Breast Fibroadenoma: Etiology, Clinical Presentation, Diagnosis and Treatment
Svetlana D.Surgical oncologist, MD
14 min read·October 15, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Fibroadenoma is a benign breast neoplasm consisting of connective and glandular tissue. It is one of the most common focal pathologies of the breast. It can occur at any age but is most commonly diagnosed between the ages of 14 and 35.
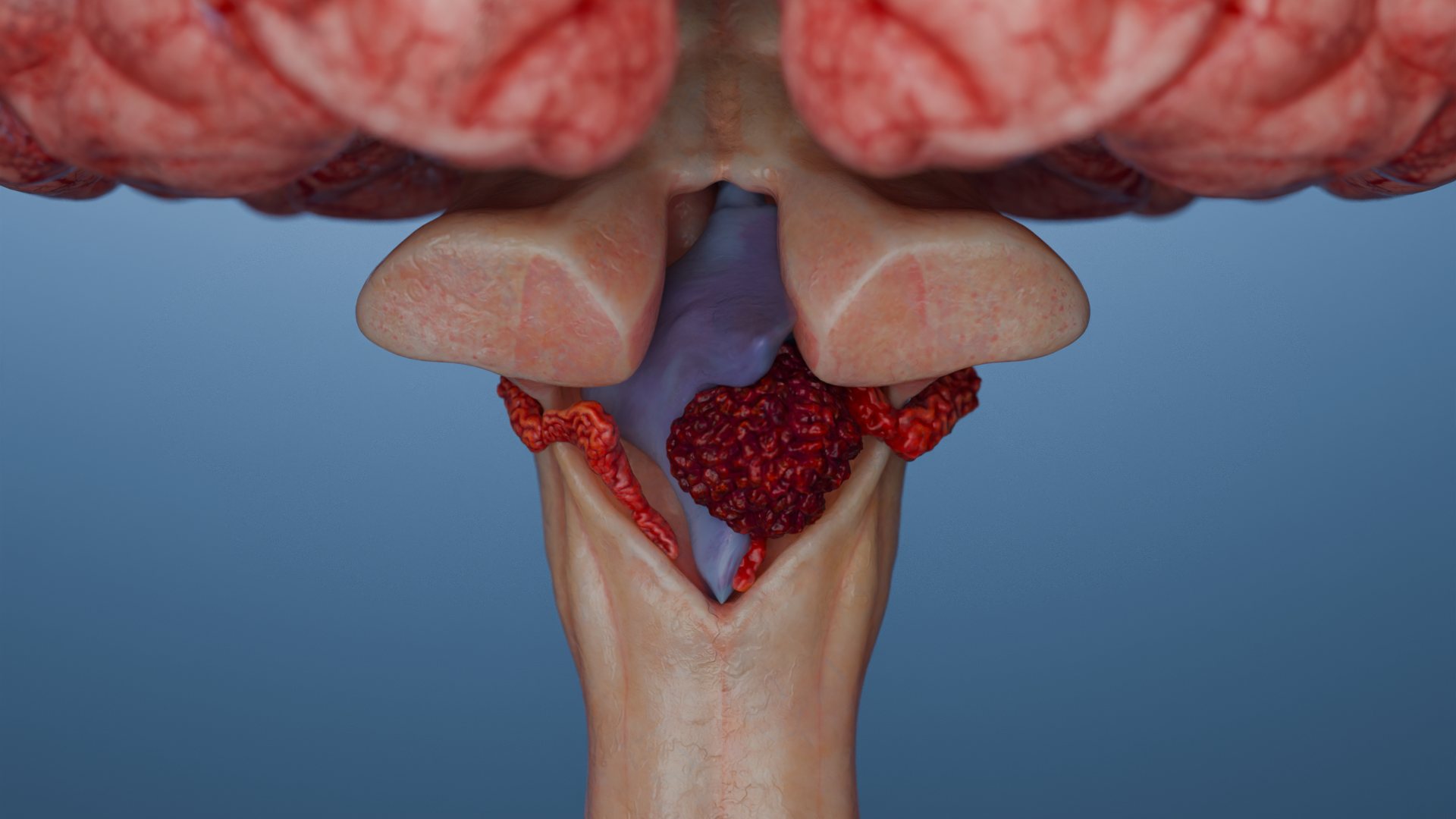
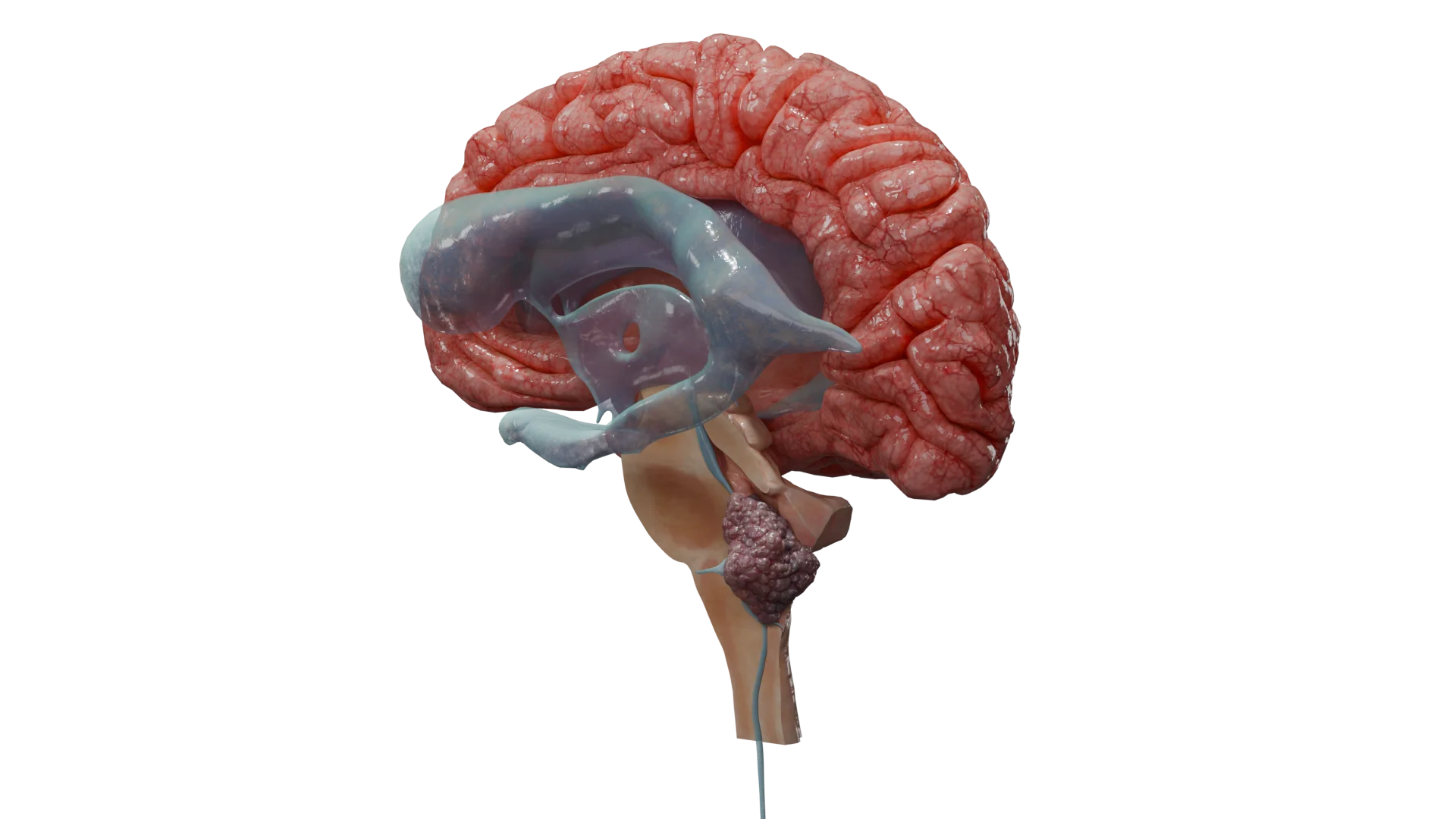
Fibroadenoma: 3D modelPhyllodes fibroadenoma (benign phyllodes tumour): 3D model3D animation: fibroadenoma
Etiology and pathogenesis of fibroadenoma
The causes of fibroadenomas are not fully understood. It is currently believed that the main factor in the development of fibroadenoma (FA) is hormonal imbalance: an increase in oestrogen levels associated with decreased progesterone levels stimulates hyperplasia of glandular and connective tissue, which is a key factor in the development of fibroadenoma.
Increased sensitivity of breast tissue to estrogen may also contribute to the development of hyperplasia even at normal levels of sex hormones.
In addition to hormonal imbalance, somatic mutations in the MED12 (found in more than 60%), KMT2D and RARA genes play a role in the development of fibroadenomas.
Morphological presentation
Fibroadenoma is a clearly defined, non-encapsulated mass characterized by expansive growth. A proliferation of connective and glandular tissue cells, with a relatively constant ratio between them within the mass volume, is typical for these tumors.
The stroma is homogeneous and hypovascular, consisting of spindle-shaped cells with indistinct oval or elongated nuclei. There is no stromal cell polymorphism. Mitoses are rare, more typical for juvenile fibroadenomas, and do not indicate malignancy. In older women, the stroma may be hyalinized.
The parenchyma of fibroadenoma is represented by normal double-layered epithelium typical of mammary ducts: the inner layer is represented by cubic epithelium, while the outer layer consists of myoepithelial cells.
Classification of breast fibroadenomas
By growth type
Depending on the type of growth, the histological variants of fibroadenomas are as follows:
Pericanalicular: characterized by the growth of connective tissue around the mammary ducts while maintaining their patency;
Intracanalicular: connective tissue growth occurs inside the duct, leading to its deformation and narrowing of the lumen up to complete occlusion;
Mixed fibroadenoma: connective tissue growth occurs both around and inside the ducts.
Depending on the growth rate and degree of maturity, fibroadenomas are divided into mature and immature.
By histological structure
Depending on the histological structure, there are:
Typical adult-type fibroadenomas;
Juvenile fibroadenomas: occur during puberty, characterized by more pronounced epithelial hyperplasia and a higher number of stromal cells;
Myxoid fibroadenomas: characterized by the presence of evident myxoid stroma;
Phyllodes (leaf-shaped) fibroadenomas: arise from the glandular tissue of the breast, are characterized by rapid growth and the possibility of malignancy.
Depending on their structure, fibroadenomas are classified as simple, consisting of homogeneous cells, and complex, which may contain cystic cavities and calcified foci.
Juvenile fibroadenoma. Source: WebPathology [11]Myxoid fibroadenoma. Author: M. Khan, DO. Source: NCBI [8]
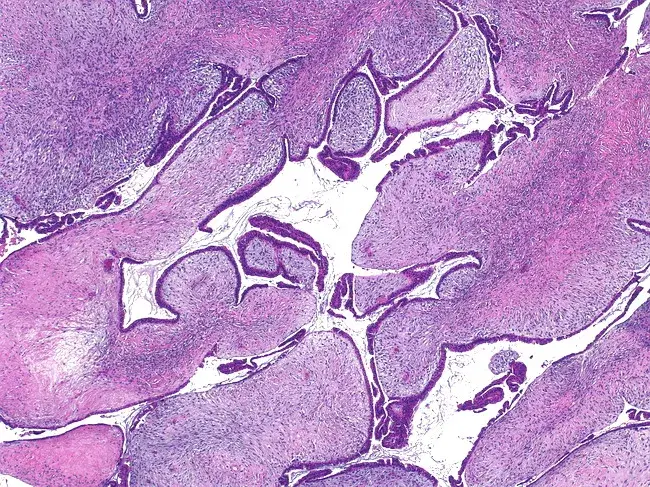
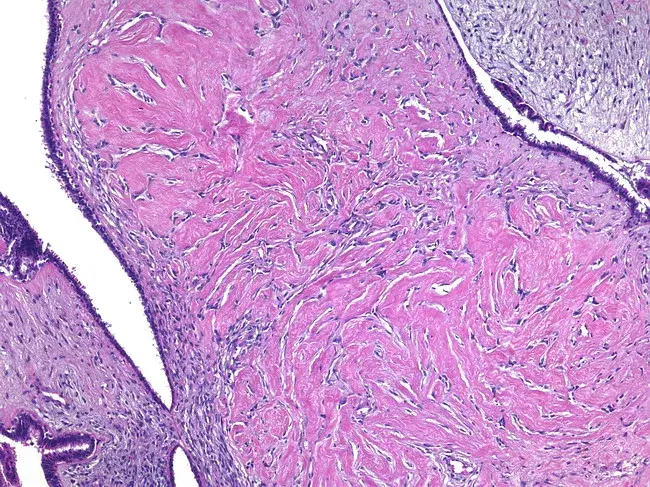
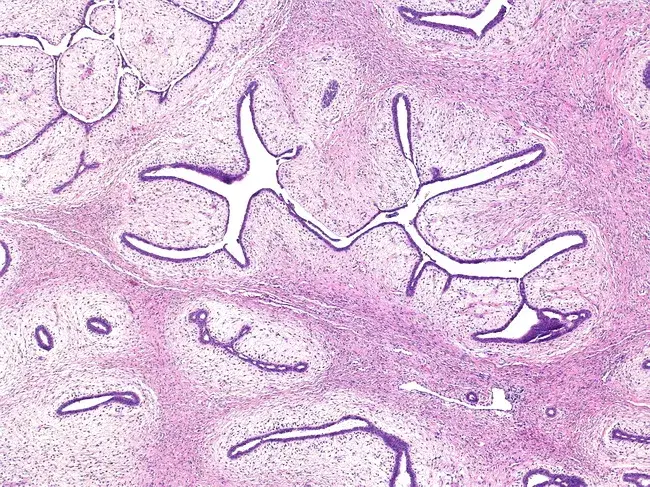
Below are histological images of low-grade phyllodes tumors (fibroadenomas) having various manifestations and histological changes. Source: WebPathology [11]:
Phyllodes tumor: structure of the stroma and glandular epithelium
Low-grade phyllodes tumor with expansion of slit-like spaces and formation of cysts with papillary structures
Histological features of low-grade phyllodes tumor with pseudoangiomatous stromal hyperplasia (PASH)-type stromal changes
Phyllodes tumor with periductal stromal proliferation and nodular structure
Clinical presentation
The clinical presentation is non-specific and depends on the size of the lesion. Small fibroadenomas (less than 5 mm) are usually asymptomatic and are detected by ultrasound.
Clinically, fibroadenoma manifests as a clearly defined, round mass in the breast with the following characteristics:
Smooth, even contours;
Painless on palpation;
Easy to move under the skin;
Dense elastic consistency.
Phyllodes fibroadenomas can reach enormous sizes, significantly enlarging and deforming the contour of the breast.
During pregnancy and lactation, fibroadenomas can rapidly increase in size and compress the lactiferous ducts until they are completely blocked, leading to lactostasis and, as a result, lactational mastitis.
Diagnosis of breast fibroadenoma
The findings of visual inspection and palpation in fibroadenoma are non-specific, i.e. they can be very similar to the manifestations of other lesions, including cysts. This is why instrumental methods are always required for accurate diagnosis.
1. Visual inspection
There are usually no visual changes when the fibroadenoma is small. Large masses may cause visible deformity of the breast contour.
2. Palpation
On physical examination, a fibroadenoma is most often identified as a mass with the following characteristics:
Shape and contours: clearly demarcated, round or oval, with smooth surface;
Consistency: densely elastic, “rubber-like”.
Painfulness: painless;
Mobility: very easily displaced in the glandular tissue, so it is informally called “mammary mouse,” or “breast mouse.”
Regional lymph nodes (axillary, supra- and subclavian) in fibroadenoma are usually not enlarged.
3. Ultrasound
The typical ultrasound signs of fibroadenoma are as follows:
Solid mass, frequently having homogeneous structure;
Iso- or hypoechoic with clear contours and smooth or lobulated borders (depends on the morphological type);
Horizontal orientation;
Movable when compressed by the US probe;
Occasionally, dorsal pseudo-amplification of the signal may occur;
Hypo- or avascular while mapping in CDI (color Doppler imaging) and PD (power Doppler) modes;
Strain-ratio index at elastometry is above 2.5.
Breast fibroadenoma on ultrasound image. Author: Dr. Taco Geertsma. Source: UltrasoundCases [12]
Ultrasound signs of a phyllodes fibroadenoma:
An iso- or hypoechoic mass;
Heterogeneous structure, with non-echoic inclusions in the event of large mass size;
Rounded or oval in shape, with clear, even contours;
Presence of acoustic effects (symmetrical lateral shadows, dorsal signal amplification);
Significant intranodular vascularisation in CDI and PD modes;
Strain-ratio index at elastometry is above 2.5.
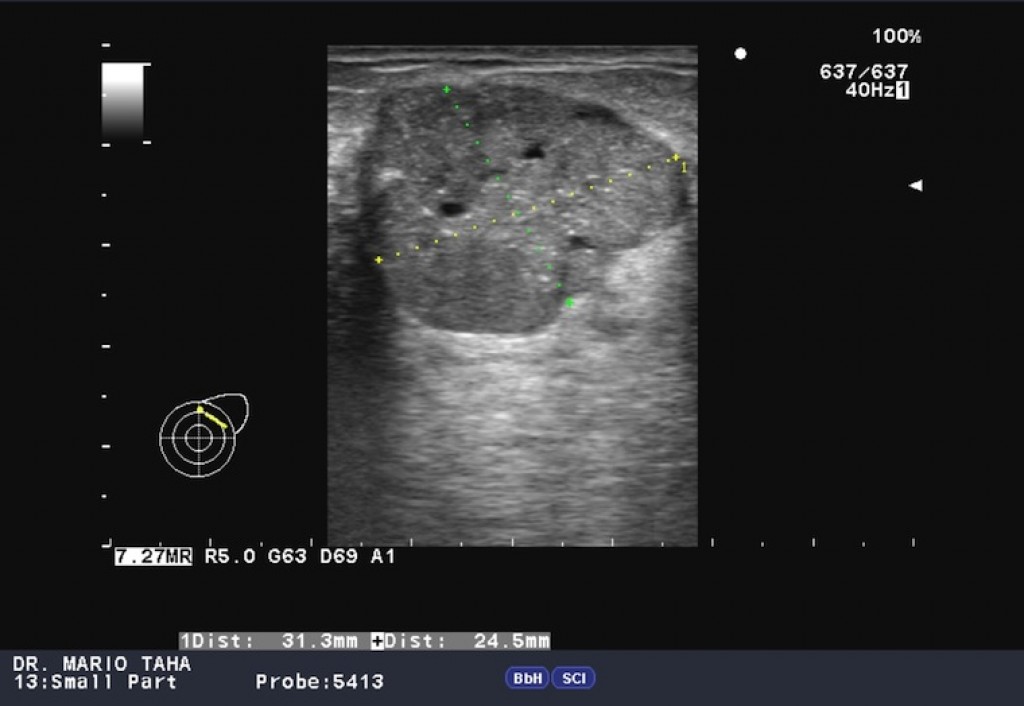
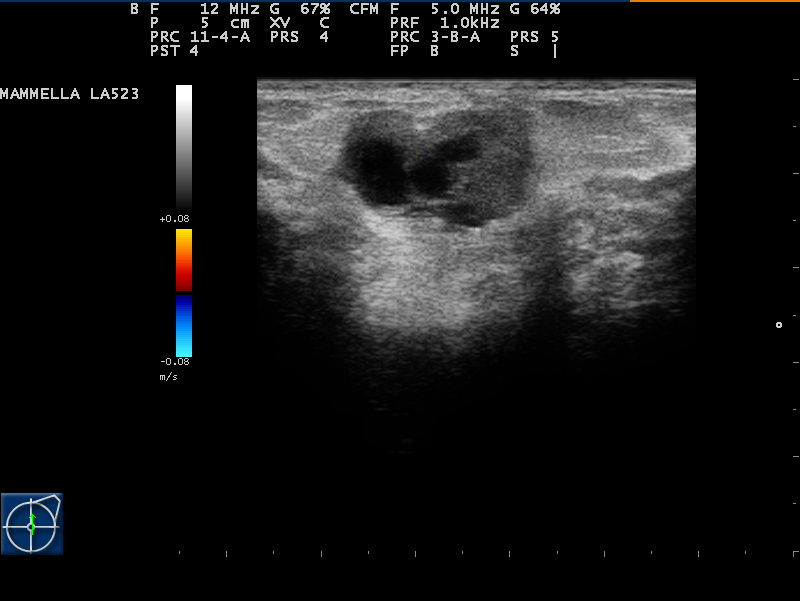
A phyllodes breast tumor is shown below on ultrasound images. Author of photos No. 1 and No. 2: Mario Taha. Source: Radiopaedia [10]. Author of photo No. 3: Giorgio M. Baratelli. Source: Radiopaedia [10].
Phyllodes breast tumor on ultrasound image No. 1
Phyllodes breast tumor on ultrasound image No. 2
Phyllodes breast tumor on ultrasound image No. 3
Breast fibroadenomas, according to the BI-RADS classification, correspond to BI-RADS 3 (probably benign mass, risk of malignization less than 2%) and BI-RADS 4 (risk of malignization 2–95%). In the presence of ultrasound criteria consistent with BI-RADS 4, the patient is indicated for tumor biopsy to clarify the diagnosis.
4. Mammography
Mammography in the diagnosis of fibroadenomas has limited utility due to the fact that this pathology, as a rule, occurs in patients of reproductive age, and well-developed glandular tissue worsens the visualization of masses.
Depending on the histological type, the tumor on radiographs can be defined as a homogeneous round, oval-shaped mass with a clear contour (pericanalicular fibroadenomas), or have a lobular, heterogeneous structure with unclear contours (intracanalicular fibroadenoma). Large, popcorn-shaped calcified foci may be present, and calcification of the entire mass is also possible.
Breast fibroadenomas on mammograms. Author: Hani M. Al Salam. Source: Radiopaedia [10]
5. Magnetic resonance imaging (MRI)
Magnetic resonance imaging in fibroadenomas is not the method of choice and is clarifying in nature. Fibroadenoma on CT scans is visualized as a round or oval mass with clear contours.
It is iso- or hypointense on T1-weighted images, and can be either hypo- or hyperintense on T2-weighted images. Contrast study findings are characterized by a slow initial enhancement followed by a persistent delayed phase (type I enhancement curve).
MRI of breast fibroadenoma. Author: Roberto Schubert. Source: Radiopaedia [10]
Morphological verification is performed by fine-needle aspiration biopsy (cytological verification of the diagnosis), core needle biopsy, excisional biopsy.
6. Fine-needle aspiration biopsy (FAB)
It is a diagnostic procedure that is performed to obtain cellular material from a mass for subsequent cytological examination.
Advantages: the procedure requires no special preparation, is performed in outpatient settings and, as a rule, does not require anesthesia.
Disadvantage: only allows evaluation of individual cells, not tissue structure, so is not always adequate for definitive diagnosis.
This is the “gold standard” in the diagnosis of fibroadenomas. The procedure aims to take columns of tissue for subsequent histological examination, which allows you to study not only the cells but also the structure of the tissue.
Advantages: gives the most accurate and complete diagnosis, allowing to distinguish fibroadenoma from other tumors, including malignant ones.
Procedure: unlike FAB, core needle biopsy requires local anesthesia. Under ultrasound control, several tissue samples are taken with a special instrument (core needle, or trephine).
Complications: similar to FAB but slightly more common. Allergic reactions to the anesthetic may occur.
8. Excisional biopsy
This is surgical removal of the entire mass followed by histological examination. For fibroadenoma, this procedure is both diagnostic and therapeutic.
Indications: it is used for large or rapidly growing fibroadenomas, in the presence of atypical features, and at the patient’s request.
Procedure: performed in inpatient or outpatient settings under local or general anesthesia.
Complications:
Bleeding from the postoperative wound;
Inflammation of the postoperative wound;
Allergic reactions to anesthetics.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Breast fibroadenoma treatment
In most cases, fibroadenomas do not require treatment and patients with this diagnosis are only subject to dynamic monitoring.
There is no medication therapy approved.
Surgical treatment consists of removing the fibroadenoma within healthy tissue, for which a sectoral resection of breast, or lumpectomy, is performed.
Indications for surgical treatment are:
The size of the fibroadenoma is over 2 cm;
Presence of breast deformity;
Rapid tumor growth (enlargement twice or more in 3–6 months);
Phyllodes fibroadenoma (due to high risk of malignization);
Planning pregnancy (due to the high risk of rapid growth of fibroadenoma and, as a consequence, lactation disorders).
FAQ
1. What are the causes of fibroadenoma?
The main cause is considered to be hormonal imbalance, in particular, an increase in estrogen levels associated with progesterone deficiency, which stimulates the growth of breast tissue. In addition, somatic mutations in some genes (e.g., MED12) play an important role and are found in more than 60% of cases.
2. What are the signs and symptoms of fibroadenoma and does it hurt?
The main sign is the presence in the breast of a clearly delineated, rounded, densely elastic mass with smooth contours. On palpation, it is easily displaced (“slips”) and is usually completely painless. Smaller fibroadenomas may be asymptomatic and can only be detected on ultrasound.
3. Can a fibroadenoma progress to cancer and what are its main dangers?
A typical fibroadenoma is a benign tumor and does not progress to cancer. The main danger is associated with its rare histological subtype, the phyllodes (leaf-like) tumor. This variant is characterized by rapid growth and has the potential for malignant transformation (malignization), so it is always subject to surgical removal.
4. How fast does a fibroadenoma grow?
The rate of growth is individualized. Many fibroadenomas remain stable in size for years. However, a sign that requires attention is rapid growth, which is clinically defined as tumor enlargement of 2 or more times in 3–6 months. Such growth is one of the indications for surgical treatment. Also, fibroadenomas can rapidly increase during pregnancy.
5. Can a fibroadenoma disappear or resolve on its own?
No, unlike cysts, a fibroadenoma is a solid (tissue) tumor and cannot resolve on its own. As well, there is no medication therapy approved. Mentions that fibroadenoma can resolve during pregnancy are misleading; on the contrary, pregnancy is more likely to stimulate its growth.
6. How is a fibroadenoma removed, and when is it necessary?
Fibroadenoma removal is done surgically. The standard surgery is sectoral resection of the breast (or lumpectomy): excision of the tumor within healthy tissue. Indications for surgery: size more than 2 cm, rapid growth, deformation of the breast contour, phyllodes type of tumor, as well as planning pregnancy.
References
1.
VOKA Catalog. [Electronic resource].
https://catalog.voka.io/
2.
Article “Breast Description and Diagnosis.” UpToDate. [Electronic resource].
Medison Medical Journal, article “BI-RADS system for ultrasound: description, classification, illustrations (Система BI-RADS для УЗИ: описание, классификация, иллюстрации).” \[Article in Russian] Author: A. V. Anisimov (А. В. Анисимов). [Electronic resource].
https://www.medison.ru/si/art434.htm
4.
A. N. Sencha. Breast ultrasound. Step by step. From simple to complex. (А. Н. Сенча. Ультразвуковое исследование молочных желез. Шаг за шагом. От простого к сложному.) \[Book in Russian] 2nd edition.
5.
A. N. Sencha, Yu. V. Bikeev. Ultrasound examination of mammary glands. Atlas.
6.
S. K. Ternovoy, A. B. Abduraimov. Radiation mammology. (С. К. Терновой, А. Б. Абдураимов. Лучевая маммология.) \[Book in Russian]
7.
Pathology Outlines. [Electronic resource].
https://www.pathologyoutlines.com
8.
Ajmal M., Khan M., Van Fossen K. Breast Fibroadenoma. [Electronic resource].
https://www.ncbi.nlm.nih.gov/books/NBK535345/
9.
Leithner D., Wengert G.J., Helbich T.H., Thakur S., Ochoa-Albiztegui R.E., Morris E.A., Pinker K. Clinical Role of Breast MRI Now and Going Forward. Clinical Radiology. [Electronic resource].