




Chalazion: Etiology, Pathogenesis, Diagnosis and Treatment Methods
A Detailed Analysis of Chalazia of the Eyelid. Explore the Etiology, Pathogenesis, Clinical Presentation, Differential Diagnosis and Modern Treatment Protocols.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
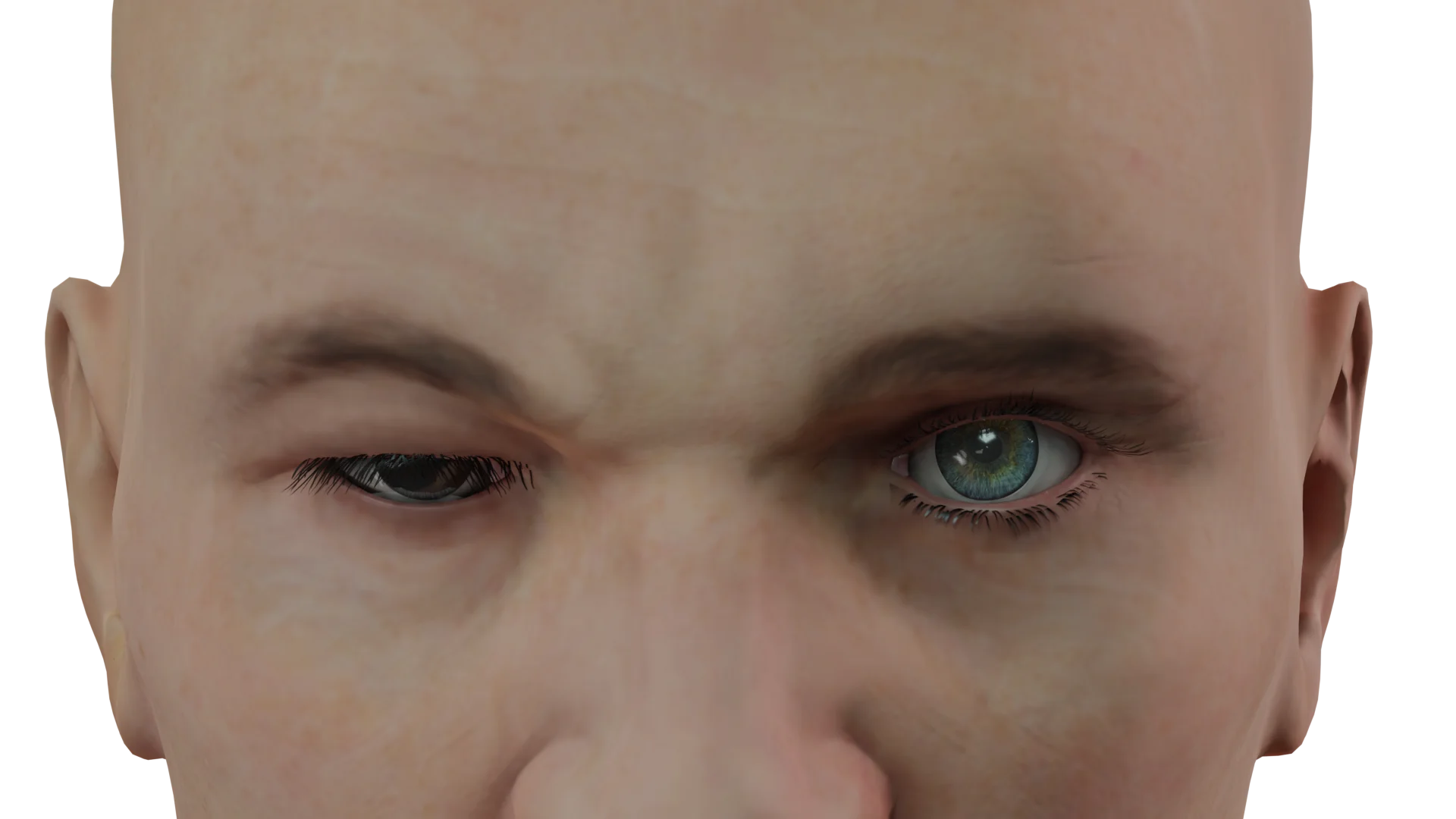
Ptosis, or blepharoptosis, is a pathological condition in which the upper eyelid droops below its normal anatomical position while in the primary gaze position.
The term originates from the Greek words blepharon (eyelid) and ptōsis (an act of descent).
Blepharoptosis may be categorized in various ways concerning its pathogenetic, diagnostic, predictive, and therapeutic aspects.
Etiologically, upper eyelid ptosis may be classified into:
The condition typically presents as nonprogressive drooping of the upper eyelid. Unilateral ptosis accounts for 75 % of cases, while the bilateral form is asymmetrical.
Histopathological examination of isolated congenital myogenic ptosis reveals dysgenesis of the anterior part of the levator palpebrae superioris. Over time, the striated muscle fibers are lost, and loose connective tissue overgrows, impairing the levator’s ability to contract and relax.
This form of ptosis may arise due to various reasons, as outlined below.
Myogenic etiology: This category encompasses primary inherited myopathies accompanied by a chronic, progressive decline in the function of the levator palpebrae superiori, as well as secondary myopathies associated with other systemic conditions.
Primary hereditary myopathies include mitochondrial disorders and autosomal dominant or recessive inherited conditions.
Chronic progressive external ophthalmoplegia is the most common form of primary inherited myopathy. By the age of 30–40 years, such patients typically present with bilateral ptosis and ophthalmoplegia, which may be accompanied by neurosensory deafness and dysphagia.
Oculopharyngeal muscular dystrophy is a rare form of muscular dystrophy with an onset at 40–50 years of age. It is typically characterized by progressive ptosis and external ophthalmoplegia. This pathology is diagnosed through the identification of an autosomal dominant PABPN1 mutation in combination with systemic dysphagia and weakness in proximal extremities.
Clinically, blepharoptosis may be classified based on its severity:
3D model of ptosis of upper eyelid of various severity:
 Ptosis — first stage
Ptosis — first stage Ptosis — second stagePtosis — third stage
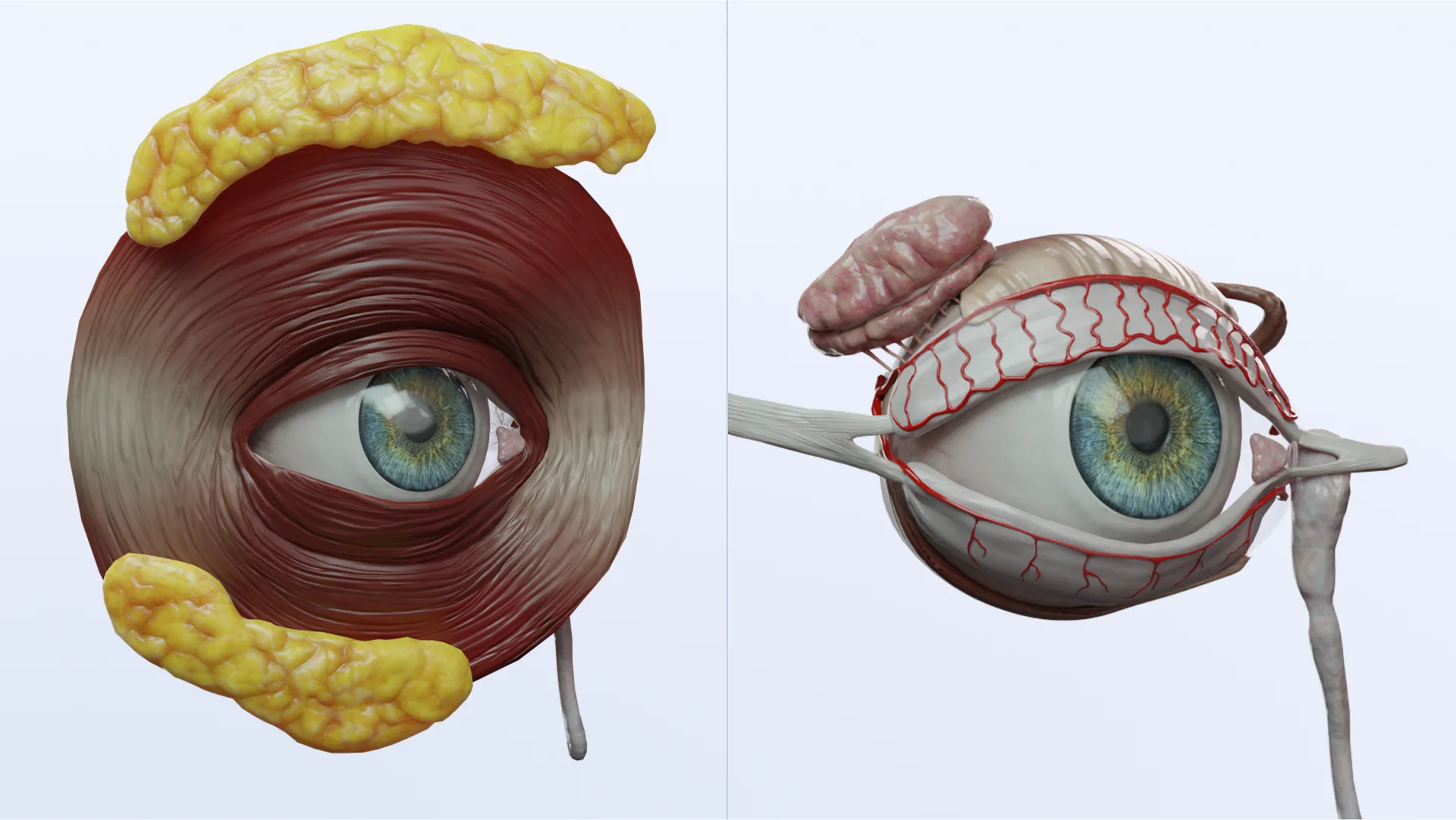
Ptosis — second stagePtosis — third stageElevation of the upper eyelid is a complex process involving three different retractors, each innervated individually. Any direct or indirect impact on these muscles may trigger blepharoptosis.
The levator palpebrae superioris (upper eyelid levator) serves as an antagonist to the orbicularis oculi muscle. It originates from the lesser wing of the sphenoid bone and gives off the superior rectus muscle (inferiorly) and the obliquus superior capitis muscle (medially). At the level of the supraorbital margin, the levator palpebrae superioris transitions into a broad tendon that divides into anterior, middle, and posterior portions.
The anterior and posterior portions receive innervation from the superior branch of the oculomotor nerve, while the middle portion is innervated by the sympathetic fibers of the cervical sympathetic ganglion. The middle portion of the levator palpebrae superioris has been identified by some authors as an independent smooth muscle structure, referred to as the superior tarsal muscle or Müller’s muscle. It servesas a vertical mobility effector for the upper eyelid and works in conjunction with the levator palpebrae superioris.
The core of each eyelid is formed by a dense tarsal plate composed of fibrous connective tissue. For the upper eyelid, this plate typically measures 29–30 mm in length, 1 mm in thickness, and 10–12 mm in height.
The medial and lateral palpebral ligaments originate from the terminal portions of the upper and lower tarsal plates at their medial and lateral ends.
Blepharoptosis should be managed based on its etiology, severity, and associated symptoms.
Certain forms of blepharoptosis may require medical therapy. Eye disorders linked to thyroid gland conditions may trigger drooping of the upper eyelid. Such cases necessitate corticosteroids and/or immunomodulator therapy to stabilize the eyelid for approximately 6–9 months prior to surgery.
As the levator function may vary greatly in myastenia patients, the dose of cholinesterase inhibitors and/or corticosteroids should be adjusted to stabilize the condition for 3–4 years before any corrective procedure.
Botulotoxin injected into the pretarsal area of the orbicularis oculi muscle may be effective to treat mild acquired aponeurotic ptosis or acquired neurogenic ptosis.
Find more scientifically accurate content on our social media








Blepharoptosis may be corrected using several approaches:
Currently, suspension techniques are preferred when the levator function is weak, whereas average or strong muscular performance may only require levator resection.
Suspension techniques involve elevating the upper eyelid using the frontalis muscle or superior rectus muscle. This method of ptosis correction offers different variations and utilizes different kinds of sutures and autogenous tissues (muscles, sclera, dura, fascia lata, etc.). However, autogenous tissues generally yield insufficient results and increase the risk of relapse. That is why they are now rarely used in blepharosplasty. The fascia lata is the only exception to this trend.
Resection of the levator palpebrae superioris is another nosotropic approach to treating blepharoptosis. This surgical procedure anatomically restores the normal position of the upper eyelid. Severe blepharoptosis may require maximal levator resection. In such cases, the lateral horns of the aponeurosis and the Whitnall ligament are completely dissected.
Procedures aimed at reinforcing the levator palpebrae superioris may be further categorized into transcutaneous and transconjuctival levator resections. These techniques result in the formation of a fold, which shortens the tendon of the levator.
1. Can a newborn have ptosis?
2. Does a child with congenital ptosis need surgery?
3. What causes acquired ptosis?
4. Can ptosis heal on its own?
5. Is ptosis dangerous?
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Ptosis. Merriam-Webster Medical Dictionary.
Available from: https://www.merriam-webster.com/dictionary/ptosis. [Last accessed on 27 Nov 2020].
3.
Belphar-. Merriam-Webster Medical Dictionary.
Available from: https://www.merriam-webster.com/dictionary/blephar-. [Last accessed on 27 Nov 2020]
4.
Nalci Baytaroğlu H, Kaya B, Korkusuz P, Hoşal MB. A study of histopathologic evaluation and clinical correlation for isolated congenital myogenic ptosis and aponeurotic ptosis. Ophthalmic Plast Reconstr Surg 2020;36:380-4.
5.
Bacharach J., Lee, W.W., Harrison, A.R. et al. A review of acquired blepharoptosis: prevalence, diagnosis, and current treatment options // Eye. – 2021. – Vol. 35. – P. 2468–2481.
https://doi.org/10.1038/s41433-021-01547-5.
6.
Göncü T., Çakmak S., Akal A., Karaismailoğlu E. Improvement in Levator Function After Anterior Levator Resection for the Treatment of Congenital Ptosis // Ophthalmic Plastic and Reconstructive Surgery. – 2014. – Vol. 31(3). DOI: 10.1097/IOP.0000000000000242.
7.
Li, Z. et al. Artificial intelligence in ophthalmology: The path to the real-world clinic. Cell Rep. Med. 4, 101095 (2023). DOI: 10.1016/j.xcrm.2023.101095
8.
Hung, J. Y. et al. A deep learning approach to identify blepharoptosis by convolutional neural networks. Int. J. Med. Inform. 148, 104402 (2021).
https://doi.org/10.3390/jpm12020283
Loading test 6 questions




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io
.webp)