




Acute Sinusitis (Acute Rhinosinusitis): Classification, Clinical Manifestations, Diagnosis, and Treatment
A detailed review of rhinosinusitis, including classification, symptoms, diagnostic approaches, and current treatment strategies.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
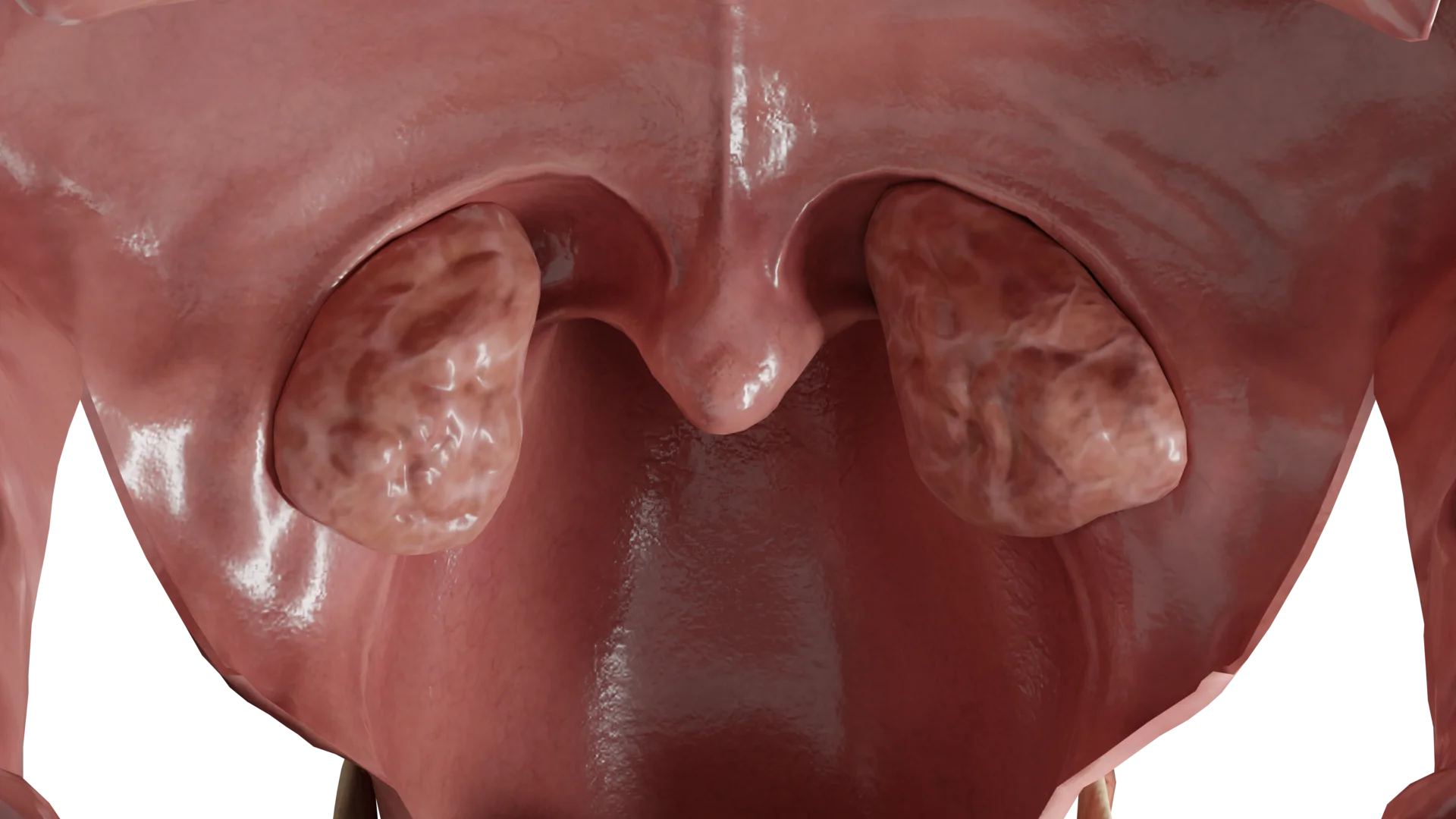
Hypertrophy of the palatine tonsils (HPT), also known as tonsillar hypertrophy, is an enlargement of the lymphatic tissue bundles located on each side of the oral cavity between the palatopharyngeal and the palatoglossal arches. This is a transient condition with no signs of chronic inflammation.
By tonsillar enlargement degree:
By localization:
Hypertrophy of palatine tonsils is one of the most common conditions in preschool and school-age children (about 25 per 1000 children). It can be combined with hypertrophy of the nasopharyngeal tonsil (adenoids), or occur independently. This disease occurs equally in males and females, with the highest peak in children aged 3 years to adolescence, followed by involution of lymphoid tissue (immunity has formed). However, hypertrophy can sometimes persist throughout life.
Tonsillar hypertrophy can have multiple etiologies, including adaptation problems and endocrine disorders (i.e., adrenal insufficiency). In addition, allergy conditions, such as lymphatic-hypoplastic diathesis, may be the cause. It should be noted that the palatine tonsils can become enlarged in response to external irritants. These may include postnasal drip, constant mouth breathing, or difficulty in nasal breathing due to inflammation of the pharyngeal tonsil. Another significant reason for HPT that has drawn a lot of attention lately is gastroesophageal reflux (GER) and the irritating effects of hydrochloric acid.
The tonsils are an important part of the immune system. Their major function is to support the local mucosal immune system of the upper respiratory tract. Foreign antigens (viruses, bacteria, etc.) initiate an acquired immune response in the tonsils, leading to transient tonsillar hypertrophy. When exposed to a new antigen, the tonsils produce specific immunoglobulins A (IgA) and G (IgG), which constitute the primary immune response. If a patient encounters the same pathogen later on, existing immunoglobulins enable the production of T lymphocytes in the lymphoid tissue. As a result, a more rapid and effective secondary immune response is generated. However, due to the immaturity of the immune system, T lymphocytes are produced excessively to compensate for their functional insufficiency. This leads to an active proliferation of the tonsillar lymphoid tissue, manifested in hypertrophy.
The degree of HPT is classified according to B.S. Preobrazhensky. The classification is based on the tonsil localization relative to the fauces:
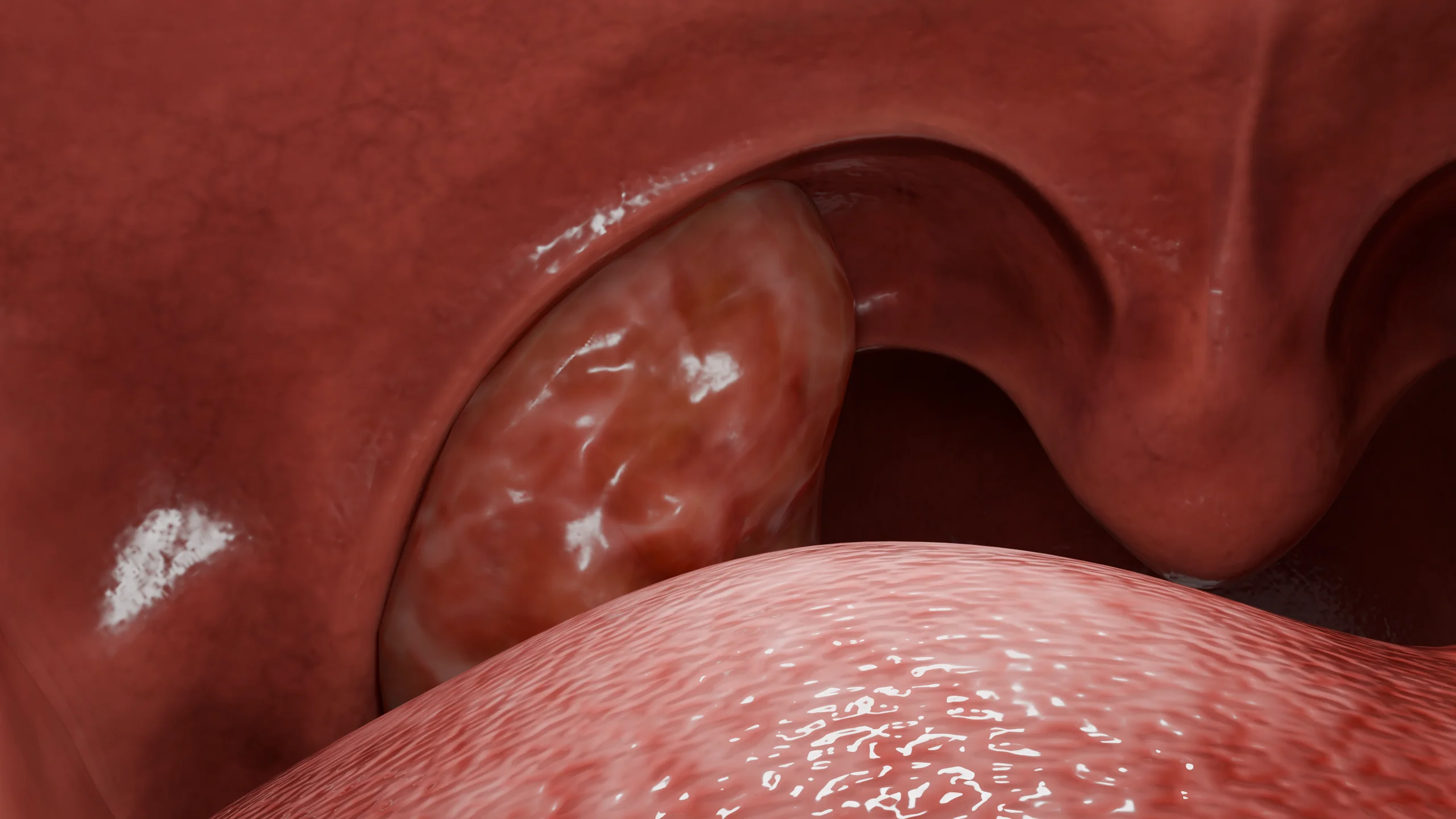
HPT can be asymmetrical. Typically, enlarged tonsils have a pale pink color and a glossy surface. The altered tonsil tissue is heterogeneous and can be loose and lumpy. Twisted tonsillar crypts can occasionally be observed.
Therefore, tonsil fusion to the palatine arches, cicatricial changes, or inflammation-induced occlusion of the tonsillar crypts are not common. On palpation, hypertrophied tonsils should come loose from the tonsillar bed easily.
In HPT, histopathological evaluation shows that hyperplastic lymphoid tissue prevails, follicular areas are increased, and plasma cells and macrophages are absent.
The enlargement of pharyngeal and palatine tonsils can be asymptomatic or accompanied by certain patient complaints (in hypertrophy of grades 2-3). In most cases, the only problem that prompts parents to seek medical help is their child’s snoring. Parents typically note that snoring is constant and does not depend on sleeping position. Frequent nighttime awakenings are also common, leading to fatigue and poor concentration during the day. If combined with adenoid hypertrophy, HPT may trigger sleep apnea (lapses in breathing during sleep). Severe HPT is characterized by trouble swallowing and a feeling of a lump in the throat, which causes significant discomfort for the patient. Tonsillar hypertrophy can also significantly affect a child’s speech, resulting in nasal or slurred speech and dysphonia. Moreover, the pharyngeal opening of the auditory tube may become blocked if an individual presents with a high superior pole of the tonsils complicated by a severe HPT. This results in middle ear congestion and otitis media with effusion, which deteriorate the hearing function.
Oropharyngoscopy and medical history are sufficient to diagnose HPT; laboratory testing is not required.
It is essential to come up with a differential diagnosis, which includes chronic tonsillitis, hematopoietic disorders (leukemia), and neoplasms of the palatine tonsils, especially in the case of unilateral hypertrophy.
Find more scientifically accurate content on our social media








The main treatment for HPT is surgical (if indicated). In preschool children, a tonsillotomy (also known as partial tonsillectomy) is typically performed. This procedure means that only hypertrophied areas of the tonsils are to be excised. Another type of surgery for HPT is tonsillectomy, when all tonsillar tissue within the tonsillar bed is removed, including the capsule. It is more often used in older age groups. In cases of concomitant adenoid hypertrophy that requires treatment, the main type of surgery can be performed alongside adenotomy when the pharyngeal tonsil is excised. The primary indications for surgical treatment are apnea, recurrent otitis media with effusion, and severe speech impairment. The procedures given above are elective inpatient surgeries performed under general anesthesia. It is also important to ensure that there are no contraindications, such as coagulation disorders or acute inflammatory processes.
Conservative treatments have been found to be ineffective. Occasionally, homeopathic products, herbal remedies, and physiotherapy may be considered. However, there is currently no scientific evidence to support the efficacy of these therapeutic approaches.
1. What are the indications for surgical treatment of hypertrophy of the palatine tonsils?
2. What are the possible complications of hypertrophy of the palatine tonsils?
3. Why is hypertrophy of the palatine tonsils more common in children?
4. Can hypertrophy of the palatine tonsils persist into adulthood?
5. Are there preventive measures for hypertrophy of the palatine tonsils?
References
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Total Otolaryngology—Head and Neck Surgery, Anthony P. Sclafani, Robin A. Dyleski, Michael J. Pitman, Stimson P. Schantz. Thieme Medical Publishers, Inc., 2015. ISBN 978-1-60406-646-3.
3.
Бербом Х. Болезни уха, горла и носа / Ханс Бербом, Оливер Кашке, Тадеус Навка, Эндрю Свифт; пер. с англ. – 2-е изд. – М. : МЕДпреcс-информ, 2016. – 776 с. : ил. ISBN 978-5-00030- 322-1.
4.
Densert O, Desai H, Eliasson A, Frederiksen L, Andersson D, Olaison J, Widmark C. Tonsillotomy in children with tonsillar hypertrophy. Acta Otolaryngol. 2001 Oct;121(7):854-8. doi: 10.1080/00016480152602339. PMID: 11718252.
5.
Reis LG, Almeida EC, da Silva JC, Pereira Gde A, Barbosa Vde F, Etchebehere RM. Tonsillar hyperplasia and recurrent tonsillitis: clinical-histological correlation. Braz J Otorhinolaryngol. 2013 Sep-Oct;79(5):603-8. doi: 10.5935/1808-8694.20130108. PMID: 24141676; PMCID: PMC9442398.
Loading test 6 questions




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io




