Systemic Enamel Hypoplasia: Etiology, Classification, Clinical Presentation, and Treatment
Developmental Enamel Defects: Systemic Hypoplasia. Overview of the Etiology, Clinical Forms, Diagnosis, and Aesthetic Restoration Techniques for Teeth.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Caries is an infectious process of demineralization and destruction of the hard tissues of teeth.
Caries develops when several factors combine: dental plaque microflora, easily fermentable dietary carbohydrates, a caries-susceptible tooth, and prolonged exposure time.
Microorganisms colonize tooth surfaces not subject to friction from the tongue, cheeks, and food fibers, forming a biofilm known as dental plaque. Carious lesions develop only in areas where plaque accumulates.
Frequent and prolonged consumption of easily fermentable carbohydrates increases the proportion of cariesogenic microflora in the biofilm, which can rapidly metabolize food carbohydrates to form organic acids and can also survive in low pH conditions. These are primarily Streptococcus mutans and Lactobacilli, but also Streptococcus sobrinus, Streptococcus oralis, Actinomyces israelii, Actinomyces gerencseriae, Bifidobacteria, and Prevotella. Streptococcus mutans also synthesize intra- and extracellular adhesive polysaccharides (glucans and fructans) that promote prolonged retention of bacteria on tooth surfaces.
Teeth are constantly bathed in saliva containing mineral substances. Saliva, due to its buffering capacity, helps maintain a neutral pH in the oral cavity. At neutral pH values (≈7), the processes of demineralization (dissolution of mineral component crystals) and remineralization (partial or complete restoration of mineral component crystals) of enamel and dentin are in equilibrium.
Bacterial metabolism of dietary carbohydrates (glucose, fructose, sucrose, maltose, and others) leads to acid accumulation and pH reduction.
If the pH drops low enough (5.2-5.5), minerals from the hard tissues of the tooth begin to dissolve. Gradual loss of minerals due to acid-induced dissolution (demineralization) is the main process in caries development.
The more frequently carbohydrates enter the oral cavity with food and the longer food debris remains on tooth surfaces, the more acid bacteria produce, lowering pH and progressing enamel demineralization. Upon reaching the dentin, in addition to continued acid production, bacteria also begin proteolytic activity. As a result, the organic component (collagen) of dentin is destroyed.
Caries progression can be slowed or stopped by reducing the frequency and duration of acid attacks, for example, by improving hygiene or limiting sugar consumption. Fluoride compounds promote remineralization processes and slow demineralization, reduce enamel solubility, and enhance its resistance to acid attacks.
3D models of caries by depth of lesion:
 Caries stages according to the radiological classification – stage E1
Caries stages according to the radiological classification – stage E1 Caries stages according to the radiological classification – stage E2
Caries stages according to the radiological classification – stage E2 Caries stages according to the radiological classification – stage D1
Caries stages according to the radiological classification – stage D1 Caries stages according to the radiological classification – stage D2
Caries stages according to the radiological classification – stage D2 Caries stages according to the radiological classification – stage D3
Caries stages according to the radiological classification – stage D33D models of caries by lesion localization:
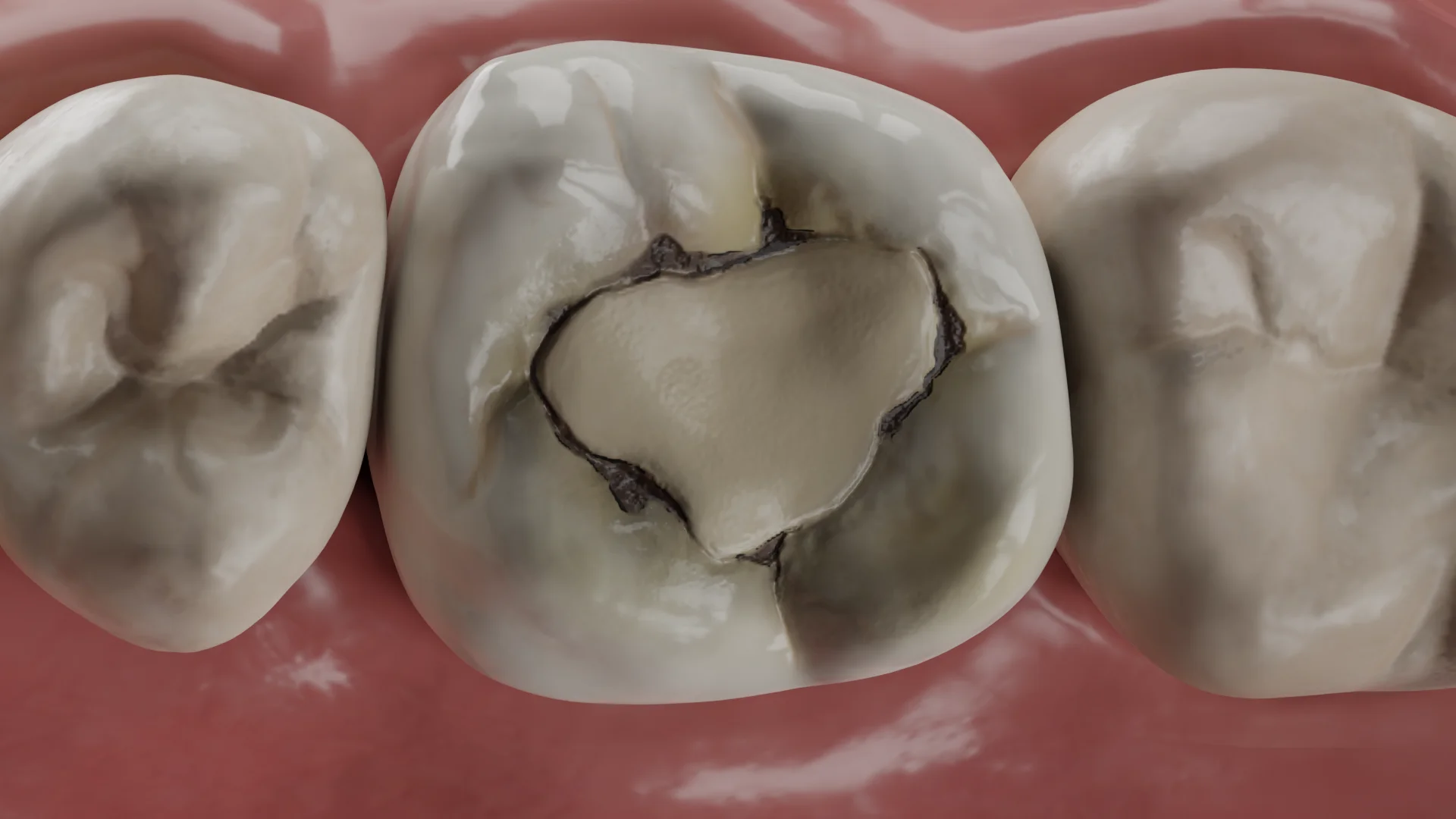
 Localization of carious cavities according to Black’s classification – class I
Localization of carious cavities according to Black’s classification – class I  Localization of carious cavities according to Black’s classification – class II
Localization of carious cavities according to Black’s classification – class II Localization of carious cavities according to Black’s classification – class III
Localization of carious cavities according to Black’s classification – class III Localization of carious cavities according to Black’s classification – class IV
Localization of carious cavities according to Black’s classification – class IV Localization of carious cavities according to Black’s classification – class V
Localization of carious cavities according to Black’s classification – class V Carious lesion always begins on the tooth surface that directly contacts the oral cavity: on the enamel surface, exposed root cementum, or exposed dentin. Caries more often develops in typical areas of plaque accumulation – in pits and fissures, on the lateral surfaces of teeth, in the cervical area. With high caries activity and insufficient hygiene, ‘immune zones’ can be affected by caries – smooth surfaces, the equator zone, and cusps.
Enamel caries: at the initial stage, after removing plaque and drying the tooth, the enamel macroscopically appears intact, with a focus of demineralization visible as a matte white spot (E1). At a later stage (E2), the white spot is noticeable even on the moist enamel surface. The spot can be stained in various shades of brown by food dyes. In the enamel, the lesion has the shape of a cone with its apex directed towards the enamel-dentin junction (EDJ). When the process reaches the EDJ and penetrates the dentin, the further direction of the lesion spread corresponds to the course of dentinal tubules.
Dentin caries: demineralized enamel in the defect area may remain intact (pseudo-intact enamel), preventing bacteria from penetrating the demineralization focus. Macroscopically, such a defect looks like a pigmented fissure or spot on the enamel surface, under which darker contours of the affected dentin may be discerned.
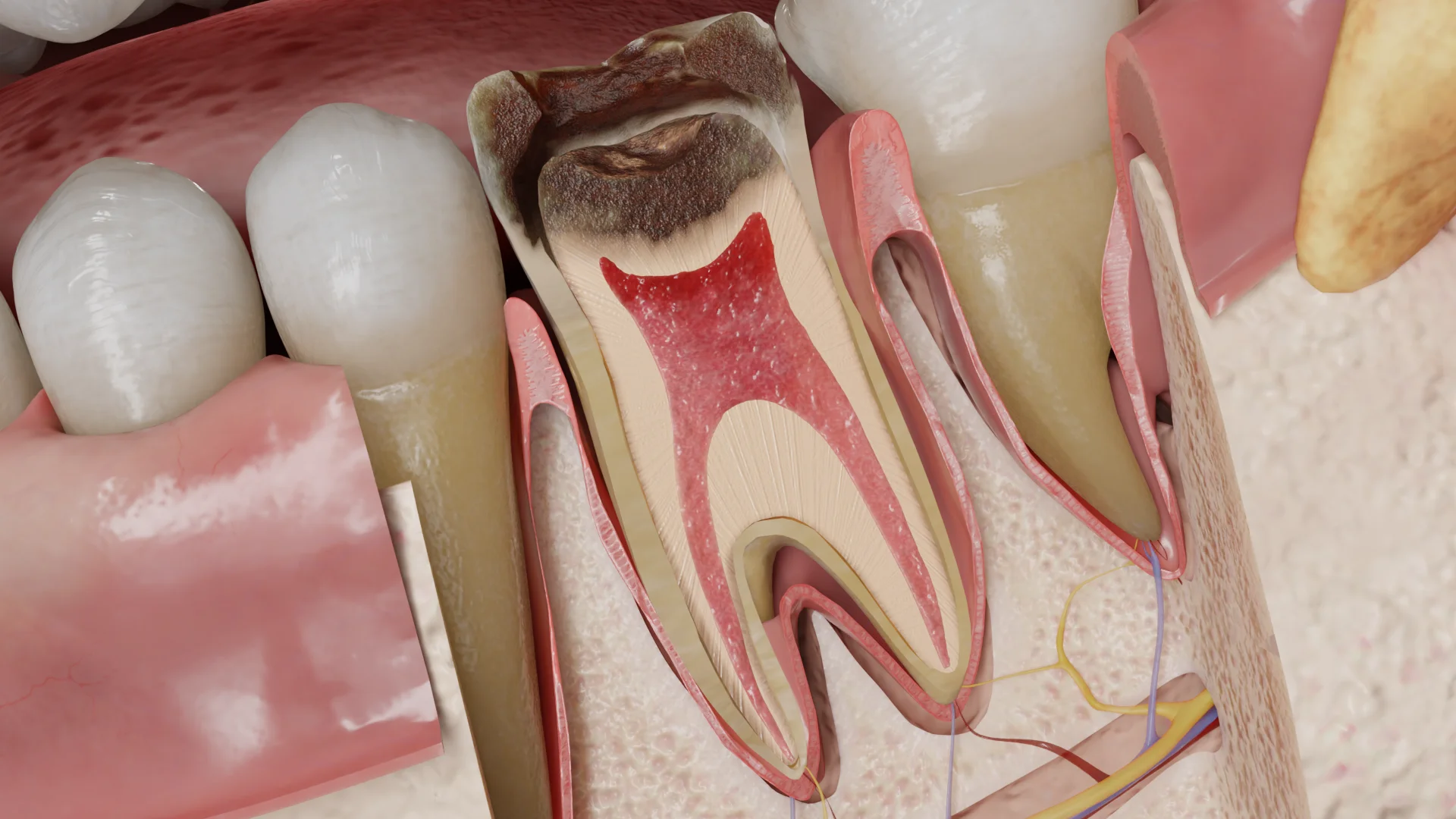
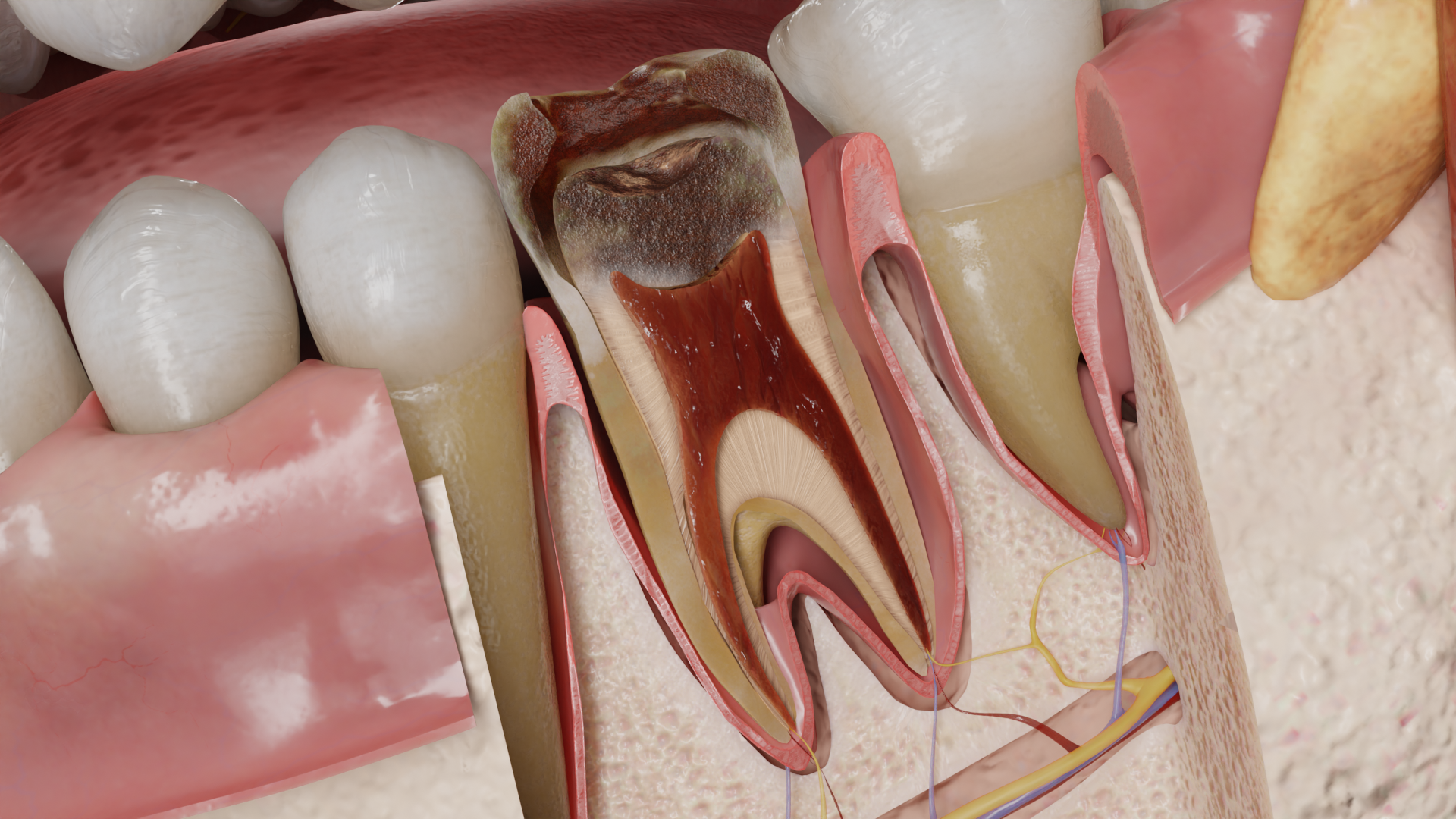
When about 30-40% of minerals in the enamel lesion focus are lost, it becomes so porous and fragile that it can easily break and form a cavity-like defect. Bacteria rush deep into the defect, under the influence of their proteases, the demineralized dentin becomes necrotic (bacterial penetration zone), and the demineralization zone spreads deeper towards the pulp. Around the demineralization focus, reactive dentin sclerosis occurs. The outer (D1), middle (D2), and inner (D3) thirds of dentin are sequentially affected. Macroscopically, an active lesion looks like a cavity filled with soft, sticky, yellowish-brown necrotic dentin that is easily removed by scraping. In a stalled lesion, the affected dentin is denser and darker.
Cementum caries in the form of a cavity filled with softened dentin develops on the tooth root surface in the presence of gingival recession and exposed root cementum. Its development follows the same mechanisms as crown caries.

Secondary caries develops as linear staining, a spot, or cavity at the border between tooth tissues and restoration with compromised marginal integrity. This type of lesion consists of a surface area of demineralization at the enamel-restoration interface, and a ‘wall’ lesion between the restoration and the cavity. The surface focus spreads along the enamel prisms towards the EDJ and then along the dentinal tubules. The ‘wall’ lesion is a narrow slit-like cavity, later spreading along the dentinal tubules and in the lateral direction.
Enamel caries (E1, E2) do not cause complaints; the patient may be concerned about the aesthetic defect. Clinically, a white or pigmented spot on the enamel is detected.
Dentin caries (D1–D3), cementum caries, secondary caries: complaints may be absent, the patient may be concerned about the presence of a cavity in the tooth or an aesthetic defect, short-term localized pain in the tooth from chemical, thermal, mechanical irritants, food getting stuck and difficulties when using dental floss. Clinically, pigmentation of the pit or fissure, borders of the old restoration, probe getting stuck in them (Black’s Class I, secondary caries), gray shadow under the marginal ridge, inflammation of the interdental papilla adjacent to the affected tooth, food debris in the interdental space (Class II), dark spots when illuminating teeth (Class II, III), visible carious cavities filled with softened dentin (Classes I–V, cementum caries) are detected.
Find more scientifically accurate content on our social media








Enamel caries — for non-cavitated defects, remineralizing therapy, infiltration method, correction of home hygiene care, recommendations for rational nutrition, and dynamic observation are applied.
Dentin caries, cementum caries, secondary caries — tooth tissue preparation and filling of the carious cavity using dental restorative materials.
1. What microorganisms cause caries development?
2. How does enamel caries differ from dentin caries?
3. What are the main methods of caries treatment?
4. Caries and pulpitis: what are the differences?
Pulpitis is a complication of caries, in which inflammation of the tooth pulp (nerve and blood vessel bundle) develops. Pulpitis is accompanied by severe, often radiating pain, which can occur spontaneously, without external stimuli.
Main differences:
1. Localization:
• Caries affects enamel and dentin;
• Pulpitis affects the pulp of the tooth.
2. Symptoms:
• Caries: short-term pain occurs only when exposed to stimuli (cold, hot, sweet);
• Pulpitis: prolonged (more than 5 seconds) pain occurs when exposed to temperature stimuli, spontaneous pain is possible, pain irradiation.
3. treatment:
• Caries: preparation and filling, remineralizing therapy;
• Pulpitis: root canal treatment (endodontic treatment).
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Toumba, K. J., Twetman, S., Splieth, C., Parnell, C., Van Loveren, C., Lygidakis, N. Α. (2019). Guidelines on the use of fluoride for caries prevention in children: an updated EAPD policy document. European Archives of Paediatric Dentistry, 20(6), 507–516.
https://doi.org/10.1007/s40368-019-00464-2
3.
Meyer-Lueckel, H. (2013). Caries management: Science and Clinical Practice. Thieme Medical Pub.
4.
Li, M. (2012b). Contemporary approach to dental caries. IntechOpen.
5.
Xuedong, Z. (2016). Dental caries: Principles and Management. Springer.
6.
Kidd, E. a. M., Fejerskov, O. (2016). Essentials of dental caries. Oxford University Press.
7.
Eden, E. (2018). Evidence-Based caries prevention. Springer.
8.
De Olivera Carrilho, M. R. (2017). Root caries: From Prevalence to Therapy. Karger Medical Scientific.
9.
Askar, H., Krois, J., Göstemeyer, G. et al. Secondary caries: what is it, and how it can be controlled, detected, and managed?. Clin Oral Invest 24, 1869–1876 (2020).
https://doi.org/10.1007/s00784-020-03268-7
10.
Askar H, Tu YK, Paris S, Yeh YC, Schwendicke F. Risk of caries adjacent to different restoration materials: Systematic review of in situ studies. J Dent. 2017 Jan;56:1-10. doi: 10.1016/j.jdent.2016.09.011.
Loading test 6 questions
Table of Contents




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io