Pathological Tortuosity of Carotid Arteries: Etiology, Pathogenesis, Classification, Diagnosis, Treatment
Kizyukevich O.Cardiovascular surgeon, MD
12 min read·May 27, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
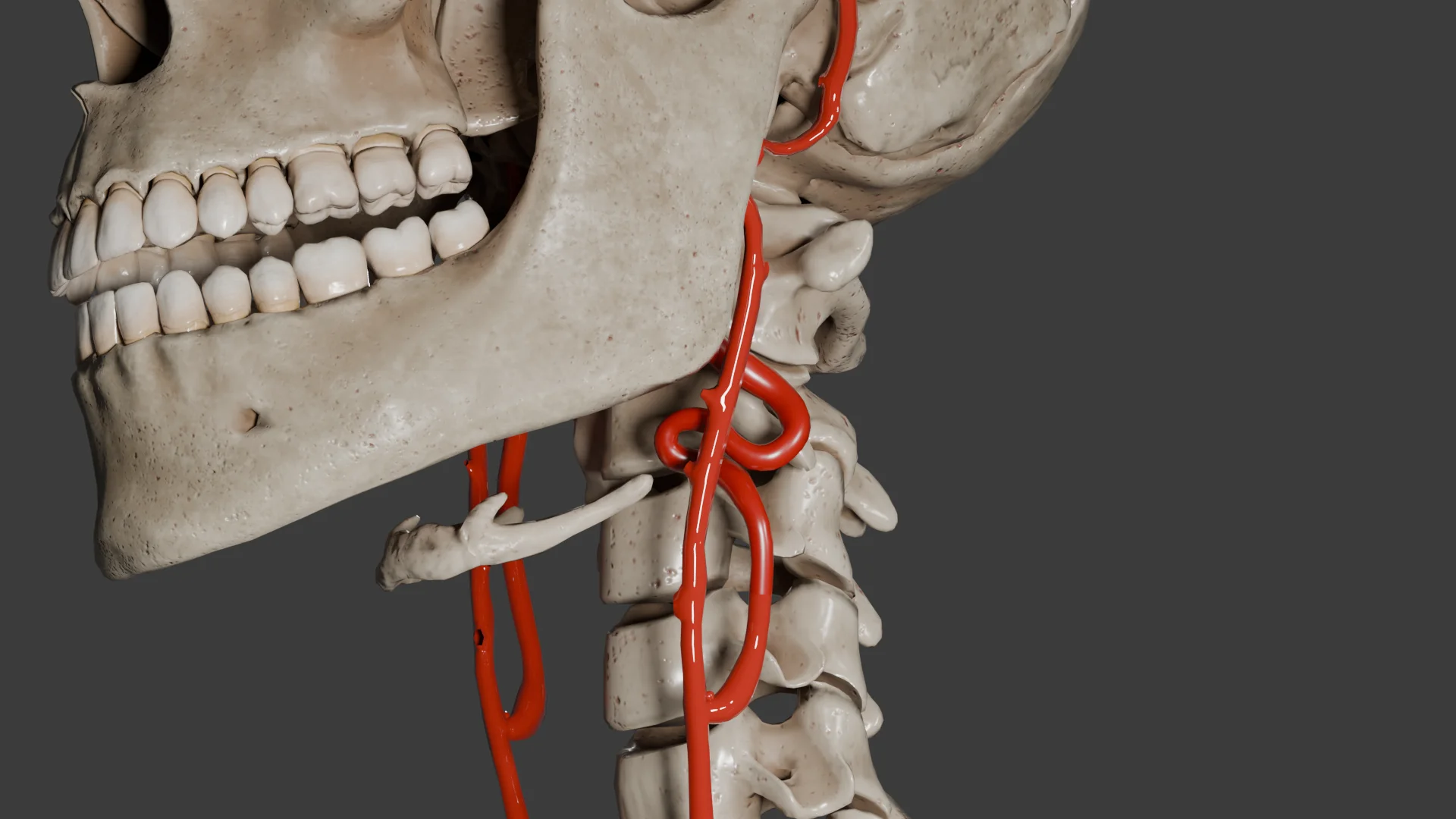
Pathological tortuosity of the carotid arteries refers to a deviation from the normal linear course of the vessel that manifests as bends (kinking), loop-like curls (coiling), or spiral-shaped tortuosity. The condition may affect both the internal carotid artery (ICA) and the common carotid artery (CCA), and is most commonly found in the extracranial portion of the ICA.
Based on ultrasound and angiography data, this deviation occurs in 10–40 % of various populations.
Additionally, the disease is more prevalent among females, particularly older women.
This age-related pattern is attributed to decreased vascular elasticity and elongated arteries.
The alterations are typically unilateral, though bilateral involvement may also occur.
Etiology
Pathological tortuosity of the carotid arteries is characterized by a multifactorial etiology, which may include:
Congenital diseases:
Connective tissue insufficiency within the vascular wall;
Genetic syndromes, such as: Marfan syndrome (mutations in the FBN1 gene encoding fibrillin-1), Ehlers — Danlos syndrome (particularly its vascular form associated with type III collagen defects), Loeys — Dietz syndrome (disruption of the TGF-β signaling pathway);
Congenital arterial elongation in a normally sized neck;
In some instances, pathological tortuosity of the carotid arteries may be identified in multiple family members, suggesting a possible autosomal dominant or polygenic inheritance pattern.
Acquired conditions:
Hypertension increases mechanical stress on the vascular wall, contributing to arterial elongation.
Atherosclerosis induces vascular remodeling.
Age-related changes involve reduced elasticity, fibrosis, and elongation of the arteries.
Obesity, particularly in women, may cause displacement of anatomical structures.
Iatrogenic factors may arise following neck surgeries or vascular prosthetic procedures.
Pathogenesis
Increasing age and/or certain diseases (hypertension, atherosclerosis, diabetes mellitus) may cause the following changes in the arterial wall:
Degeneration of elastic fibers within the media;
Fragmentation and remodeling of collagen structures in the adventitia;
Increased rigidity of the arterial wall;
Decreases vessel anchorage within the surrounding tissues.
As a result, the artery becomes less resistant to bending and deformation; under elevated pressure, it elongates and deviates from its linear course.
It is important to note that some researchers question the association between arterial hypertension or other cardiovascular risk factors and the development of carotid artery tortuosity.
Pathological tortuosity — whether acquired or congenital — leads to altered hemodynamics within the arterial bed:
Elongation of the artery → S- or U-shaped course, looping;
Disruption of laminar blood flow → turbulence, reduced perfusion pressure, and decreased efficiency of oxygen delivery;
In certain head positions, blood flow may deteriorate dynamically;
When combined with an atherosclerotic plaque, the risk of transient cerebral ischemia increases.
Classification
By location: Internal carotid artery (ICA), common carotid artery (CCA).
By etiology: Congenital, acquired.
Morphological Classification:
Tortuosity
A long, mildly sinuous bending of an artery without acute angles. This condition is typically asymptomatic and affects the elderly.
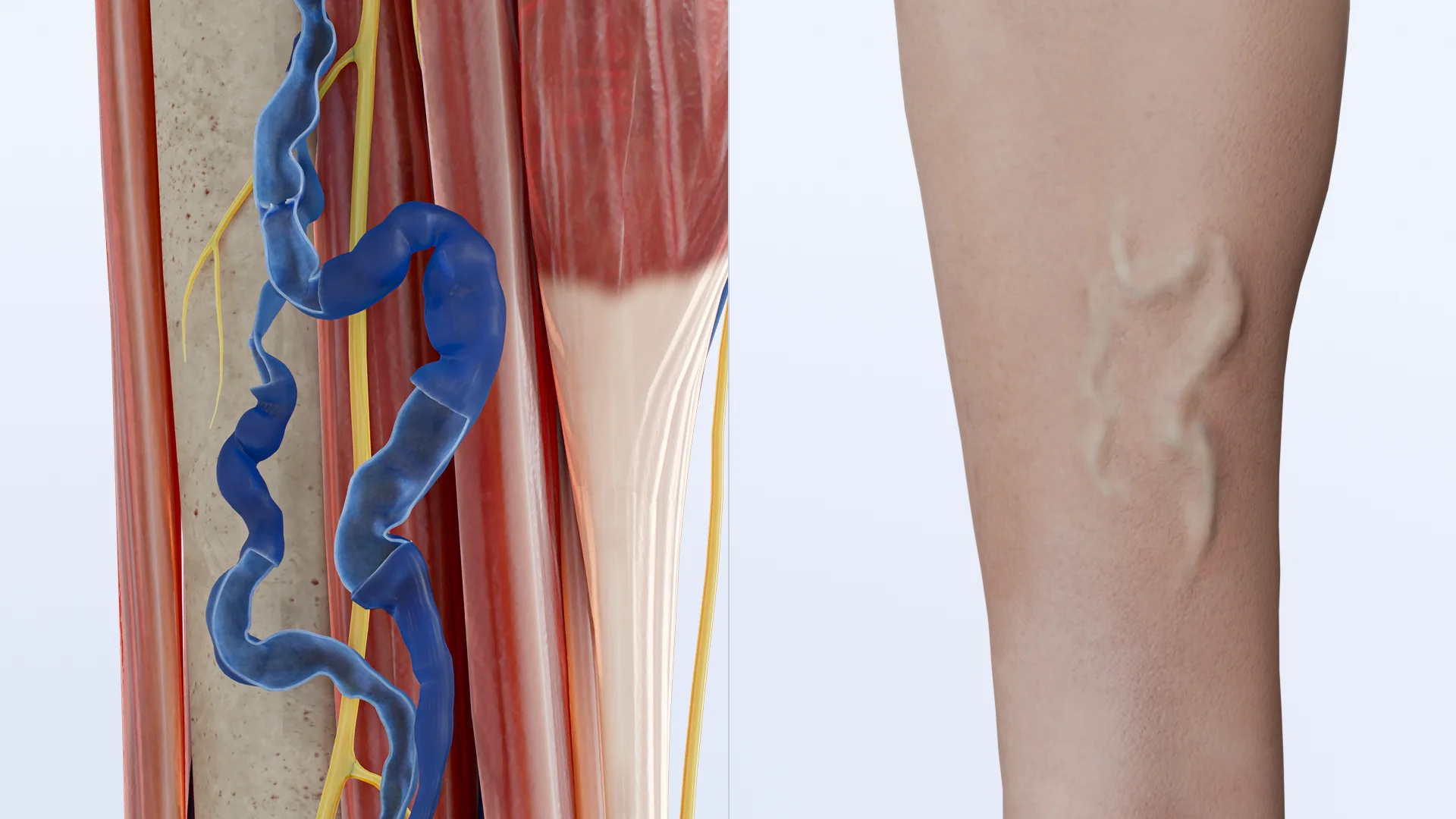
Coiling
A coil that makes the vessel run in the opposite direction; the artery becomes elongated and folds onto itself. This configuration may often result in a moderate reduction in blood flow.
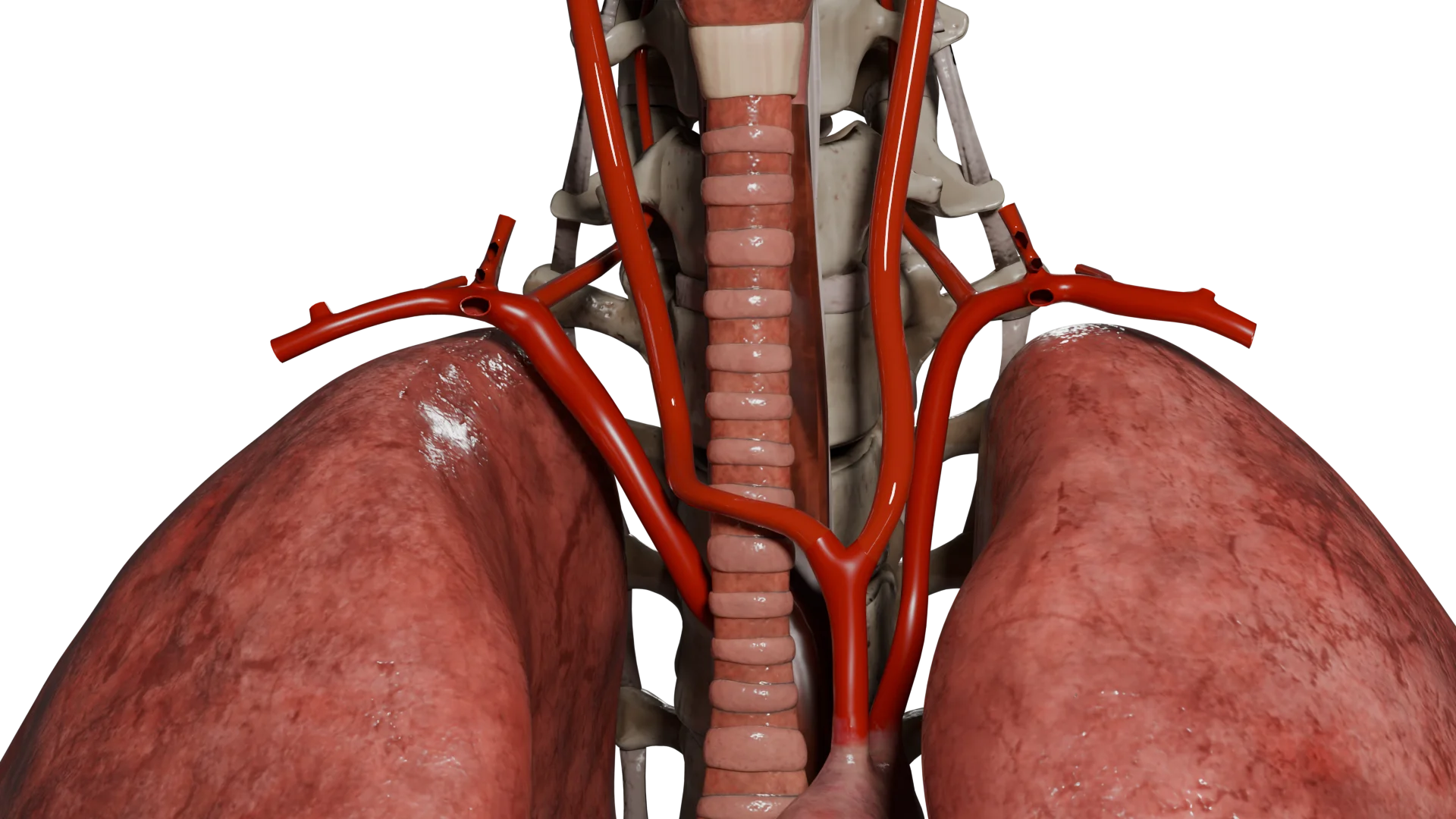
Kinking: S-shaped, C-shaped
Sharp angulated bends (typically < 90 °) develop that are usually mobile and may significantly impair blood flow. This variant is considered the most clinically significant, especially during head rotation.
3D Models of Pathological Tortuosity of Carotid Arteries:
S-Shaped Kinking of Internal Carotid Artery
C-Shaped Kinking of Common Carotid Artery
Coiling of Internal Carotid Artery
Clinical manifestations
Most cases are asymptomatic and detected incidentally. However, tortuosity can be clinically significant in some patients, presenting with:
Dizziness and presyncope, often triggered by abrupt head rotation;
Transient ischemic attacks;
Tinnitus and gait instability;
Impaired attention and memory;
Pulsatile neck mass;
Dysphagia and hoarseness.
Diagnosis
Duplex ultrasound (primary screening method):
Evaluation of vascular course and flow velocity;
Possible findings include kinking, turbulence, and flow zoning indicative of aliasing patterns
Stenosis criteria are not always applicable, unlike in cases of atherosclerosis.
CT-angiography:
Visualization of the arterial course;
Identification of the degree of deformation and its relationship to surrounding structures;
This modality is essential when planning surgery.
MR-angiography:
The method serves as an alternative to CTA when contrast media are contraindicated;
It provides valuable diagnostic information, though it is less sensitive to small regions of turbulent flow.
Cerebral Perfusion Scintigraphy or SPECT:
The method is utilized when the functional significance of tortuosity is uncertain (rarely).
Treatment of Pathological Tortuosity of Carotid Arteries
Conservative management
Risk Factor Modification:
Blood pressure control;
Body weight management;
Lipid profile adjustment and reduction of vascular inflammation;
Smoking cessation.
Medical Therapy (while it does not eliminate tortuosity, medical therapy may help prevent associated complications)
Disaggregating agents;
Antihypertensive medications;
Statins in cases of lipid profile imbalance and atherosclerosis;
Medical therapy in symptomatic patients serves as a preventive measure.
Surgical Therapy
Indications:
Symptomatic tortuosity with confirmed cerebral hemodynamic impairment;
Episodes of transient ischemia triggered by specific head positions;
Tortuosity combined with hemodynamically significant stenosis;
Failure of medical therapy in cases of functionally significant kinking.
Contraindications:
An asymptomatic disease;
Severe comorbidities;
Marked arterial calcification and elevated surgical risk.
Most commonly, the extracranial segment of the internal or common carotid artery is accessed via a standard cervical approach, involving a longitudinal incision along the anterior border of the sternocleidomastoid muscle.
In cases of high carotid bifurcation, an extended approach may be required, which may include mobilization or partial transection of the superior edge of the sternocleidomastoid muscle.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Basic Repair Methods
1. Resection of the tortuous segment with end-to-end anastomosis
The method requires sufficient vessel length to ensure a tension-free anastomosis.
2. Carotid endarterectomy with arterial straightening
This surgery is indicated in cases where carotid artery tortuosity is accompanied by atherosclerosis;
The procedure may be performed using either the conventional or eversion technique;
Following plaque removal, the affected artery is reimplanted in a straighter anatomical configuration.
3. Internal carotid artery transposition
During the procedure, the tortuous ICA origin is removed and reimplanted into a more proximal segment of the CCA;
This type of surgery is preferred in cases of significant tortuosity or when resection with direct end-to-end anastomosis is not feasible.
4. Artery replacement
This surgical method is employed when an end-to-end anastomosis is not feasible following resection;
Either synthetic or autovenous grafts are used;
The method is considered a backup technique which is rarely performed, most commonly during reintervention.
Intraoperative Monitoring
Intraoperative doppler ultrasound: Assessment of blood flow velocity before and after surgical repair.
Bypass surgery: A temporary bypass used during carotid artery repair when there is a high risk of cerebral ischemia.
Neurophysiological monitoring: Whenever possible, especially during procedures involving a solitary functioning ICA.
FAQ
1. What is pathological tortuosity of the carotid artery?
This is when the normal course of the artery is impaired, resulting in a wavy, looped, or sharply angulated configuration. Such deformities may be either congenital or acquired.
2. Is carotid artery tortuosity dangerous?
In most cases, it is not. Many individuals do not develop any symptoms, and the condition is discovered incidentally. However, in certain cases, it may impair cerebral blood flow and lead to ischemic symptoms.
3. What is the difference between tortuosity, coiling, and kinking?
Tortuosity refers to mild, non-compressive bends in the vessel’s course. Coiling describes a tightly wound loop formation, while kinking denotes a sharp angulation that may reduce the vascular lumen and impair blood flow.
4. Why does an artery become tortuous?
Causes include congenital elongation of vessels, genetic connective tissue disorders, age-related changes, hypertension, and atherosclerosis.
5. Can pathological tortuosity of the carotid artery be symptomatic?
Yes, in certain cases, patients report dizziness, imbalance, and transient disturbances of speech or vision — particularly when rotating their head. Transient ischemic attacks (TIAs) may also occur.
6. How is the disease diagnosed?
Duplex ultrasound is the primary method to diagnose the condition. If necessary, CT angiography or MR angiography may be performed to clarify anatomic pathology and assess hemodynamics.
7. When is surgery indicated?
Surgical intervention is warranted in cases of pronounced tortuosity accompanied by impaired cerebral perfusion, ischemia, or insufficient collateral blood flow compensation. In asymptomatic cases, watchful waiting and management of risk factors are recommended.
8. How is surgery for carotid artery tortuosity performed?
The surgeon excises the deformed segment of the artery and connects the remaining ends, or transposes the artery to a new anatomical position. In some cases, a vascular graft is used, or a carotid endarterectomy is performed.
9. Can pathological tortuosity of the carotid artery be prevented?
Congenital forms cannot be prevented. However, the risk of progression can be reduced by controlling blood pressure, avoiding obesity, managing atherosclerosis, and monitoring vascular health.
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Coiling of the Internal Carotid Artery is Associated with Hypertension in Patients Suspected of Stroke. van Rooij JLM, Takx RAP, Velthuis BK, Dankbaar JW, de Jong PA. Clin Neuroradiol. 2021 Jun;31(2):425-430. doi: 10.1007/s00062-020-00892-4.
3.
Clinical implications of internal carotid artery tortuosity, kinking and coiling: a systematic review. M. Zenteno, F. Viñuela, L.R. Moscote-Salazar, H. Alvis-Miranda, R. Zavaleta, A. Flores, A. Rojas, A. Lee. Romanian Neurosurgery. 2014 Apr;21(1):51-60. doi:10.2478/romneu-2014-0005.
4.
Surgical Revascularization of Symptomatic Kinking of the Internal Carotid Artery. Hao JH, Zhang LY, Lin K, Liu WD, Zhang SG, Wang JY, Li G, Wang LX. Vasc Endovascular Surg. 2016 Oct;50(7):470-474. doi: 10.1177/1538574416671246.
5.
Dolichoarteriopathy (kinking, coiling,tortuosity) of the carotid arteries and cardiovascular risk factors. Prencipe G, Pellegrino L, Vairo F, Tomaiuolo M, Furio OA. Minerva Cardioangiol. 1998 Jan-Feb;46(1-2):1-7.
6.
Tortuosity, kinking, and coiling of the carotid artery: expression of atherosclerosis or aging? L Del Corso, D Moruzzo, B Conte, M Agelli, A M Romanelli, F Pastine, M Protti, F Pentimone, G Baggiani. Angiology. 1998 May;49(5):361-71. doi: 10.1177/000331979804900505.
7.
Age-Related Tortuosity of Carotid and Vertebral Arteries: Quantitative Evaluation With MR Angiography. Sun Z, Jiang D, Liu P, Muccio M, Li C, Cao Y, Wisniewski TM, Lu H, Ge Y. Front Neurol. 2022 Apr 29;13:858805. doi: 10.3389/fneur.2022.858805.




.webp)

/aortic%20dissection_main.webp)
