The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Thrombophlebitis is an inflammation of a venous wall accompanied by a blood clot. Superficial veins of the lower limbs are most commonly affected.
Patients aged 60 to 70 are more susceptible to the disease.
Moreover, thrombophlebitis is more prevalent among females, particularly in those with varicose veins.
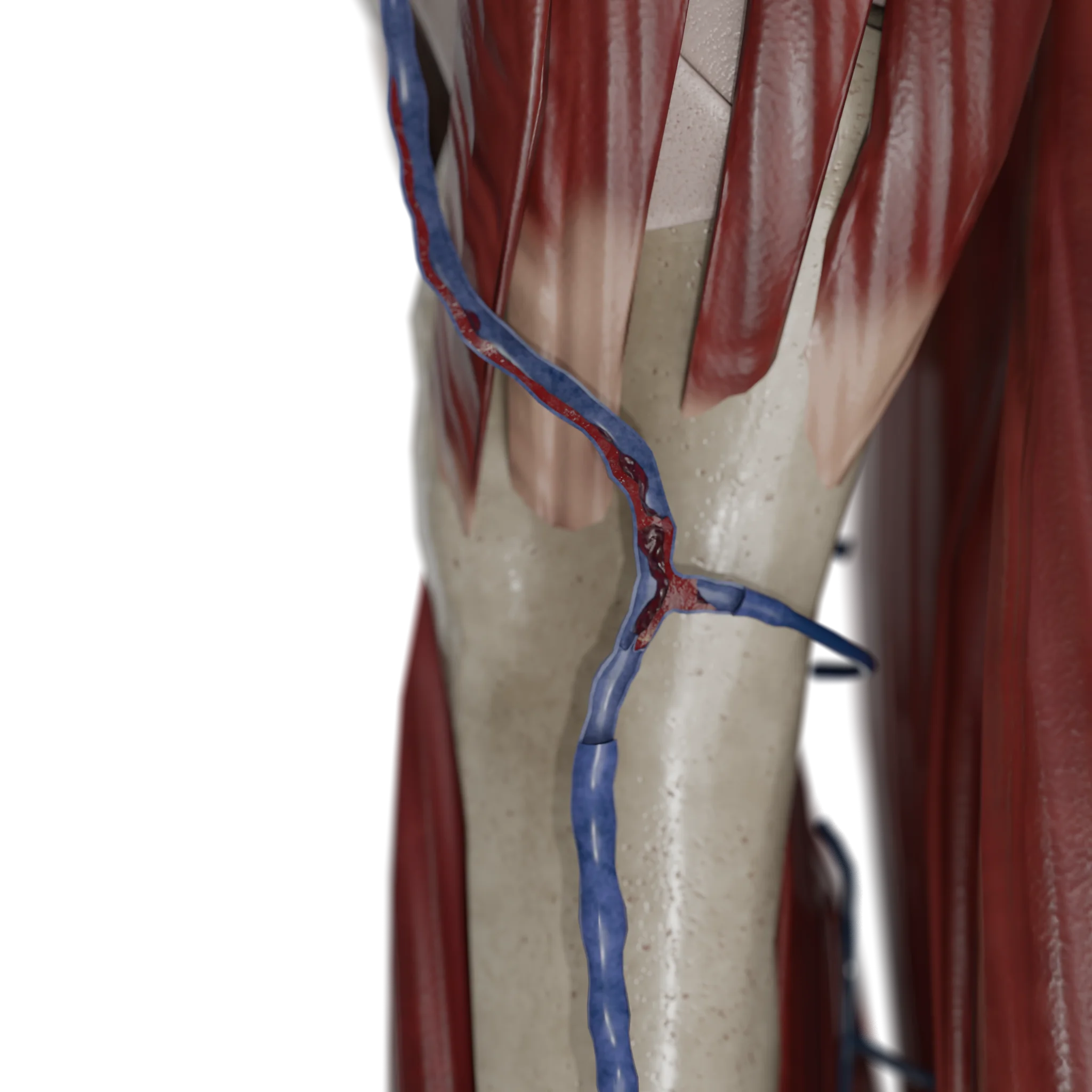
Thrombophlebitis of Great Saphenous Vein – 3D Model
Etiology
Thrombophlebitis develops as a result of multiple factors collectively referred to as Virchow’s triad.
Damage to the venous wall — a key trigger of the inflammatory and prothrombotic process — may occur under the following circumstances:
Catheterization and injections (especially in arm veins): a common cause of iatrogenic thrombophlebitis;
Surgical procedures (such as open leg surgeries, venectomy, or bypass surgery);
Soft tissue trauma, including contusions, burns, and venipunctures;
Skin and soft tissue infections, resulting in septic thrombophlebitis, frequently associated with cellulitis, abscesses, or erysipelas.
Venous Stasis and Impaired Outflow
Varicose veins of the lower limbs — the most common concomitant disease associated with superficial thrombophlebitis;
Immobilization — including bed rest, prolonged air travel, and plaster casts;
Cardiac failure — especially in decompensated cases;
Obesity — a contributing factor to reduced venous return and blood congestion in the lower limbs;
Pregnancy and the postpartum period — due to pelvic vein compression and hormonal changes.
Hypercoagulability (increased blood clotting)
Malignancies
Thrombophilias, including antithrombin III deficiency, protein C and S deficiencies, factor V Leiden, and antiphospholipid syndrome;
Hormonal therapy — estrogen use (oral contraceptives, hormone replacement therapy);
Systemic inflammatory and autoimmune diseases — including systemic lupus erythematosus and inflammatory vasculitis;
COVID-19 — a known cause of transient hypercoagulability and thrombosis, including in the superficial veins.
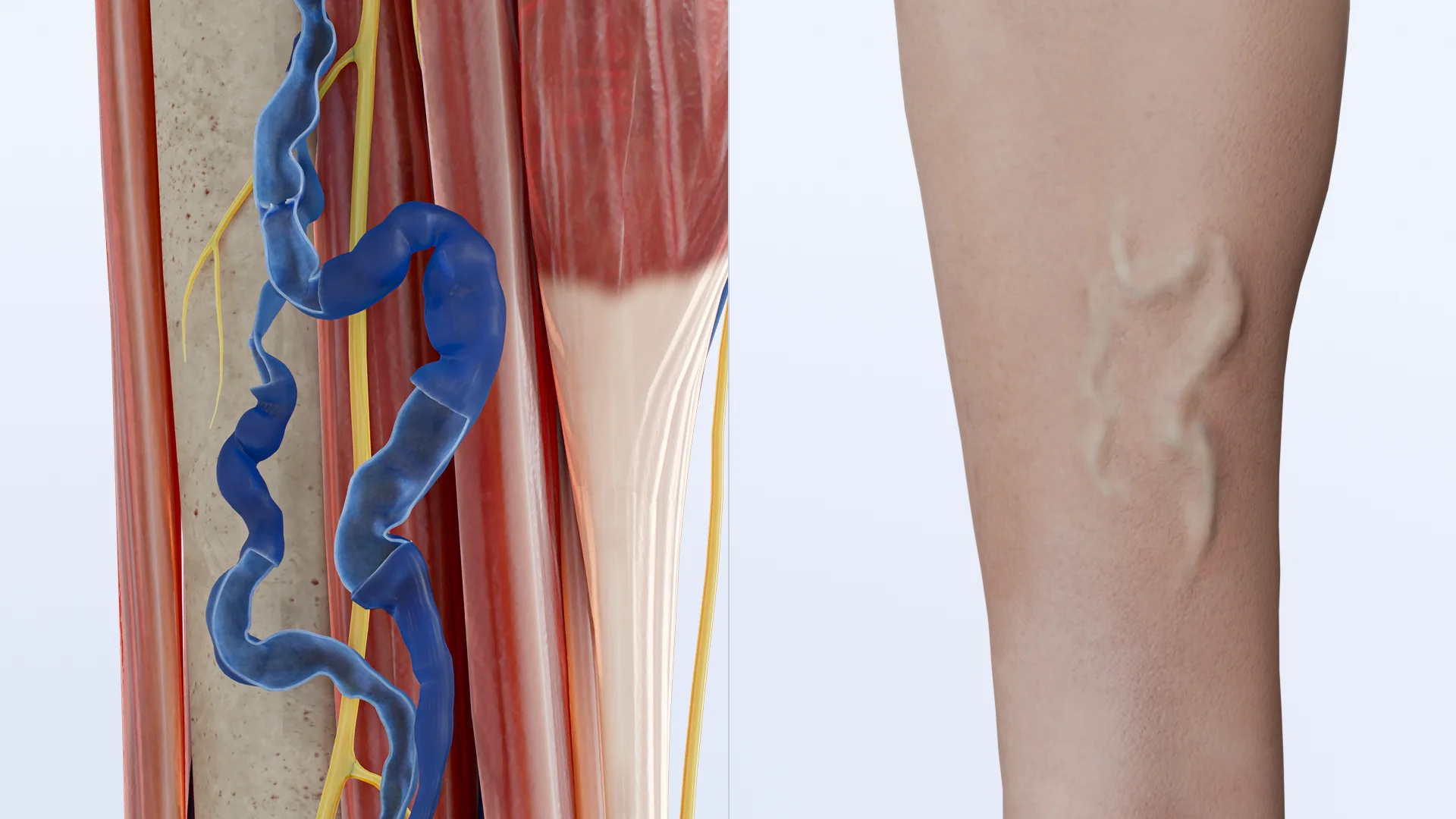
Varicose Veins of Lower Limbs — Most Common Concomitant Disease in Superficial Thrombophlebitis – 3D Model
Pathogenesis
Damage to Endothelial Lining of Venous Wall
Injured endothelium loses its antithrombotic properties, expresses adhesion molecules (ICAM-1, VCAM-1), activates platelets and leukocytes, and triggers the production of proinflammatory cytokines (IL-1β, TNF-α).
Coagulation Cascade Activation
Following intimal injury and tissue factor activation, the extrinsic pathway of blood coagulation is initiated:
Coagulation factors VIIa and X are activated;
Prothrombin is converted to thrombin;
Fibrin is produced, stabilizing the clot;
Simultaneously, platelets aggregate to form a “white” platelet matrix — particularly in areas of turbulent blood flow.
A local decrease in blood flow velocity promotes and sustains site-specific thrombogenesis. This process is facilitated by several mechanisms:
Enhanced contact interaction between formed elements of blood and the vascular wall;
Elevated concentration of procoagulants in the affected area;
Reduced washout of thrombogenic molecules.
Inflammatory infiltration of venous wall (sterile inflammation):
Migration of neutrophils and monocytes;
Secretion of matrix metalloproteinases, which promote intimal destruction;
Production of IL-6, IL-8, and other proinflammatory mediators;
Fibrosis and thickening of the venous wall in chronic stages;
In cases of secondary infection, the process may become purulent, resulting in septic thrombophlebitis.
Thrombus Organization or Embolization
Further progression may follow one of two scenarios:
Organization — the thrombus becomes infiltrated by fibroblasts, covered by endothelium, and transforms into a fibrous, scar-like strand. This leads to obliteration of the venous lumen, and the process becomes chronic.
Embolization — if the thrombus is unstable and extends into the deep venous system, it may fragment and migrate, resulting in thromboembolism.
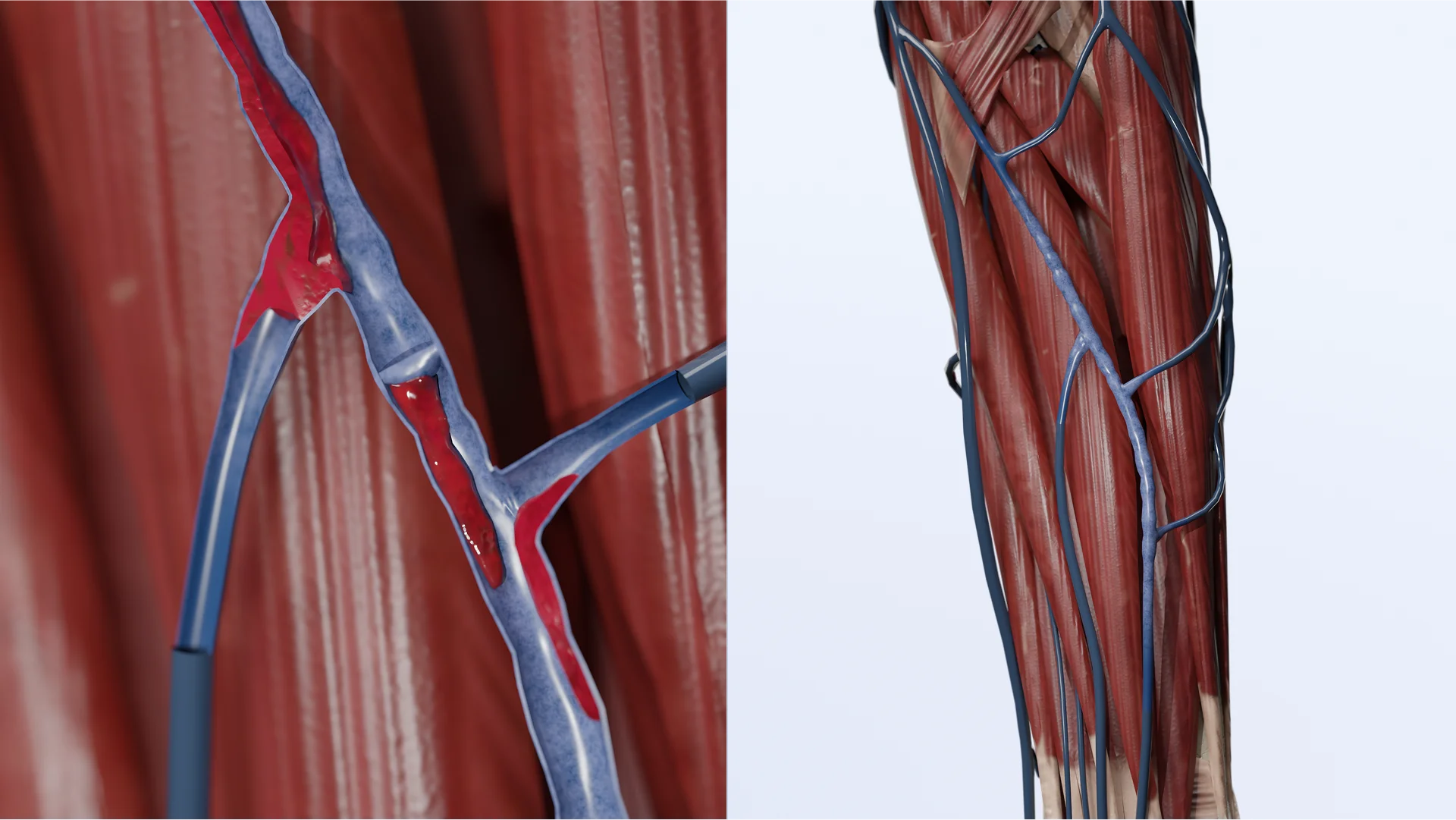
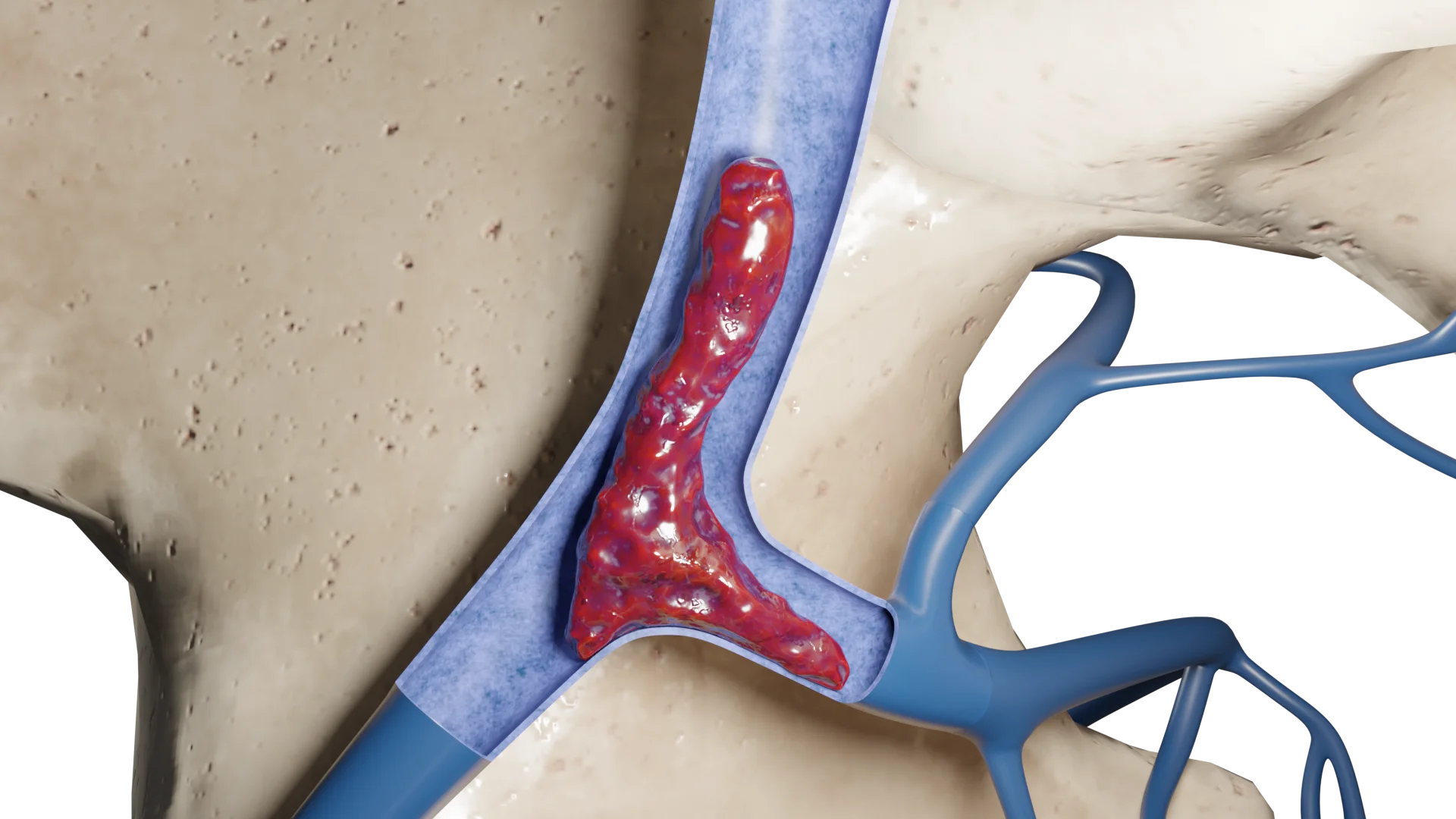
Inflammatory Infiltration of Median Antebrachial Vein Wall and Blood Clot within Its Lumen – 3D Model
NOTE: Although thrombophlebitis is often confined to subcutaneous veins and considered “clinically insignificant”, when a vein adjacent to the saphenofemoral or saphenopopliteal junction is involved, the disease may progress into the deep venous system. Therefore, even a “superficial” inflammation should be regarded as a potential risk for thromboembolism.
Thrombophlebitis Classification
Location:
Superficial thrombophlebitis: Involvement of the subcutaneous veins, most commonly the great saphenous vein of the lower limb.
Deep thrombophlebitis: Involvement of the deep veins, associated with an increased risk of thromboembolism.
Clinical course:
Acute: Sudden onset with pronounced symptoms.
Chronic: Prolonged course with intermittent exacerbations.
Presence of infection:
Aseptic: No associated infection.
Septic: Accompanied by infection.
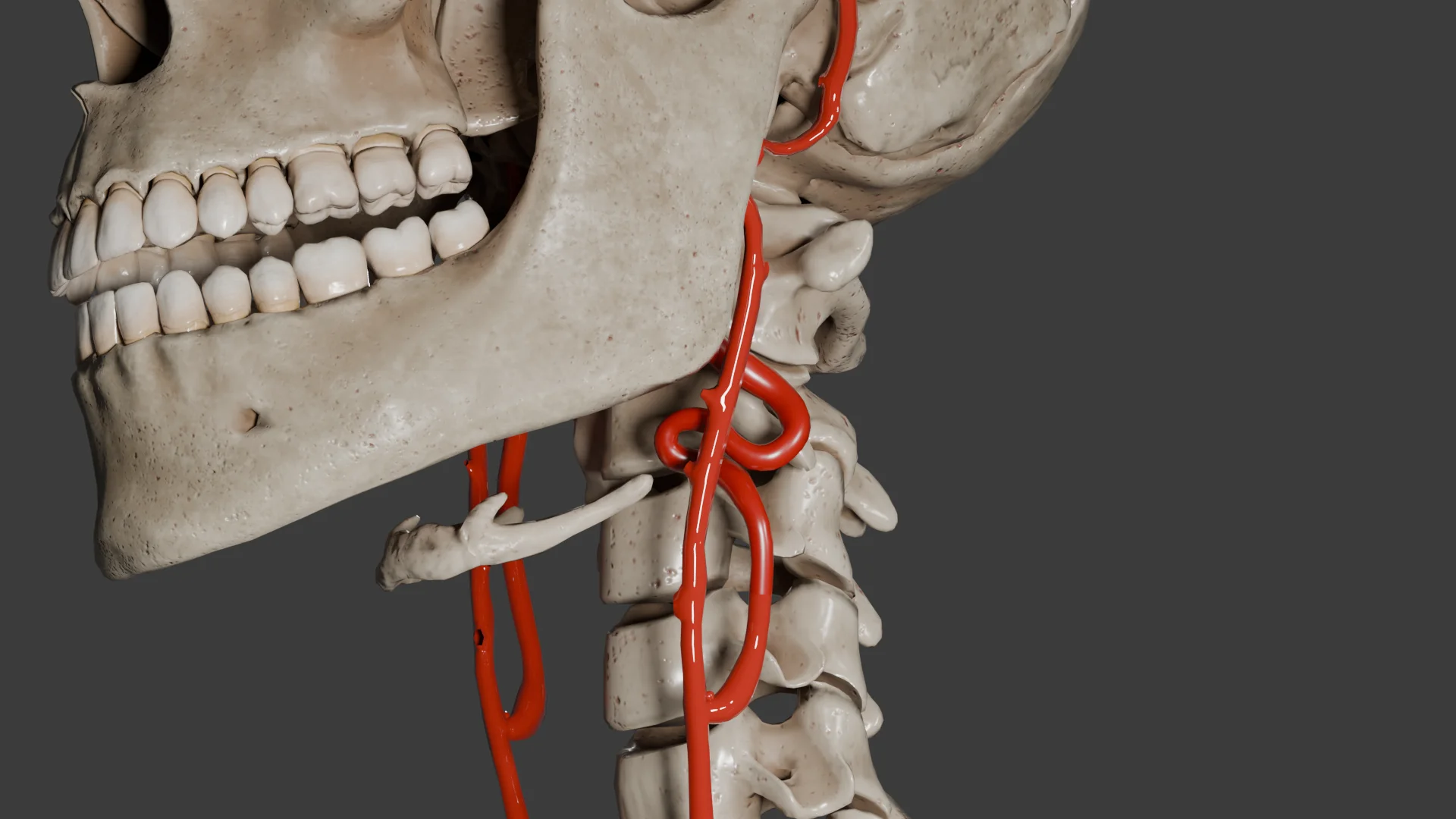
Thrombophlebitis of Great Saphenous Vein – 3D ModelThrombophlebitis of Median Antebrachial Vein – 3D Model
Clinical Manifestations
Clinical manifestations of thrombophlebitis depend on the anatomical location, extent of inflammation, depth of the affected veins, and associated complications. Acute superficial thrombophlebitis of the saphenous veins in the lower limbs has the most typical presentation, although symptoms may vary.
1. Common Symptoms of Acute Thrombophlebitis
Pain along the affected vein — dull or burning in nature, intensified upon palpation or movement.
Induration along the vein — palpable as a firm, tender, immobile strand.
Skin redness — over the site of inflammation, often linear and following the course of the vein.
Localized elevation in skin temperature.
Tissue swelling — mild and localized.
Limited limb mobility — typically observed when a large segment of the vein is involved.
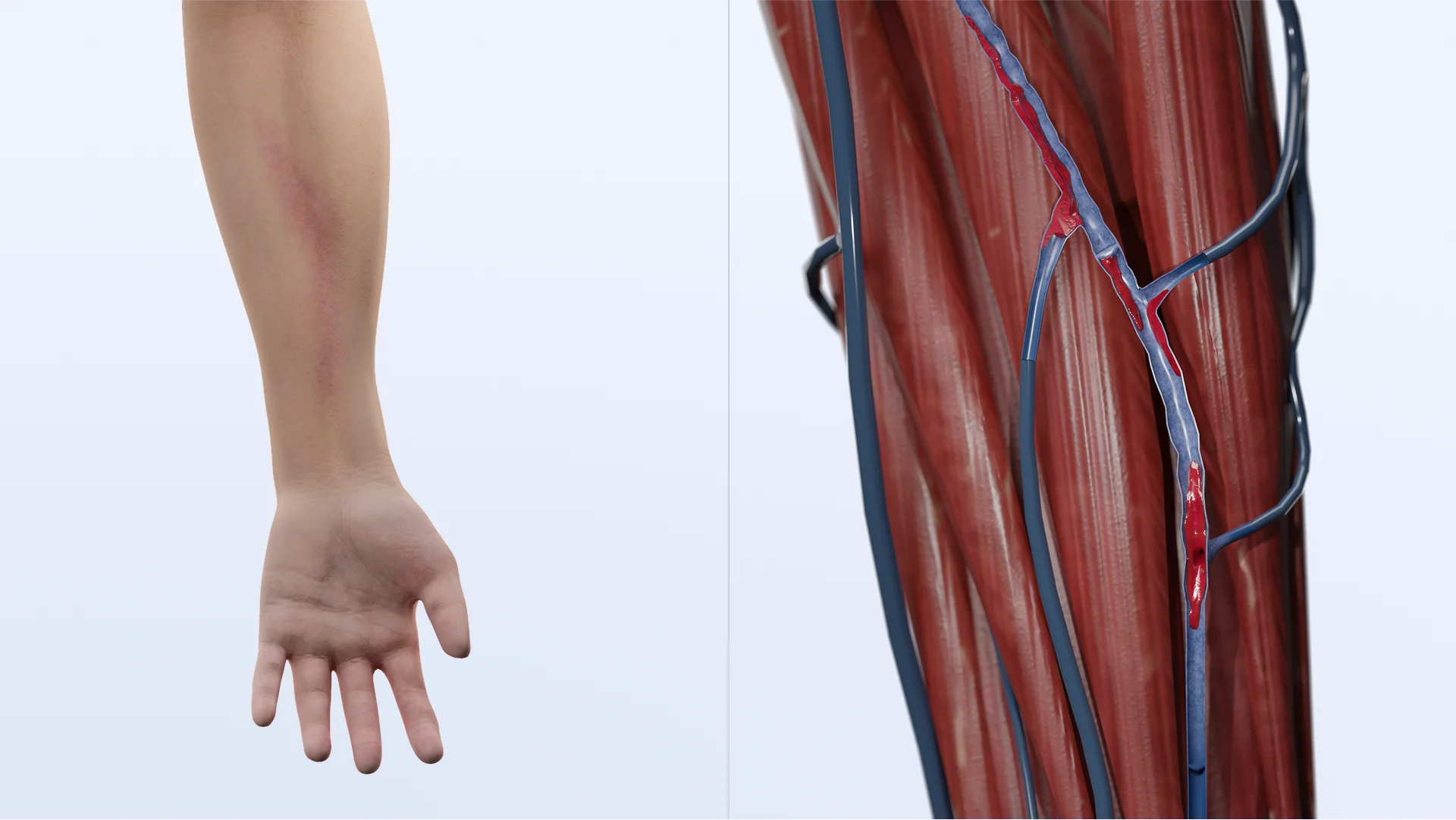
Local Manifestations of Thrombophlebitis (Saphenous Veins of Forearm and Legs) – 3D Model
2. Clinical Features of Deep Thrombophlebitis
When inflammation affects the deep veins, more pronounced symptoms may occur:
Diffuse swelling of the entire limb, often asymmetrical;
Cyanosis or mottled skin;
Intense pain in the calf or thigh during walking or upon compression (Homan’s sign);
Sensation of tension and heaviness in the affected limb.
Unlike the superficial forms of the disease, deep thrombophlebitis often presents without prominent signs of cutaneous inflammation.
3. Location and Symptom Characteristics:
Lower limb veins — the most common site. Typical clinical manifestations are observed.
Upper limb veins — often associated with catheterization; characterized by localized pain and induration, with symptoms typically resolving rapidly following catheter removal.
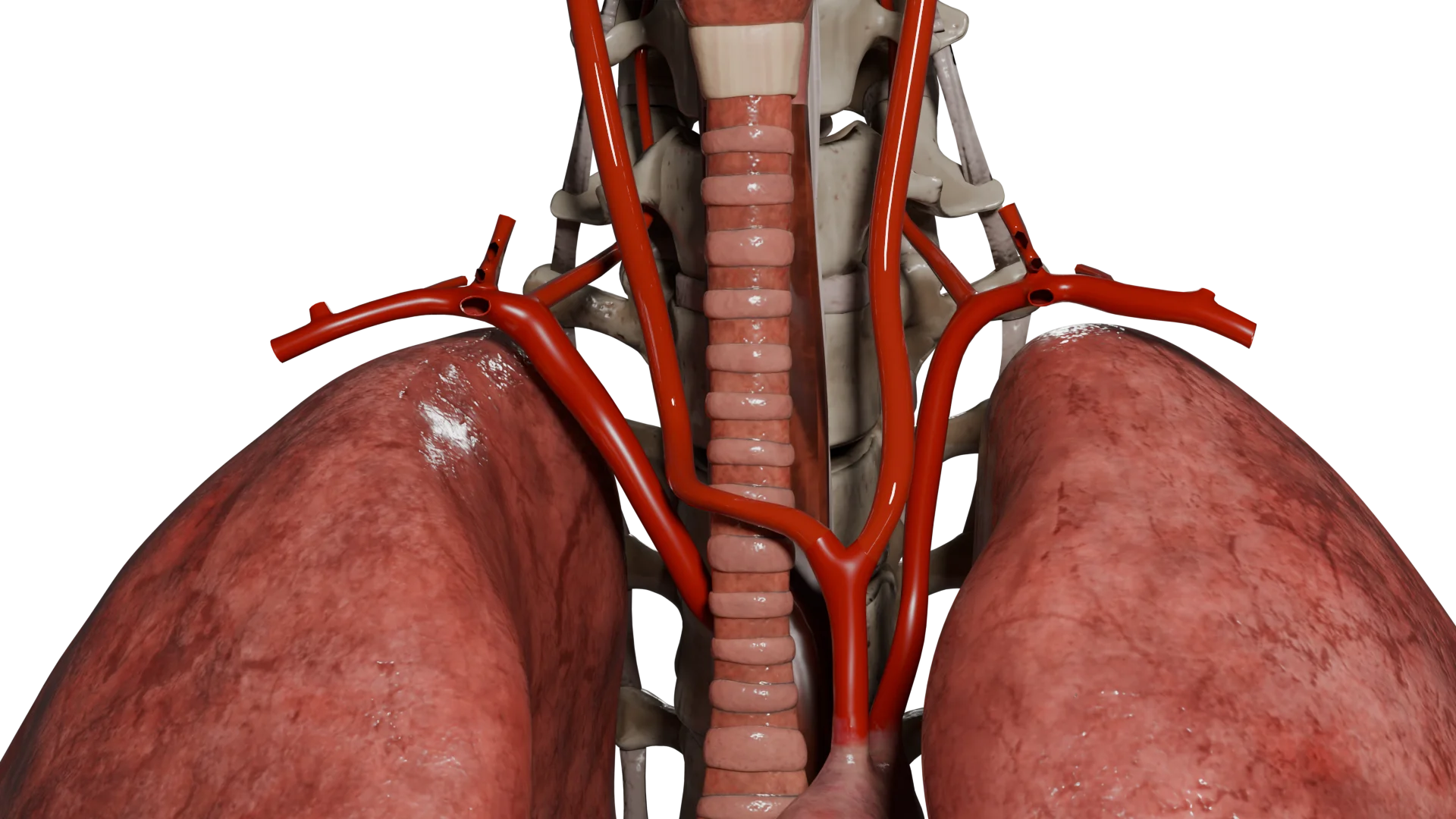
Thoracic and cervical veins (e.g., Paget — Schroetter syndrome or superior vena cava thrombophlebitis) — accompanied by arm swelling, cyanosis, and engorgement of the venous network.
Perianal and genital veins — possibly involved in specific inflammation such as Behçet disease or penile vein thrombophlebitis.
4. Complications
Once a blood clot affects deep veins, patients may experience progressive edema, intensified pain, and poorly localized symptoms.
Pulmonary embolism (PE) is associated with sudden onset of dyspnea, tachycardia, chest pain, and syncope.
Septic thrombophlebitis presents with fever, chills, purulent discharge from the catheter site, and signs of systemic inflammation.
Diagnosis of Thrombophlebitis
Physical examination (see Clinical Manifestations).
Venous duplex ultrasound is the gold standard for diagnosis. It helps assess:
Presence of a blood clot within the vein lumen (echogenic structure);
Loss of venous compressibility (a vein fails to collapse under probe pressure);
Absence or disturbance of venous blood flow on Doppler imaging;
Increased wall thickness and hyperechogenicity of the vein;
Thrombus extension into deep veins or venous junctions (e.g., saphenofemoral, saphenopopliteal).
CT angiography or MR angiography is utilized in complex or atypical cases, including:
Thrombophlebitis involving the pelvis, neck, or thorax;
Suspected thrombosis not confirmed by ultrasound;
Extrinsic compression of veins (e.g., by tumors or lymph nodes).
Laboratory tests
Possible elevation in leukocytes, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP).
D-dimer levels may be moderately increased, particularly when deep veins are involved.
Note: A normal D-dimer level does not rule out thrombophlebitis; however, elevated results warrant further evaluation to exclude deep vein thrombosis (DVT) and pulmonary embolism (PE).
Coagulation panel (activated partial thromboplastin time (aPTT), prothrombin time (PT), international normalized ratio (INR)).
Blood tests (creatinine — prior to initiating low-molecular-weight heparins or fondaparinux; liver function tests — necessary in cases of long-term anticoagulant therapy.
Thrombophilia screening is indicated in cases of:
Recurrent thrombophlebitis of unclear etiology;
Family history of thrombotic complications;
Thrombosis in atypical locations (e.g., neck, upper limbs, brain);
Tests include: Protein C and S; antithrombin III; genetic mutations: Factor V Leiden, prothrombin G20210A; antiphospholipid antibodies (anti-β2 glycoprotein I, anticardiolipin antibodies, lupus anticoagulant).
Treatment of Thrombophlebitis
Risk Factor Modification
Smoking cessation;
Bodyweight management;
Physical activity;
Avoidance of prolonged standing and sitting;
Management of diabetes mellitus, hyperlipidemia, and hypertension;
Compression stockings (class II) — particularly in cases of varicose veins, following an acute phase.
Medical Therapy
Anticoagulant therapy is indicated not only for DVT, but also for superficial vein thrombophlebitis when associated with high-risk features or complicated progression.
Indications:
Thrombus length ≥ 5 cm;
Proximity within 3 cm of the saphenofemoral or saphenopopliteal junction;
Severe pain and inflammation;
Risk factors for DVT/PE (e.g., malignancy, recent surgery, pregnancy, thrombophilia).
Recommended medications:
Fondaparinux, 2.5 mg/day, subcutaneously — for 45 days;
Low-molecular-weight heparins (e.g., enoxaparin);
Rivaroxaban — used off-label; permissible when injections are contraindicated.
Nonsteroidal anti-inflammatory drugs (NSAIDs) are prescribed for all patients with acute inflammation, especially in the presence of pain and swelling.
Ibuprofen, nimesulide, meloxicam, ketoprofen;
Duration: 7–10 days, or until inflammation regresses.
Antibiotic therapy is prescribed only when infectious (septic) thrombophlebitis is suspected.
First-line agents: amoxicillin/clavulanate, cefazolin, ceftriaxone. For MRSA — vancomycin, linezolid.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Surgical treatment
Indications:
Thrombus extension to the saphenous vein junction;
High risk of thromboembolism accompanied by contraindications to anticoagulation therapy;
Septic thrombophlebitis;
Ineffective medical therapy;
Recurrent episodes associated with varicose vein disease.
Methods:
Ligation of the affected vein (typically performed at the junction of the great saphenous vein);
Thrombectomy — rarely indicated; reserved for cases unresponsive to other therapies;
Combined phlebectomy (removal of varicose veins) — carried out following resolution of the acute phase.
FAQ
1. What is thrombophlebitis and how does it differ from thrombosis (phlebothrombosis)?
Thrombophlebitis refers to inflammation of the venous wall when a blood clot forms, most commonly in superficial veins. Thrombosis is a broader term denoting the presence of a blood clot within a vessel, which may or may not involve inflammation.
2. Is superficial thrombophlebitis dangerous?
Although generally less dangerous than deep vein thrombosis, superficial thrombophlebitis can occasionally lead to complications — particularly if the thrombus extends into the deep venous system, potentially resulting in pulmonary embolism.
3. Should thrombophlebitis be treated if it causes minimal discomfort?
Yes, it should. Even with mild symptoms, both inflammation and a blood clot require clinical observation and often medical therapy — especially if the blood clot is located near deep veins.
4. How is thrombophlebitis treated?
Treatment typically involves anticoagulants, nonsteroidal anti-inflammatory drugs (NSAIDs), and compression therapy. Surgery may also be indicated, though less frequently.
5. What signs indicate that thrombophlebitis develops complications?
Thromboembolism may be suspected when swelling worsens, pain radiates to other regions, skin discoloration occurs, and a patient experiences sudden episodes of dyspnea or chest pain. Once you have notices these signs, seek medical attention immediately.
6. Is it safe to apply heat to the lower limb affected by thrombophlebitis?
No, it is not. Heat therapy may promote inflammation and increase the risk of embolism. Compression stockings and anti-inflammatory medications are preferable alternatives.
7. Can varicose veins evolve into thrombophlebitis?
Yes, they can. Varicose veins are a major risk factor for thrombophlebitis. Damaged venous valves and blood stasis typically precede inflammation and blood clots.
8. Which test confirms thrombophlebitis?
Duplex ultrasound is the basic method to diagnose the condition. Laboratory tests such as D-dimer and C-reactive protein (CRP) help assess the degree of inflammation and the risk of complications.
9. When is surgical treatment indicated for thrombophlebitis?
Surgical intervention may be necessary when a blood clot is close to the deep venous system, in cases of purulent inflammation, ineffective medical therapy, or frequent recurrent episodes associated with varicose veins. Surgery is performed at the discretion of a vascular surgeon.
10. How can the risk of recurrent thrombophlebitis be reduced?
To control risk factors, patients should be advised to wear compression stockings, maintain a healthy body weight, stop smoking, manage their varicose veins, engage in regular physical activity, and avoid prolonged immobility.
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Editor’s Choice – European Society for Vascular Surgery (ESVS) 2021 Clinical Practice Guidelines on the Management of Venous Thrombosis. Kakkos SK, Gohel M, Baekgaard N, Bauersachs R, Bellmunt-Montoya S, Black SA, et al. Eur J Vasc Endovasc Surg. 2021 Jan;61(1):9-82. doi: 10.1016/j.ejvs.2020.09.023.
3.
Superficial Thrombophlebitis. Czysz A, Higbee SL. 2023 Jan 2. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing
4.
Treatment for superficial thrombophlebitis of the leg. Di Nisio M, Wichers IM, Middeldorp S. Cochrane Database Syst Rev. 2018 Feb 25;2(2):CD004982. doi: 10.1002/14651858.CD004982.pub6.
5.
Antithrombotic Therapy for VTE Disease: Second Update of the CHEST Guideline and Expert Panel Report. Stevens SM, Woller SC, Kreuziger LB, Bounameaux H, Doerschug K, Geersing GJ, et al. Chest. 2021 Dec;160(6):e545-e608. doi: 10.1016/j.chest.2021.07.055.
6.
Superficial vein thrombosis: State of art. A review. Cortese F, Stolfi L, Luzi G, Tarsia G, D’Addeo G, De Francesco M, et al. Phlebology. 2025 May 3:2683555251338747. doi: 10.1177/02683555251338747.


.webp)

.webp)

/aortic%20dissection_main.webp)
