Systemic Enamel Hypoplasia: Etiology, Classification, Clinical Presentation, and Treatment
Developmental Enamel Defects: Systemic Hypoplasia. Overview of the Etiology, Clinical Forms, Diagnosis, and Aesthetic Restoration Techniques for Teeth.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
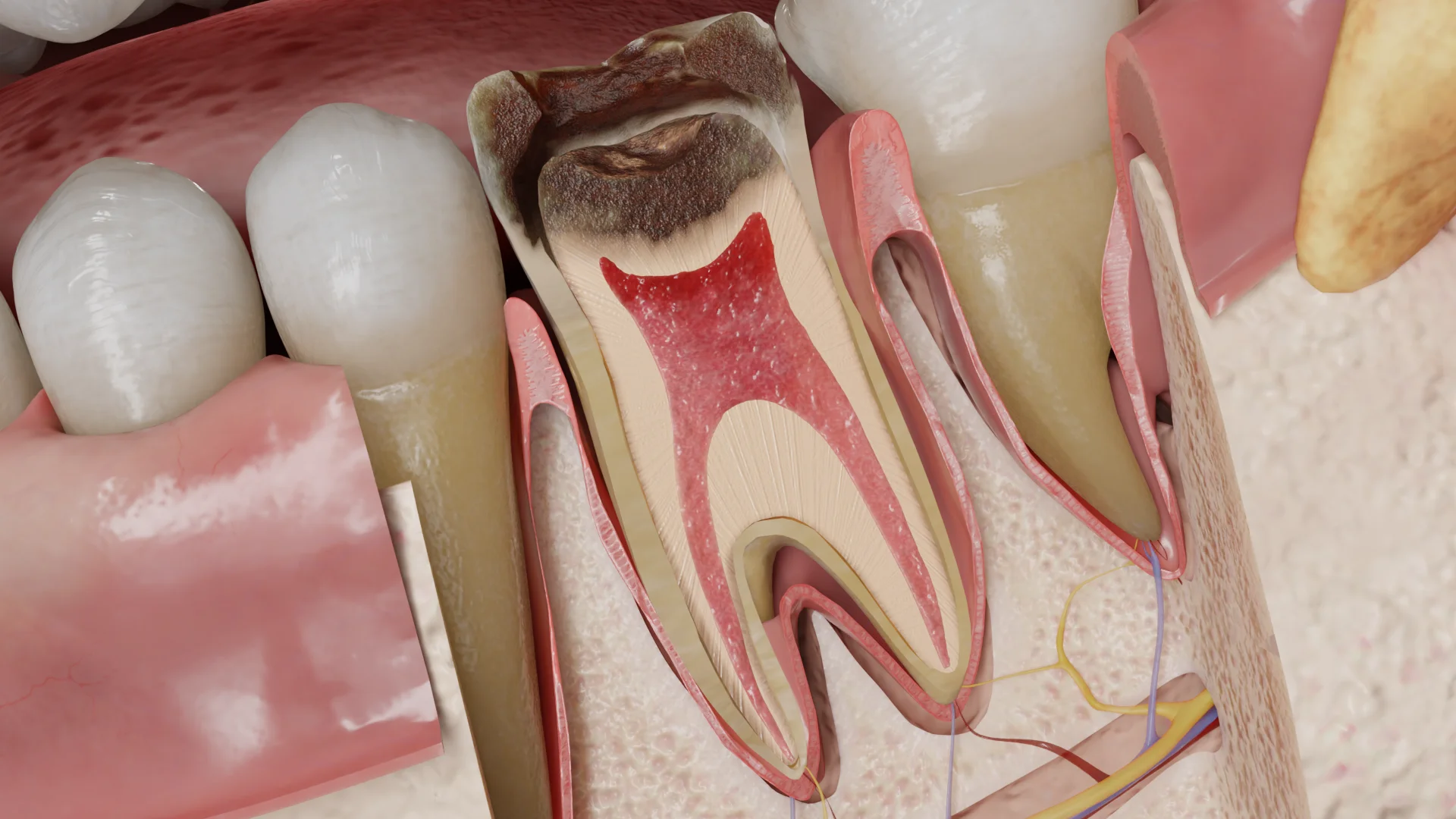
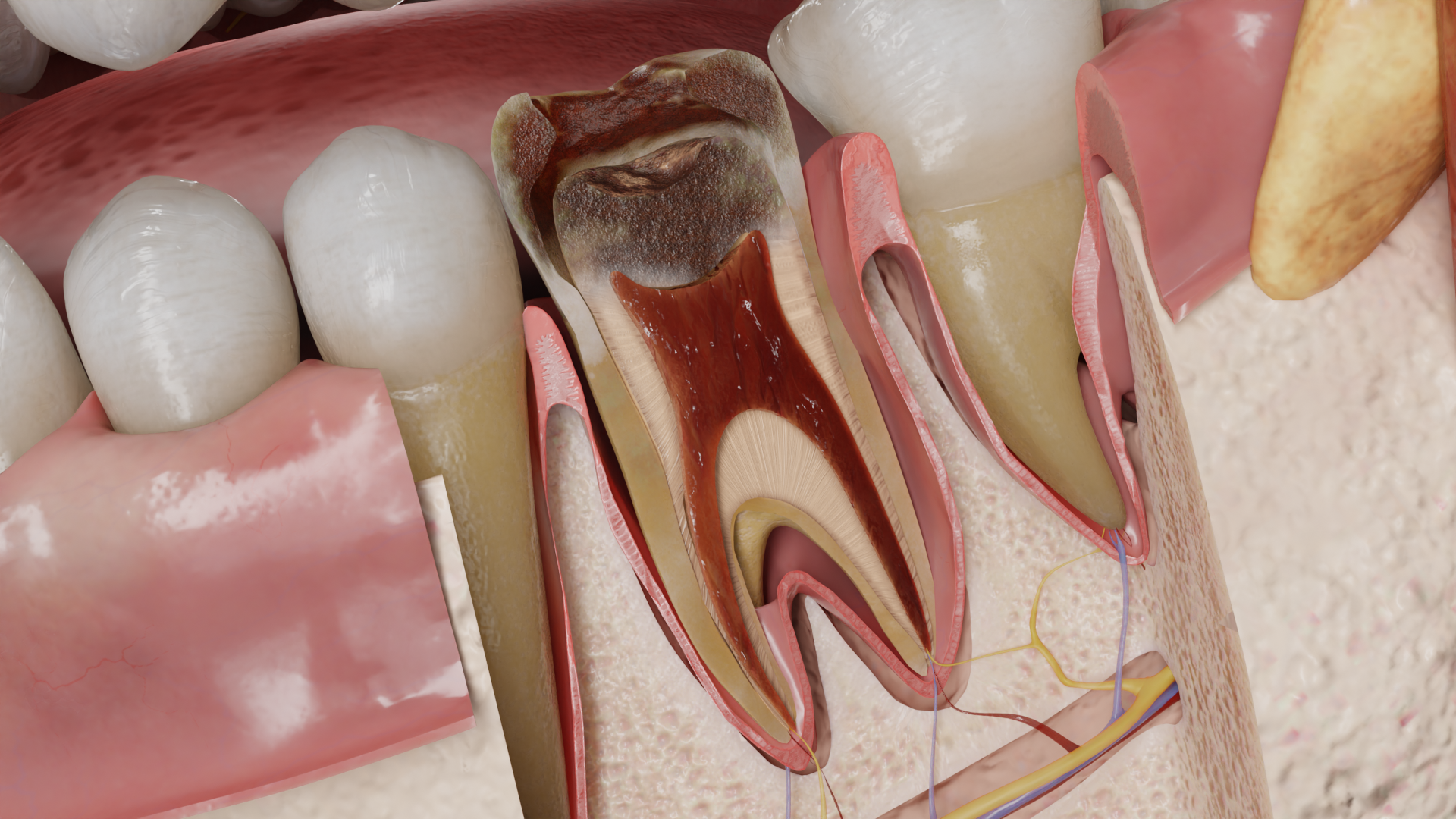
An apical abscess is a purulent inflammation of the periapical tissues in response to massive escape of virulent bacteria from the root canal system of a tooth.
Acute apical abscess may develop primary as an outcome of acute apical periodontitis, be the result of exacerbation of chronic inflammation in the periapical area.
The etiologic factor is invasion of pyogenic microflora from the root canals of the tooth into the inflamed periapical tissues (extra-radicular infection). The microflora of apical abscess is mixed, Gram-negative anaerobic bacilli and peptostreptococci predominate.
The predominant effector cells in an acute apical abscess are polymorphonuclear neutrophilic leukocytes. After phagocytic activity of these cells and their death, a large number of tissue-destroying elements (hydrolases and oxygen radicals) appear, macrophages can no longer cope with cell cleansing and repair. Destruction of the periodontal ligament and bone in the area of the root apex occurs.
Bone loss is caused by activated osteoclasts, resorption is accompanied by immune cell invasion. There may also be direct invasion of microorganisms from root canals, which gradually causes tissue destruction.
Chronic apical abscess is characterized by a long-lasting purulent inflammatory process that drains through a fistulous passage. The inflammatory process perforates the cancellous bone and one of the cortical laminae and creates a draining fistulous passage that allows for the constant discharge of the resulting pus.
Depending on the etiologic factor, the affected tooth may exhibit:
The pulp of the tooth is necrotic, yellowish-gray or gray-black in color.
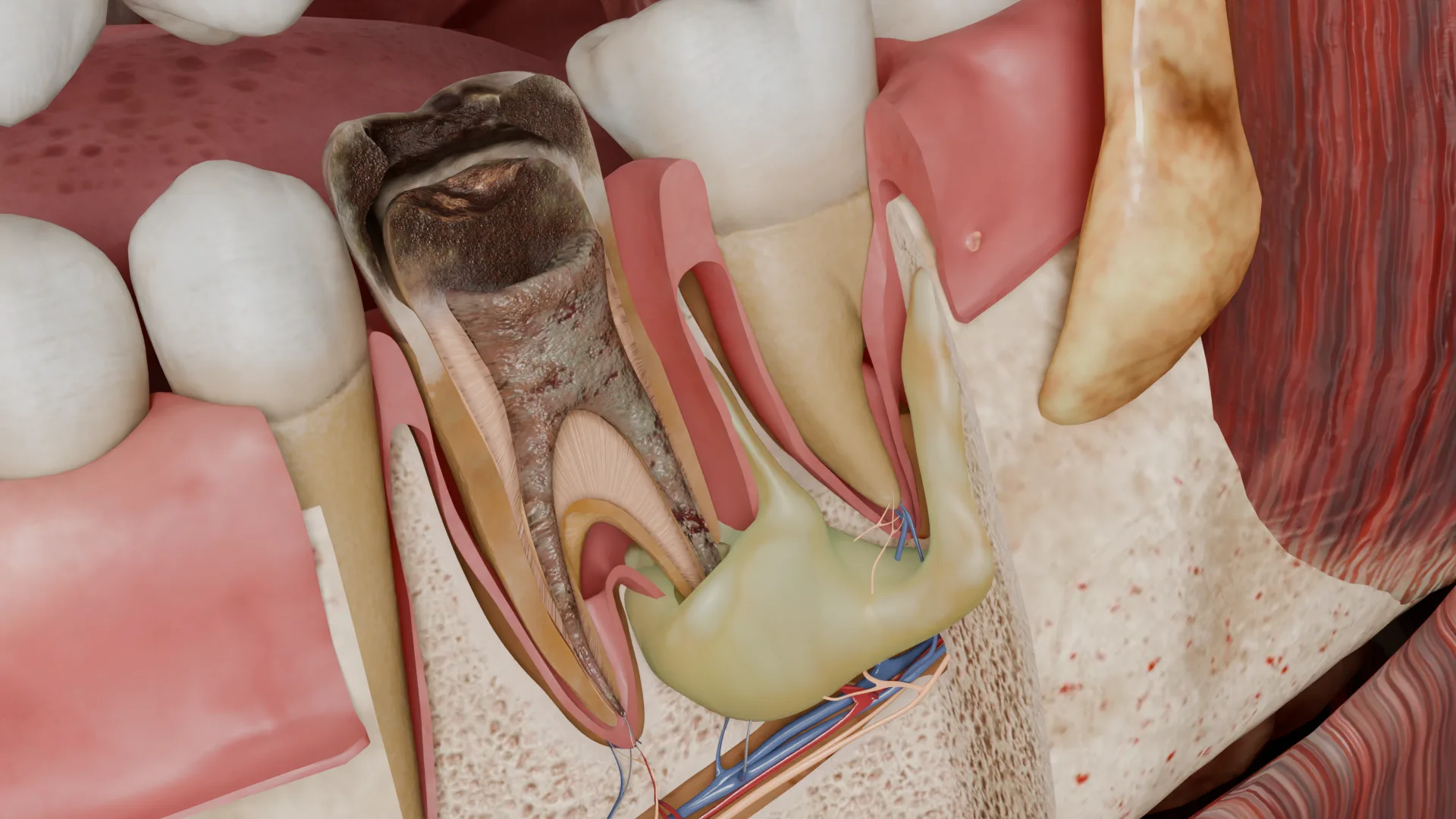
In acute apical abscess in the area of the root apex, an area of destruction of the periodontal ligament and alveolar bone filled with purulent exudate and surrounded by fibrovascular granulation tissue is determined.

In chronic apical abscesses, the process penetrates the cancellous bone, compact lamina, mucosa or skin and a fistulous passage is formed. The opening of the fistulous passage is a convex rounded soft tissue mass with a hole in the center from which purulent exudate is released. Fistulous passage can open as close to the focus of infection, and at a distance from it: vestibularly or lingually on the mucosa of the alveolar process, on the attached gingiva. Sometimes the fistulous passage may run along the root of the tooth and open into the gingival sulcus or furcation zone.
In this case, a deep narrow false pocket develops, masquerading as a periodontal pocket or a symptom of a vertical root fracture. Also, the opening of the fistulous passage can open into the nasal cavity, the maxillary sinus, on the skin of the face, neck.
Internally, the fistulous passage may be completely or partially lined with epithelium surrounded by inflamed connective tissue.
The patient complains of localized pain in the area of one of the teeth, of moderate or high intensity, intensified by biting on the tooth of the cause, a feeling of pressure or a feeling of a “grown tooth”. Visualization of the tooth reveals a deep carious cavity, restoration or traumatic defect penetrating into the pulp chamber. Percussion of the tooth is sharply painful, palpation of the transitional fold can also be painful, with the involvement of the cortical plate may be present swelling and hyperemia of the mucosa in the projection of the root apex. The depth of periodontal probing is within normal limits (1-3 mm). The mobility of the tooth can be determined. There is no reaction to temperature and electrical stimuli. In addition, there may be systemic manifestations of the infectious process: increased body temperature, increased lymph nodes of the submandibular and chin area, leukocytosis.
In chronic apical abscess, the patient may not report any complaints, or may indicate the presence of a mass or localized swelling on the gingiva.
A tooth with a deep carious cavity, restoration or traumatic defect penetrating the pulp chamber. Percussion of the tooth is usually painless or mildly painful. Palpation of the transitional fold is painless. On the mucous membrane or skin is determined by the opening of the fistulous passage, from which purulent exudate is released. With obstruction of the fistulous passage may develop local swelling of soft tissues.
Find more scientifically accurate content on our social media








Endodontic treatment of the tooth is performed: extirpation of non-viable pulp or removal of old filling material from the root canals, mechanical treatment and irrigation of root canals. In the presence of exudate in the root canals, fistulous passage, it is recommended to use temporary intracanal attachments. Drainage of purulent exudate is carried out through the root canals or through the cortical plate of the jaw in the projection of the lesion. In the future, a hermetic obturation of root canals with subsequent restoration of the tooth is performed.
If access to the source of infection is difficult, in addition to conservative endodontic treatment, microsurgical methods (periradicular curettage, resection of the root apex with retrograde filling, root amputation), intentional replantation may be used.
If the prognosis of endodontic treatment is unsatisfactory, the tooth should be extracted.
Antibiotic prophylaxis during non-surgical and surgical endodontic treatment is performed in the following groups of patients:
1. What is an apical abscess?
2. What symptoms are characteristic of an apical abscess?
3. How is an apical abscess treated?
4. What complications can occur if left untreated?
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Siqueira, J. F., Jr, & Rôças, I. N. (2022). Treatment of endodontic infections. Quintessenz Verlag.
3.
Berman, L. H., & Hargreaves, K. M. (2020). Cohen’s Pathways of the Pulp Expert Consult. Elsevier.
https://www.aae.org/specialty/clinical-resources/guide-clinical-endodontics/
4.
Torabinejad, M., Fouad, A., & Shabahang, S. (2020). Endodontics: Principles and Practice. Elsevier.
5.
Ghom, A. G., & Ghom, A. S. (2019). Textbook of Oral Medicine: With Free Book on Basic Oral Radiology. Jaypee Brothers Medical Publishers Pvt. Ltd. Limited.
6.
American Association of Endodontists. (2019, June 3). Guide to Clinical Endodontics – American Association of Endodontists.
7.
Ricucci, D., & Siqueira, J. F. (2013). Endodontology: An Integrated Biological and Clinical View. Quintessence Publishing (IL).
8.
Bergenholtz, G., Hørsted-Bindslev, P., & Reit, C. (2013). Textbook of Endodontology. John Wiley & Sons.
9.
Hülsmann, M., Schäfer, E., Bargholz, C., & Barthel, C. (2009). Problems in endodontics: Etiology, Diagnosis and Treatment. Quintessence Publishing (IL).
10.
Beer, R., Baumann, M. A., & Kielbassa, A. M. (2004). Taschenatlas der Endodontie.




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io