Systemic Enamel Hypoplasia: Etiology, Classification, Clinical Presentation, and Treatment
Developmental Enamel Defects: Systemic Hypoplasia. Overview of the Etiology, Clinical Forms, Diagnosis, and Aesthetic Restoration Techniques for Teeth.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Enameloma is a tooth developmental anomaly that manifests as a spherical, protruding enamel mass on the root surface of a permanent or primary tooth. It is also referred to as enamel hyperplasia, enamel drop, enamel pearl, or enamel nodule.
Enamelomas are quite rare. The incidence of enamel pearls varies depending on the study method and population:
The highest incidence is observed in the permanent molars of the upper jaw.
Disruption of odontogenesis processes is the primary cause of enamel hyperplasia. The formation of enameloma is associated with the local transformation of the remnants of the enamel epithelium of Hertwig’s root sheath into enameloblasts (enamel-producing cells). Consequently, an ectopic drop of enamel develops where the root cementum should be.
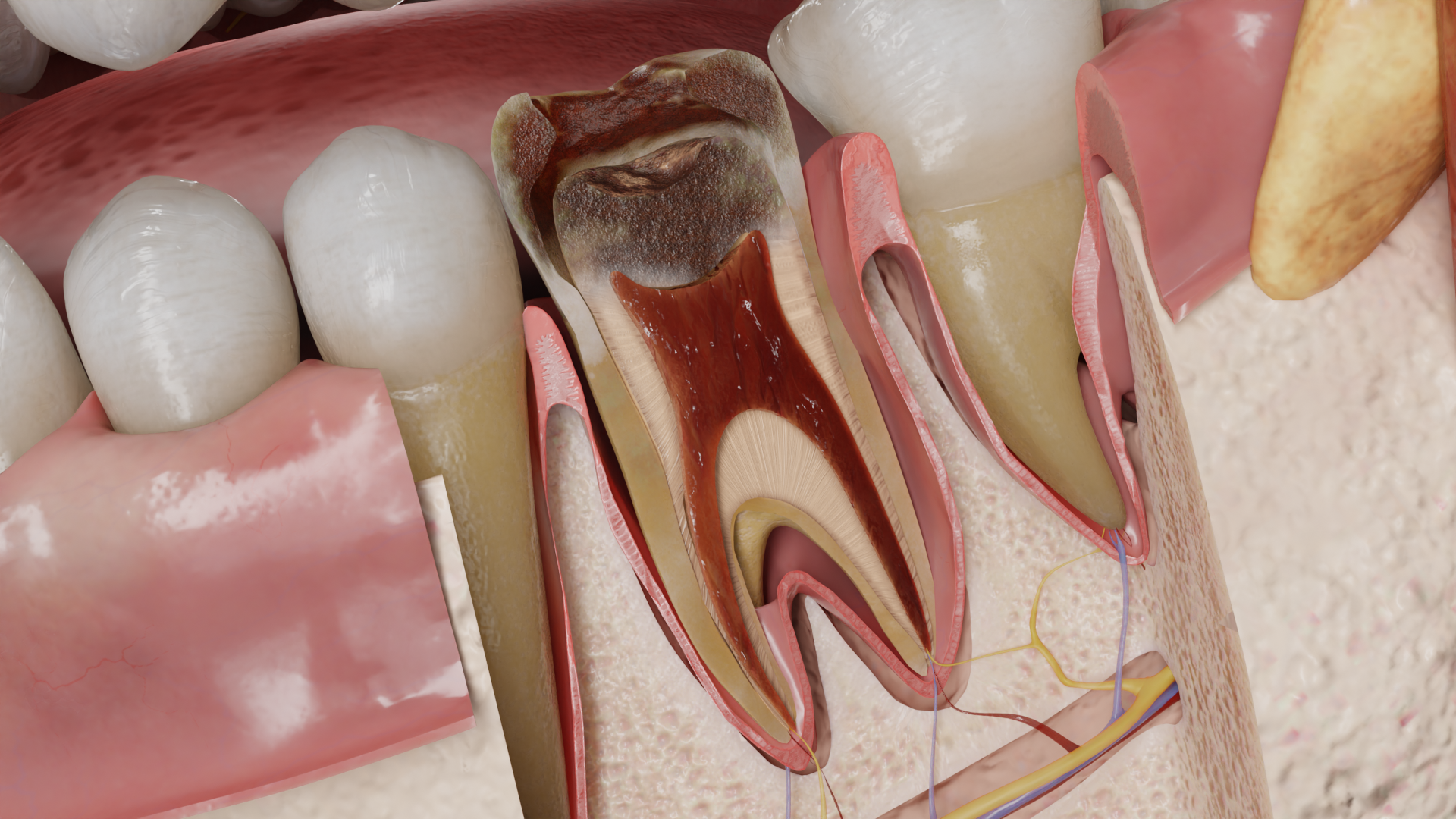
Enamel pearls prevent periodontal tissues from attaching to the root surface, create a niche for bacterial colonization and plaque retention, and make hygiene care difficult. If the enameloma is located in the area connecting with the oral cavity, it can provoke the rapid formation of a deep periodontal pocket and the development of local periodontitis. Enamelomas in the root furcation area of primary teeth can cause late replacement of primary teeth and deviation of the eruption path of the secondary teeth.

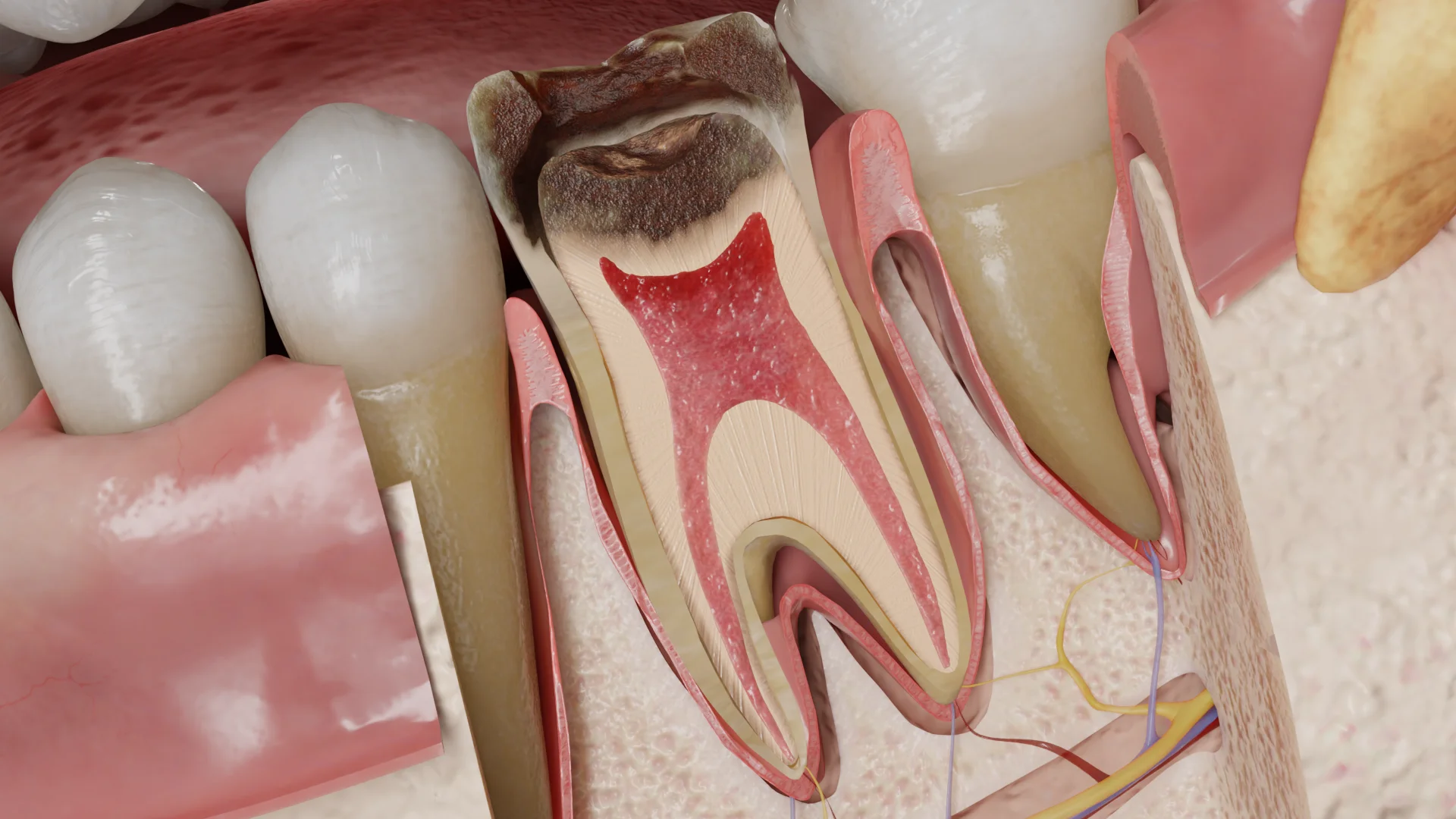
Macroscopically, enameloma appears as a round or hemispherical white formation with a smooth, shiny surface, tightly attached to the surface of the tooth root. Its size varies from 0.3 to 4.48 millimeters.
| Enameloma type | Structure description |
|---|---|
| True enamel pearls | Contain enamel only |
| Enamel-dentin pearls | Contain dentin core coated with enamel |
| Enamel-dentin-pulp pearls | Contain pulp, which is often associated with the pulp cavity or root canal of the tooth |
Most often, this abnormal finding is localized:
Also, in rare cases, enamelomas can be found on the tooth crown or in the coronal, middle, or apical third of the tooth root.
Most commonly, enamelomas occur in the furcation areas of maxillary molars, between the distobuccal and the palatal roots. Large enamel pearls most often develop on the lower molars and may contain pulp. Enamelomas of maxillary molars are smaller in size but there may be several of them on one tooth. The cases of bilateral development of multiple enamelomas on all maxillary molars have been documented.
On premolars, canines, and incisors, enamelomas are quite uncommon. Sometimes enamel pearls are found in combination with other pathological masses (fibrous epulis, etc.).

An enamel pearl may be completely asymptomatic.
If an enameloma has caused the development of a periodontal pocket, the patient may complain of the following:
Clinically, a hemispherical, solid, white mass with a smooth surface on the tooth neck or bifurcation can be detected. In the event of concomitant local periodontitis, the gums around the mass are swollen and hyperemic and bleed when probing, and the depth the periodontal probe is placed into the gingival sulcus is 4 mm or more.
Enamelomas can be clinically diagnosed visually on examination, during gingival retraction, periodontal probing, or tooth extraction surgery.
The main diagnostic approach is radiological, using the following methods:
Radiographic findings: the radiograph shows a clearly defined, hyperintense, rounded shadow in the projection of the tooth neck, on the root surface, or in the furcation area of the tooth root. If the pulp is part of the mass, a radiolucency area may be detected in the center of the mass.
Enameloma requires treatment if it is located in an area accessible to oral microflora penetration and biofilm formation.
The mass is excised using a diamond bur, the surface is ground and polished, and remineralizing therapy is administered. The patient should also be motivated to maintain oral hygiene carefully.
Possible complications of the mass excision:
1. What is enameloma and why does it develop?
2. How common are enamel pearls?
3. What are the risks of enamel pearl?
4. How is enameloma diagnosed?
5. Does enameloma require treatment, and if so, what kind?
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Grine FE, Holt S, Brink JS, Du Plessis A. Enamel pearls: Their occurrence in recent human populations and earliest manifestation in the modern human lineage. Archives of Oral Biology [Internet]. 2019 Mar 16;101:147–155.
Available from: https://doi.org/10.1016/j.archoralbio.2019.03.004
3.
Zenóbio EG, Vieira TR, Bustamante RPC, Gomes HE, Shibli JA, Soares RV. Enamel Pearls implications on periodontal disease. Case Reports in Dentistry [Internet]. 2015 Jan 1;2015:1–3.
Available from: https://doi.org/10.1155/2015/236462
4.
Chrcanovic BR, Abreu MHNG, Custódio ALN. Prevalence of enamel pearls in teeth from a human teeth bank. Journal of Oral Science [Internet]. 2010 Jan 1;52(2):257–260.
Available from: https://doi.org/10.2334/josnusd.52.257
5.
Moharir AN, Akkottillam M, Bhagat S, Pagare V, Hakkepatil A, Bagde H. Enamel Pearls: A Culprit of Localised Periodontitis. Journal of Pharmacy and Bioallied Sciences [Internet]. 2025 Jun 1;17(Suppl 2):S2007–S2009.
Available from: https://doi.org/10.4103/jpbs.jpbs_566_25




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io