Skin Biopsy in Dermatology: Classification, Technique, and Diagnostic Value
Skin biopsy. This article covers punch, shave, and excisional techniques, specimen handling and fixation, and the role of biopsy in dermatology and oncology.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
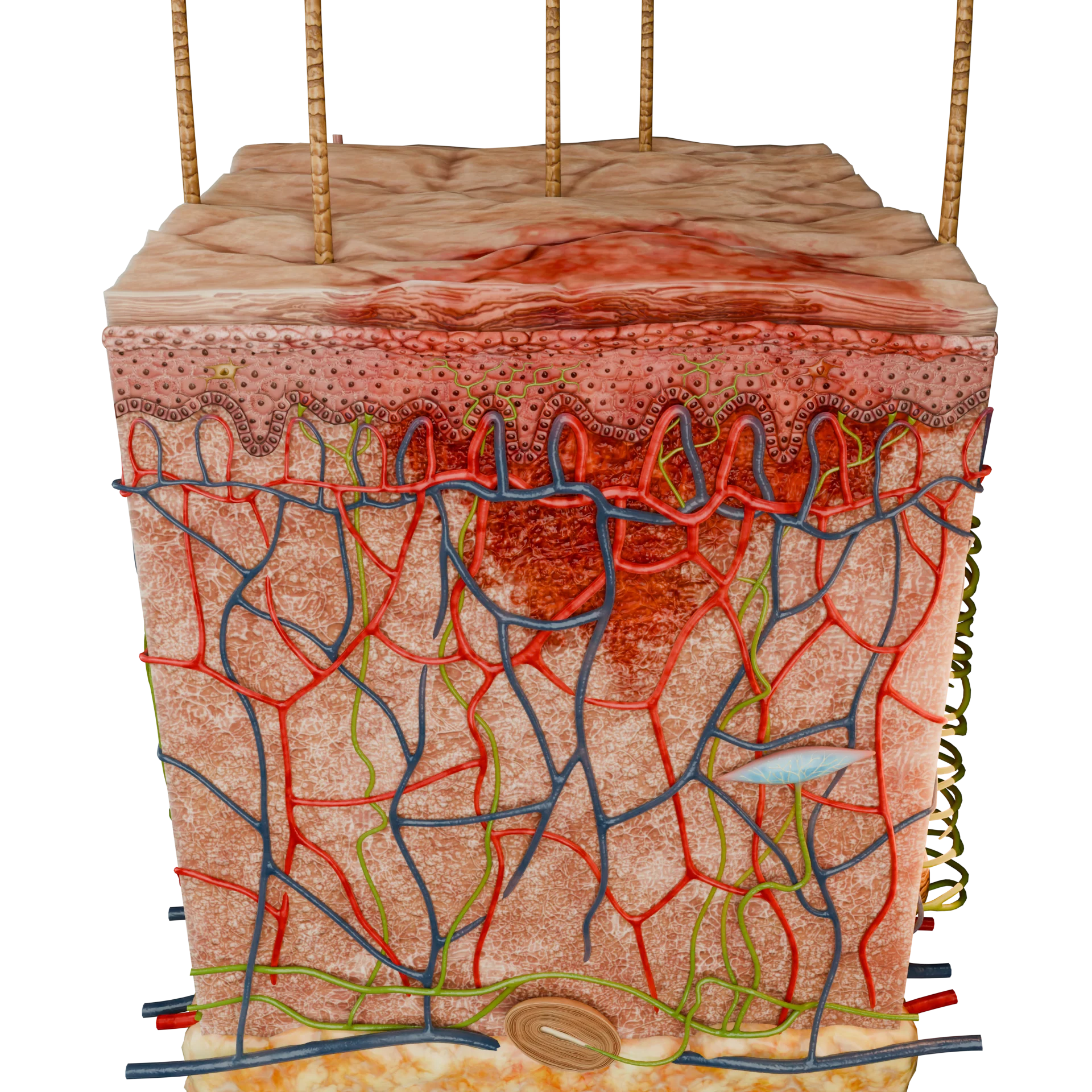
Primary morphologic elements are represented by changes in the skin and mucous membranes, which appeared as a result of various pathologic processes in the unchanged skin and mucous membranes.
Three primary cavity morphologic elements are distinguished:
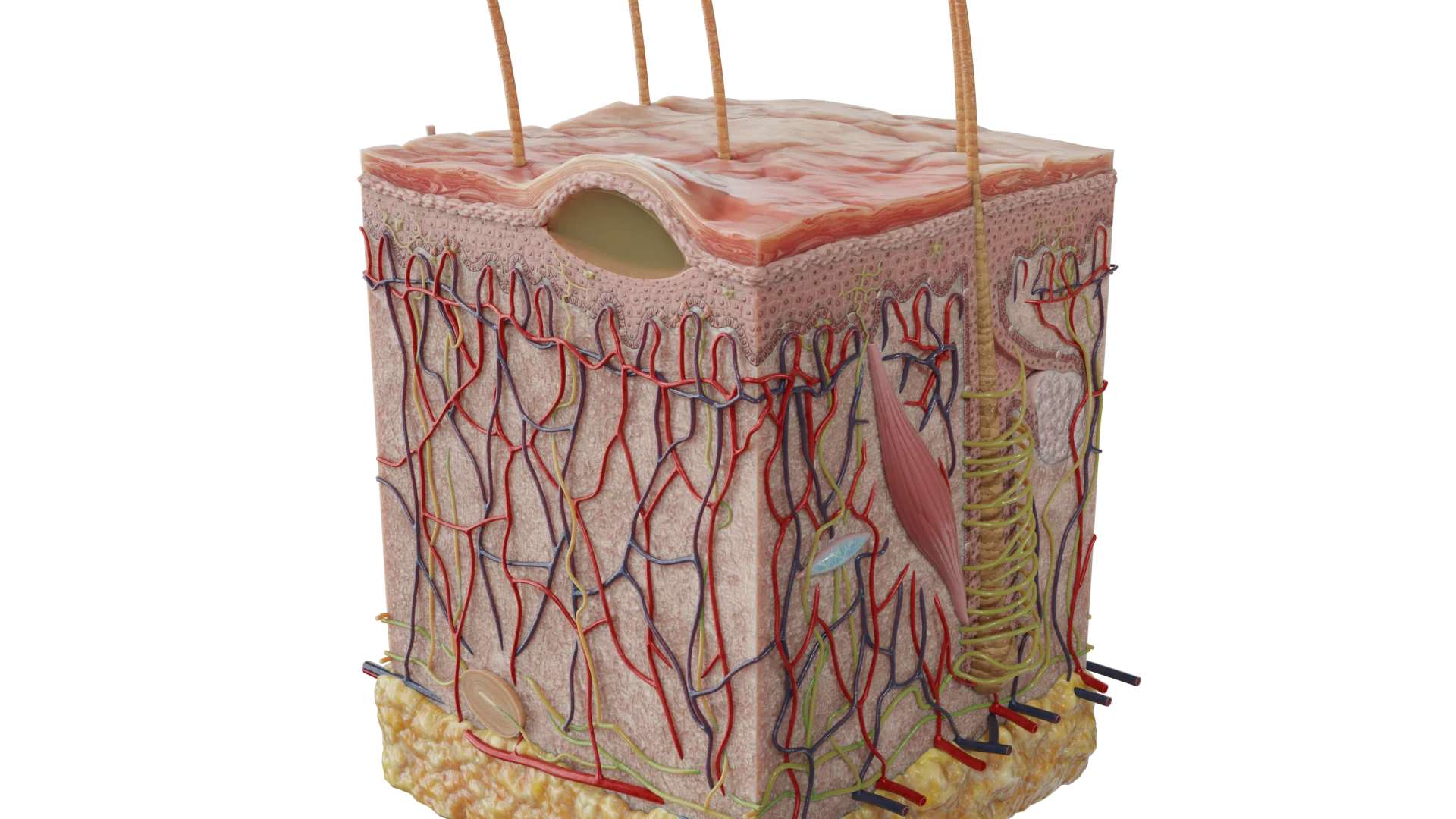
A vesicle is a cavitary primary exudative morphologic element that is a small (up to 0.5 cm) fluid-filled mass located in the upper layers of the epidermis. It has a hemispherical shape with clear boundaries and consists of a covering, a cavity with contents and a bottom. The vesicles may be located in isolation or in groups.
In the process of development of vesicles can open and form erosions and wetting, which are covered with crusts and later fall off, sometimes leaving behind a hyperpigmented spot, which then passes without trace.
By depth of location:
By the nature of the contents:
Vesicles are characteristic of herpes skin lesions (herpes simplex and shingles), allergic and contact dermatitis, eczema, impetigo, dyshidrosis, burns, and some autoimmune processes (e.g., Duhring’s dermatitis herpetiformis).
A bubble is a cavitary primary exudative morphologic element that is a mass greater than 0.5 cm in diameter filled with fluid (serous, hemorrhagic, or purulent). It is located in the epidermis, at the border with the dermis or in the subcutaneous tissue. It has a dense covering, clear boundaries and consists of:
The bubbles may be single-chambered or multi-chambered, arranged in isolation or in groups.
In the process of development, blisters may shrink when the contents are resorbed, open with the formation of erosions or ulcers covered with crusts, and in case of deep location – to leave behind scars or areas of hyperpigmentation.
By depth of location:
By the nature of the contents:
Blisters are characteristic of autoimmune diseases (vesicles, pemphigoid), infections (bullous impetigo, herpes), toxic-allergic reactions, trauma and burns.
A pustule is a cavitary primary morphologic element that is a mass up to 0.5-1 cm filled with purulent contents (leukocytes, bacteria, detritus). Located in the epidermis, dermis, or around the hair follicle. It has distinct borders, an inflammatory corolla and consists of:
Pustules can be superficial (heal without scarring) or deep (leave scarring).
In the process of development, pustules open with the release of pus, after which erosions are formed, covered with a crust. In deep lesions, they can form ulcers that subsequently scar.
Find more scientifically accurate content on our social media








Classification of pustules
By localization:
Depth:
Pustules are characteristic of bacterial infections (staphylococcal, streptococcal pyoderma), inflammatory dermatoses (acne, rosacea), autoimmune processes (pustular psoriasis), fungal and viral infections (herpes, candidiasis).
1. What is the main difference between a vesicle, blister, and pustule?
2. What diseases are most often accompanied by vesicles?
3. When do blisters pose a serious health risk?
4. What diagnostic methods are used for cavitary elements?
5. How to prevent scarring after opening cavity elements?
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Carter KF, Dufour LT, Ballard CN. Identifying secondary skin lesions. Nursing. 2004 Jan;34(1):68. doi: 10.1097/00152193-200401000-00060. PMID: 14738076.
3.
An Approach to Primary Lesions. In: Burgin S. eds. Guidebook to Dermatologic Diagnosis. McGraw-Hill Education; 2021. Accessed April 01, 2025.
4.
Soutor C, Hordinsky MK. eds. Clinical Dermatology: Diagnosis and Management of Common Disorders, 2e. McGraw-Hill Education; 2022. Accessed April 04, 2025.
5.
Wafaa Binti Mowlabaccus et al, Common benign skin lesions DermNet (from the web), July 2020.
6.
Hunter JAA, Savin J, Dahl MV. Clinical Dermatology / J.A.A. Hunter, J.A. Savin, M.V. Dahl. 3rd ed. Blackwell Science; 2002.




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io