Galactocele: Etiology, Clinical Presentation, Diagnosis and Treatment
Svetlana D.Surgical oncologist, MD
7 min read·October 15, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Galactoceles are cystic formations filled with milk, appearing due to blockage of the lactiferous ducts during lactation, in the early period after the end of breastfeeding, as well as in the third trimester of pregnancy.
Galactocele: 3D modelLactiferous duct obstruction in galactocele3D animation: galactocele
Etiology and pathogenesis of galactocele
The main pathophysiologic mechanism of galactocele development is obstruction of the lactiferous ducts in the lactating breast.
Factors leading to obstruction may include:
Improper breastfeeding technique;
Reduced frequency of breastfeeding;
Trauma or inflammatory diseases of the breast;
Abnormalities of nipple development;
The presence of a tumor compressing the lactiferous duct.
Obstruction of the duct leads to incomplete emptying of its proximal parts and gradual enlargement of the latter with the formation of a cystic cavity filled with milk.
Clinical presentation
Clinically, a galactocele is manifested by the presence of a painless round or oval elastic mass in the breast (the most common localization is in the retroareolar region).
The size of the mass is variable, ranging from 1 to 10 cm, and may vary throughout the day, up or down, depending on the frequency and volume of feeding. Galactoceles can be single or multiple, localized in one or both breasts.
In rare cases, infection of a galactocele with the development of inflammatory complications is possible, which is clinically manifested as redness and infiltration of the skin over the formation, the appearance of local soreness and increased body temperature.
Diagnosis of galactocele
Medical history, examination and palpation of breasts;
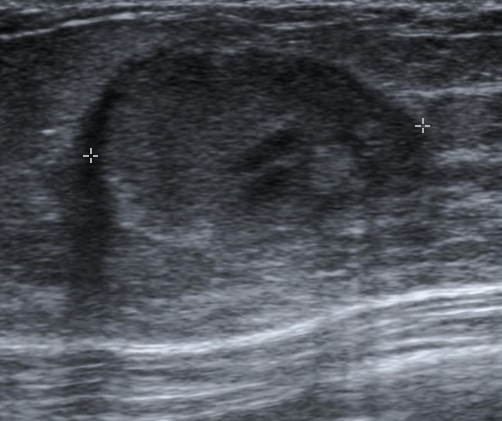
Breast ultrasound: allows visualization of non-echoic fluid-filled, avascular cystic mass;
Breast MRI: can be used as a clarifying diagnosis, is not the method of choice;
Mammography: is used very rarely due to radiation exposure and is only indicated when a malignant breast tumor is suspected;
Fine-needle aspiration biopsy of the contents of the mass under ultrasound control.
Galactocele on ultrasound. Source: Radiopaedia. Galactocele [9]
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Treatment of galactocele
In most cases, treatment of galactocele is not required, and the masses resolve on their own.
Uncomplicated form
Patients with uncomplicated galactocele are recommended to exclude the risks of traumatization and to comply with breastfeeding technique (correctly latching the baby to the breast and avoiding both too frequent pumping out and long breaks between feedings).
Larger sizes
In case of a large size of galactocele and ineffectiveness of non-surgical management, aspiration of the contents of the cystic cavity by fine-needle aspiration biopsy or drainage of the cavity with a catheter is indicated. Surgical treatments are generally not used.
Infection
In case of infection of the galactocele, drainage of the cystic cavity and antibacterial treatment are indicated.
Staphylococci and Streptococci are the most common infectious agents.
Medication therapy
First-line therapy includes antibiotics from the penicillin group (cloxacillin 500 mg 4 times a day for 10–14 days) and first-generation cephalosporins (cephalexin 500 mg 4 times a day for 10–14 days).
In case of ineffectiveness of first-line antibiotics or in the presence of relevant contraindications, clindamycin 300 mg 4 times a day for 10–14 days is recommended.
FAQ
1. What are the main symptoms and signs of galactocele?
The main sign is the presence in the breast of a painless, mobile mass of round or oval shape and elastic consistency. A typical symptom is variability in size, which may increase or decrease depending on the frequency of feeding. In rare cases of infection, there is pain, redness of the skin and an increase in body temperature.
2. What are the typical ultrasound signs of a galactocele?
On ultrasound, a galactocele is visualised as a typical cystic mass. The key ultrasound signs are: a non-echoic structure (fluid-filled), clear even contours, and no blood flow within the mass on Doppler imaging (avascularity).
3. What is the proper management strategy, and how should a galactocele be drained while breastfeeding?
The main strategy is non-surgical, aimed at ensuring adequate milk outflow. It is not advisable to make attempts to drain a galactocele by force. Instead, breastfeeding should be established and continued, paying attention to proper breastfeeding to ensure effective emptying. It is important to avoid both long breaks between feedings and excessive, too frequent pumping out.
4. Can a galactocele resolve or go away on its own?
Yes, in the vast majority of cases. Galactocele is a benign and self-resolving condition. With normalization of milk outflow and after lactation discontinuation, the formation usually resolves on its own without any medical intervention.
5. When does removal or drainage of a galactocele become necessary?
Surgical removal is generally not used. Intervention is indicated only when the galactocele is large, causing discomfort, or when non-surgical measures are ineffective. In such cases, the method of choice is a minimally invasive procedure: aspiration of the contents with a fine needle under ultrasound control. In case of infection of a galactocele, its drainage and administration of a course of antibiotics are indicated.
Medison. BI-RADS system for ultrasound: description, classification, illustrations (Система BI-RADS для УЗИ: описание, классификация, иллюстрации). \[Article in Russian] [Electronic resource].
https://www.medison.ru/si/art434.htm
4.
A. N. Sencha. Breast ultrasound. Step by step. From simple to complex. (А. Н. Сенча. Ультразвуковое исследование молочных желез. Шаг за шагом. От простого к сложному.) \[Book in Russian] 2nd edition.
5.
A. N. Sencha, Yu. V. Bikeev. Ultrasound examination of mammary glands. Atlas. (Сенча А. Н., Бикеев Ю. В. Ультразвуковое исследование молочных желез. Атлас.) \[Book in Russian]
6.
S. K. Ternovoy, A. B. Abduraimov. Radiation mammology. (С. К. Терновой, А. Б. Абдураимов. Лучевая маммология.) \[Book in Russian]
7.
Pathology Outlines. [Electronic resource].
https://www.pathologyoutlines.com
8.
Leithner D., Wengert G.J., Helbich T.H., Thakur S., Ochoa-Albiztegui R.E., Morris E.A., Pinker K. Clinical role of breast MRI now and going forward. Clinical Radiology. [Electronic resource].