of tympanic membrane perforations, a wait-and-see approach is most justified, as even large perforations can close on their own. If it is assumed that the perforation was infected at the time of injury, local antibacterial preparations in the form of drops are prescribed. Prevention of secondary infection is important for the best possible healing, which includes limiting the ingress of water into the external ear canal and ensuring good functioning of the auditory tube. If the perforation does not heal within 2-3 months, and if the perforation is located in the unstretched portion of the tympanic membrane or involves the fibrous ring, a myringoplasty is performed. In case of BP infection, antibacterial drugs are prescribed, systemically or locally. After myringoplasty it is recommended to follow up with an ENT doctor for at least 2 years, as there is still a risk of cholesteatoma formation.
In hemotympanum , antibacterial therapy is administered orally and topical preparations in the nasal cavity (nasal decongestants) for better functioning of the eustachian tube. Self-purging of the auditory tube is recommended. If the outcome is favorable, the blood is lysed within 7-10 days. If the contents of the tympanic cavity are infected, its puncture is performed, aspirate the pathological secretion and conduct a bacteriological study. According to the results of sensitivity, antibacterial therapy is prescribed.
To restore the ossicular chain, tympanic cavity revision and tympanoplasty are performed 3-6 months after the injury. This is due to the fact that during this time there may be an independent improvement of hearing due to scar fusion of the ruptures.
Conservative therapy for temporal bone fractures includes the use of systemic corticosteroids to prevent delayed facial nerve paresis and the administration of systemic antibiotic therapy to prevent bacterial complications. A wait-and-see approach to surgical treatment is warranted. Early surgical intervention is necessary in case of facial nerve paralysis, the presence of perilymphatic fistula with increasing vestibular symptoms or pronounced sensorineural hearing loss. If facial nerve edema develops in the delayed period against the background of conservative therapy, decompression of the facial nerve canal is performed. In case of continued liquorrhea for more than 14 days, surgical treatment with closure of the defect is also indicated. In the presence of inflammatory complications
1. How do I know if the inner ear is damaged?
For an accurate diagnosis, a doctor’s consultation and instrumental tests (CT scan, audiometry) are necessary.
2. What should be the first aid for middle and inner ear injuries?
3. When is surgical intervention required for ear injuries?
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Total Otolaryngology—Head and Neck Surgery, Anthony P. Sclafani, Robin A. Dyleski, Michael J. Pitman, Stimson P. Schantz. Thieme Medical Publishers, Inc., 2015. ISBN 978-1-60406-646-3.
3.
Бербом Х. Болезни уха, горла и носа / Ханс Бербом, Оливер Кашке, Тадеус Навка, Эндрю Свифт; пер. с англ. – 2-е изд. – М. : МЕДпреcс-информ, 2016. – 776 с. : ил. ISBN 978-5-00030- 322-1.
4.
Sagiv D, Migirov L, Glikson E, Mansour J, Yousovich R, Wolf M, Shapira Y. Traumatic Perforation of the Tympanic Membrane: A Review of 80 Cases. J Emerg Med. 2018 Feb;54(2):186-190. doi: 10.1016/j.jemermed.2017.09.018. Epub 2017 Oct 28. PMID: 29110975.
5.
Dolhi N, Weimer AD. Tympanic Membrane Perforation. [Updated 2023 Aug 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK557887/
6.
Campbell E, Tan NC. Ossicular-Chain Dislocation. [Updated 2023 Jul 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK560621/
7.
Patel A, Lofgren DH, Varacallo MA. Temporal Fracture. [Updated 2024 Jan 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK535391/
Loading test 6 questions
Table of Contents




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io




