Systemic Enamel Hypoplasia: Etiology, Classification, Clinical Presentation, and Treatment
Developmental Enamel Defects: Systemic Hypoplasia. Overview of the Etiology, Clinical Forms, Diagnosis, and Aesthetic Restoration Techniques for Teeth.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
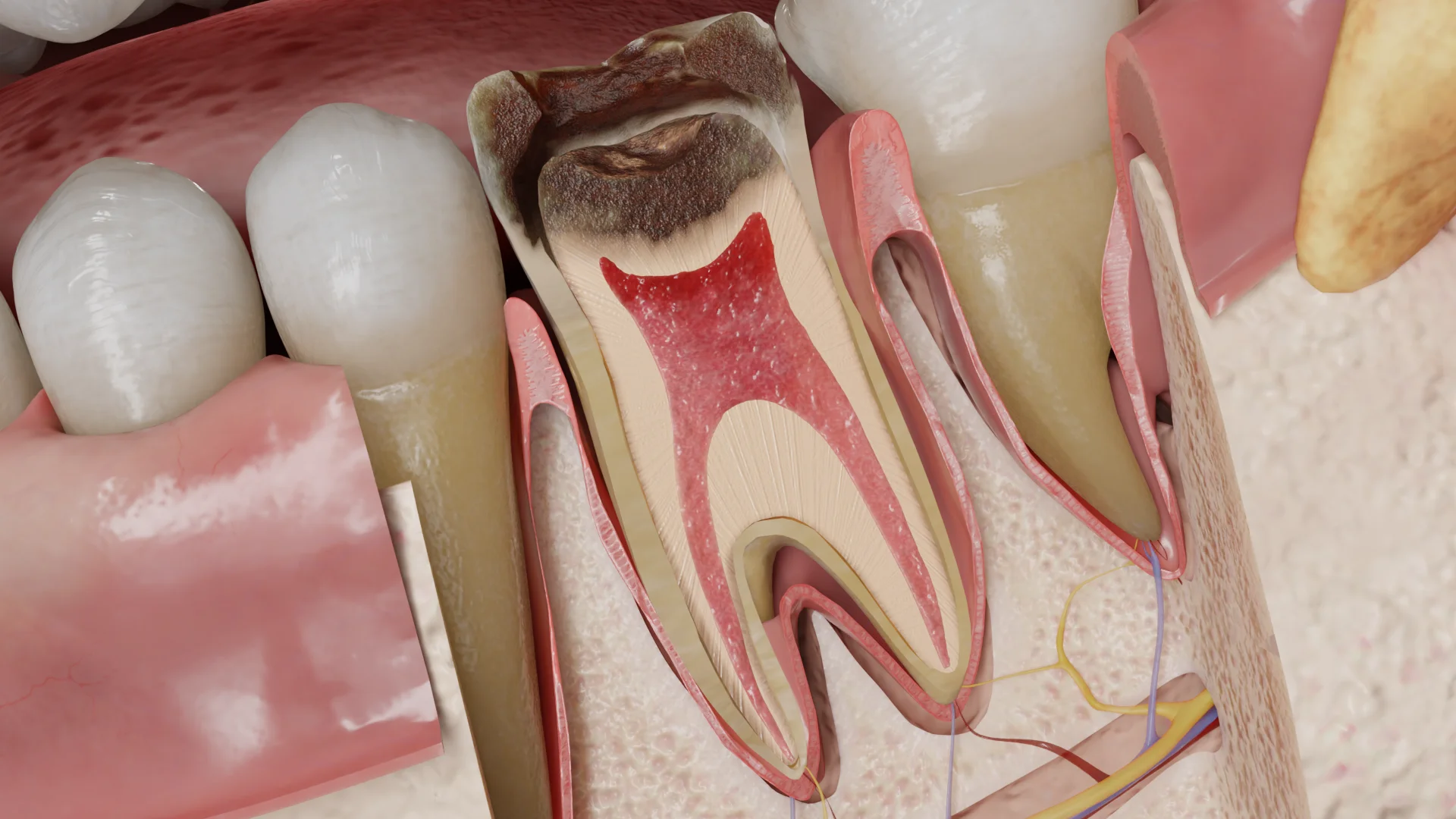
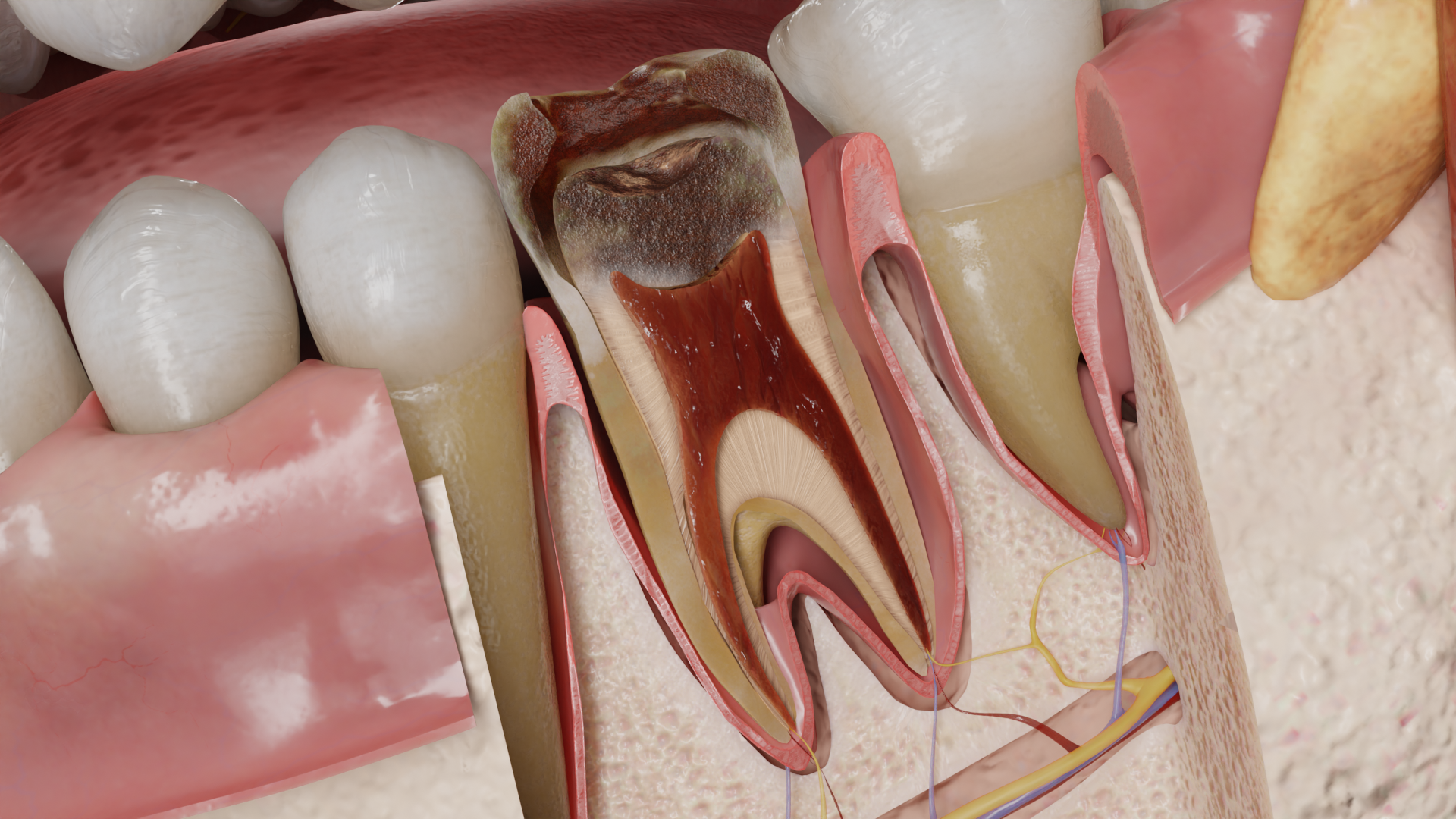
Acute apical periodontitis (AP) is an inflammation of the periodontium that is primarily caused by an infection of the root canal system. The inflammation usually affects the alveolar bone, also known as the alveolar process, the periodontal ligament, and the cementum surrounding the apex of the tooth root (the periapical region).

There are several possible reasons for AP:
In the majority of cases, AP is caused by bacterial infection. Within the root canal system, bacteria can exist as planktonic organisms. However, most often, they form biofilms, which are aggregates of microorganisms attached to the dentin. For one thing, this mode of existence provides bacteria with effective protection against microbial competitors and the host immune system; for another, it makes them more resistant to a variety of antibacterial agents.
Pathogens usually enter the periapical tissues through the apical foramen, lateral canals, or root perforations. The bacteria found in untreated root canals are typically of a mixed type with approximately equal amounts of gram-positive and gram-negative species, dominated by obligate anaerobes. Notably, evidence linking certain bacterial species to distinct AP symptoms is limited. The most common bacterial pathogens include Fusobacterium, Dialister, Porphyromonas, Prevotella, Tannerella, Treponema, Pyramidobacter, Veillonella, Campylobacter, Parvimonas, Filifactor, Pseudoramibacter, Streptococcus, Propionibacterium, Olsenella, Actinomyces, Peptostreptococcus, and Eubacterium.
Acute (symptomatic) AP is a common consequence of total pulp necrosis. Nevertheless, it can also develop against viable, though inflamed, pulp tissue in the apical portion of the root canal. This may happen due to an infection of the vital pulp, resulting in the diffusion of inflammatory mediators, proinflammatory cytokines, chemokines, and bacterial toxins into the periapical region prior to complete pulp necrosis.
The pathophysiology of acute AP resembles that of a typical acute inflammatory response, involving vasodilation, increased vascular permeability, and the migration of leukocytes from the bloodstream into the perivascular space. These reactions lead to leukocyte infiltration, accumulation of immunoglobulins and plasma proteins, and complement activation in the damaged tissue. In acute AP, the primary effector cells are polymorphonuclear neutrophils, which are known as the first line of defense against bacterial infection. Neutrophil death results in the release of lysosomal proteolytic enzymes, reactive oxygen species (such as nitric oxide), proinflammatory cytokines, eicosanoids, and matrix metalloproteinases, which further intensify the inflammatory response and contribute to tissue damage.
Although AP is predominantly an infectious disease, bacteria are typically found within the root canal system rather than in the periapical tissues.
Destruction of the apical bone is uncommon in AP. Since the condition is associated with a short-term acute inflammatory response, neutrophils and macrophages are not able to resorb bone tissue.
The possible outcomes of acute AP include:
– repair of periapical tissues (if the causative factor is eliminated by root canal treatment);
– abscess formation (in cases of extensive invasion of pyogenic bacteria);
– progression to chronic periapical inflammation (if the causative factor persists).

Depending on the underlying etiology, the following anatomical changes may be observed in the affected tooth:
The yellow-gray or gray-black pulp may be partially or completely necrotic. At the apex of the roots, the pulp may appear edematous, hyperemic, and bright red. The periodontal ligament space near the root apex is typically widened and filled with serous-hemorrhagic or purulent exudate.
Patients with acute AP often complain of prolonged, dull, localized pain that intensifies when biting on the affected tooth, along with a sensation that the tooth feels “raised” or higher than the adjacent teeth. There may also be a noticeable change in tooth color. Past medical history may include a prolonged response to thermal stimuli and/or spontaneous pain that has subsided over time.
Find more scientifically accurate content on our social media








The primary treatment for acute AP is endodontic therapy. This is when the necrotic pulp tissue is removed, followed by mechanical and chemical debridement of the root canals. If exudate is present in the canals, temporary intracanal dressings (calcium hydroxide paste) are recommended. Subsequently, the root canals are hermetically sealed, and the tooth is restored.
In cases where endodontic treatment may have unfavorable outcomes, tooth extraction is indicated.
For cases involving a premature contact of a restoration or mechanical trauma, occlusal adjustment through selective grinding may be performed, followed by regular monitoring.
1. What is acute apical periodontitis?
2. What are the main symptoms of acute apical periodontitis?
3. What is the treatment for acute apical periodontitis?
4. What complications may arise from untreated acute apical periodontitis?
List of Sources
1.
Berman, L. H., & Hargreaves, K. M. (2020). Cohen’s Pathways of the Pulp Expert Consult. Elsevier.
2.
Torabinejad, M., Fouad, A., & Shabahang, S. (2020). Endodontics: Principles and Practice. Elsevier.
3.
American Association of Endodontists. (2019, June 3). Guide to Clinical Endodontics – American Association of Endodontists.
https://www.aae.org/specialty/clinical-resources/guide-clinical-endodontics/
4.
Ricucci, D., & Siqueira, J. F. (2013). Endodontology: An Integrated Biological and Clinical View. Quintessence Publishing (IL).
5.
Bergenholtz, G., Hørsted-Bindslev, P., & Reit, C. (2013). Textbook of Endodontology. John Wiley & Sons.
6.
Hülsmann, M., Schäfer, E., Bargholz, C., & Barthel, C. (2009). Problems in endodontics: Etiology, Diagnosis and Treatment. Quintessence Publishing (IL).
7.
Beer, R., Baumann, M. A., & Kielbassa, A. M. (2004). Taschenatlas der Endodontie.
Loading test 6 questions




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io