Normal Singleton Pregnancy: Management, Necessary Examinations, Risk Factors
Daria G.Gynecologist, fertility specialist, MD
21 min read·August 05, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Normal pregnancy means that there is one fetus with no genetic abnormalities that has been conceived naturally. It is generally characterized as physiological.
3D-Animation: Physiological Full-Term Pregnancy
Initially, the estimated due date (EDD) is set by adding 280 days to the first day of the last menstrual period (LMP). However, this method is not always accurate as only 50 % of patients can remember the exact date of their LMP, and some women present with irregular menstrual cycles. Human chorionic gonadotropin (hCG) and ultrasound may help specify gestational age.
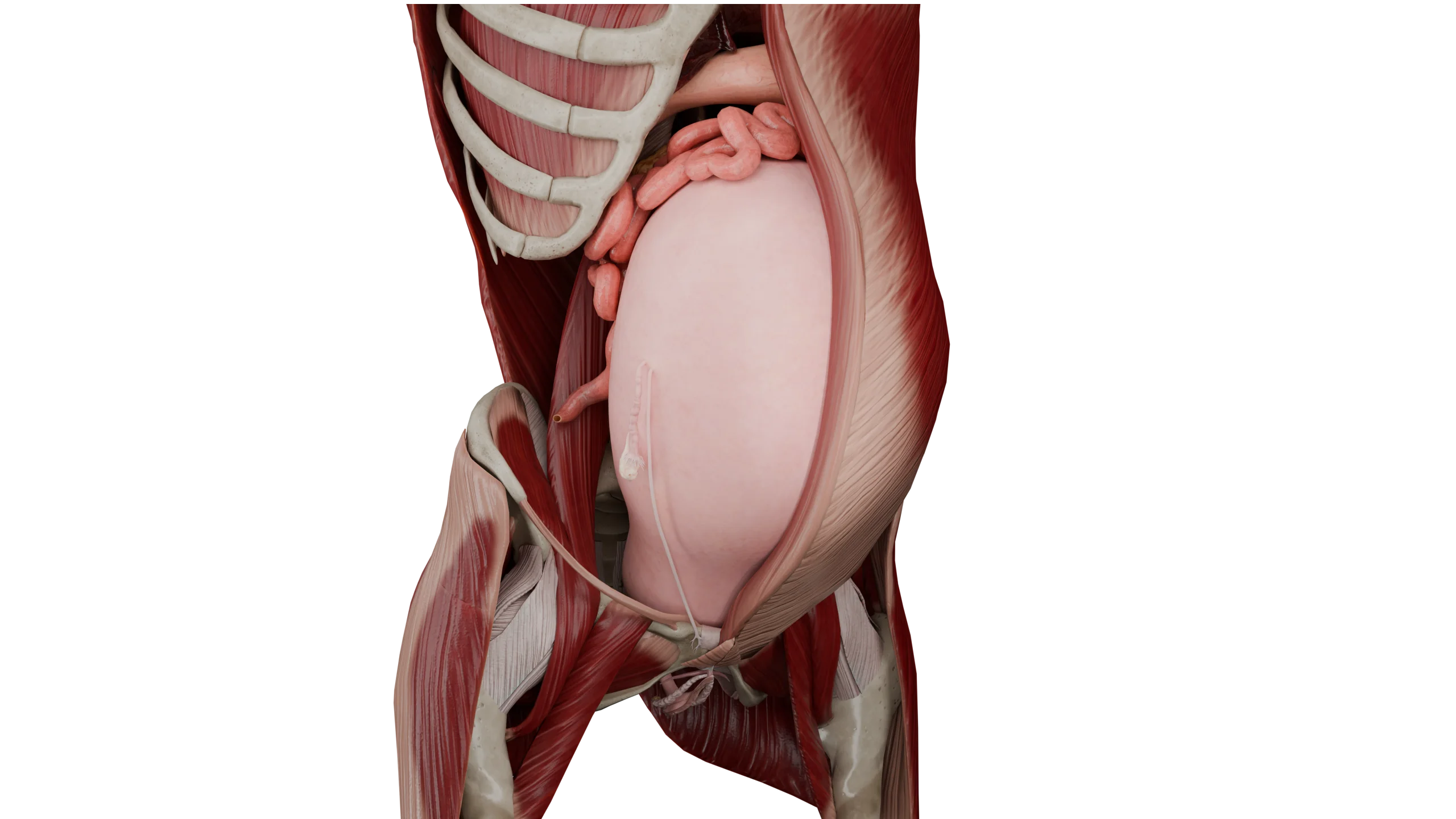
Anatomical Location of Visceral Organs in Full-Term Pregnancy
Uterus, Fetus, and Membranes
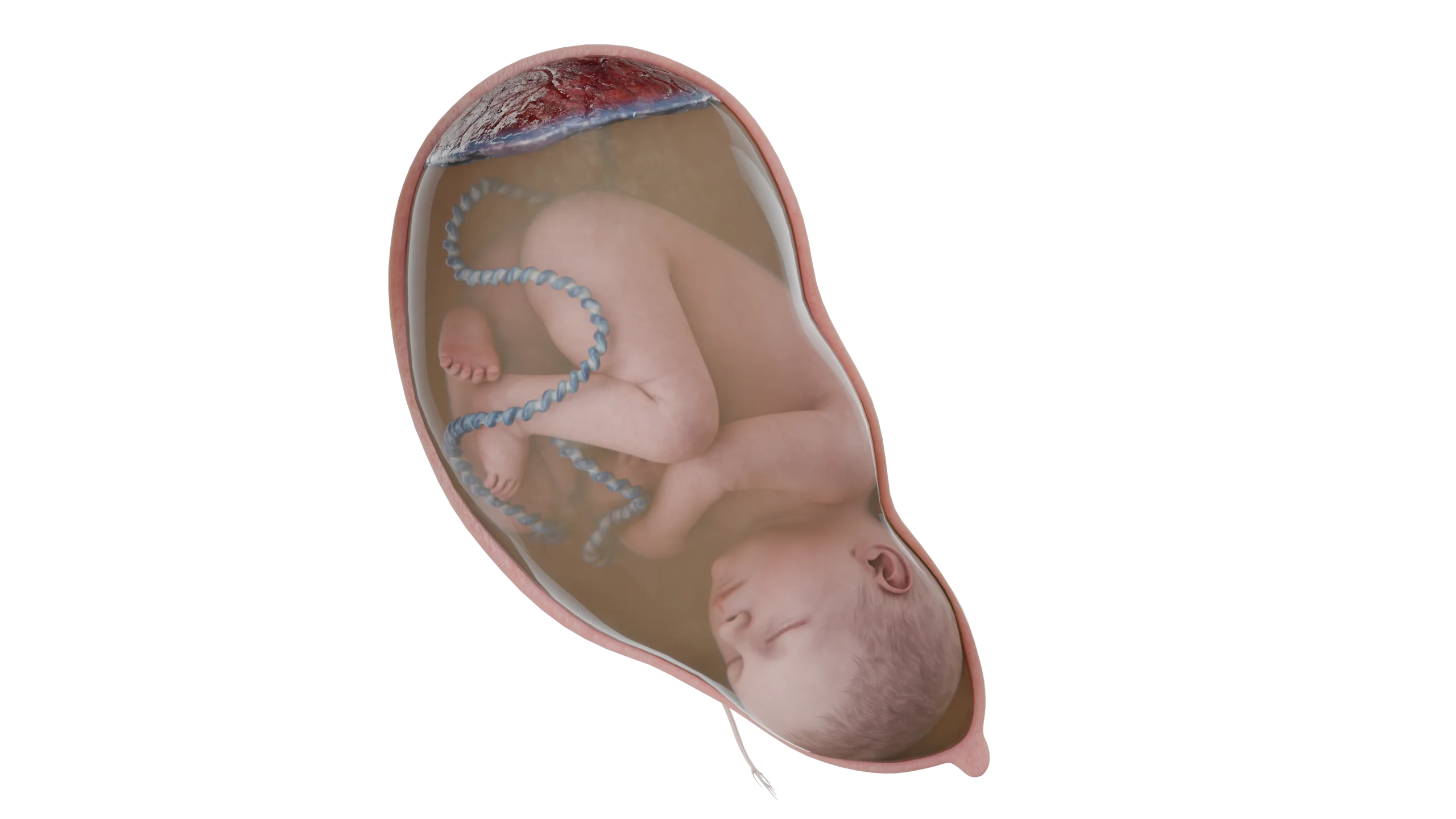
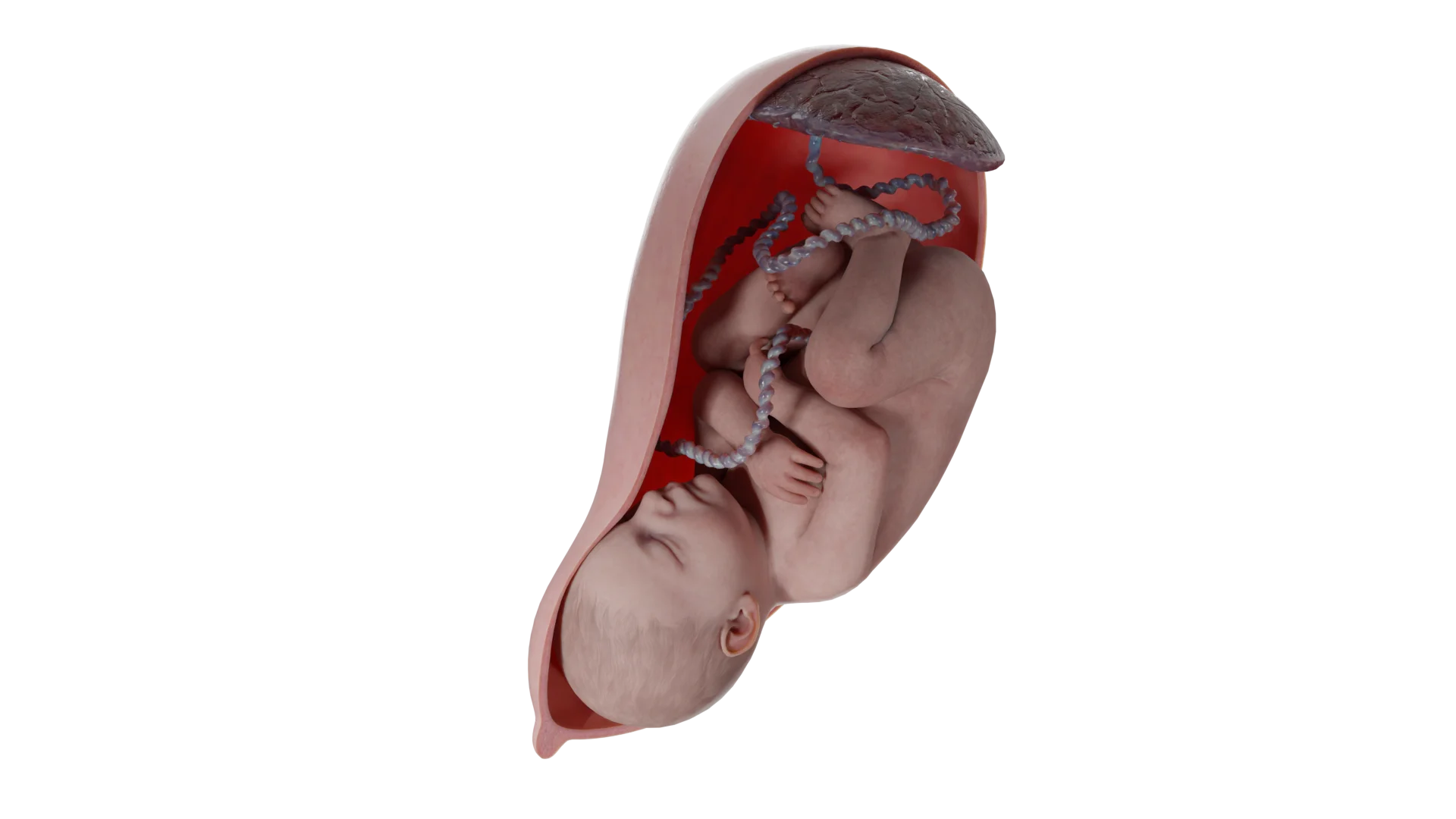
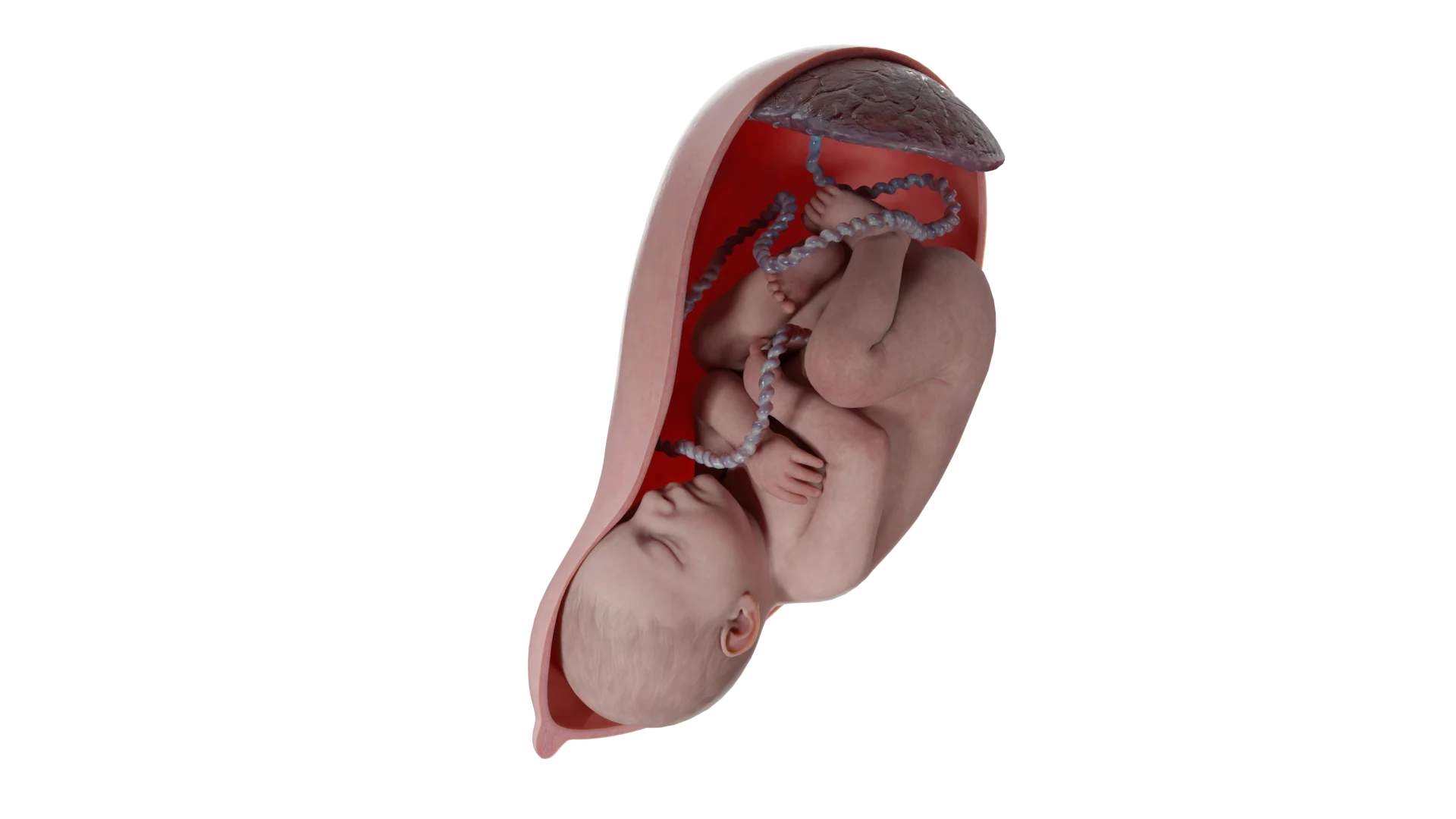
Fetus, Umbilical Cord, Placenta in Longitudinal Lie, Cephalic Presentation
Longitudinal Fetal Lie
Examination in Physiological Pregnancy
During the initial visit, a patient with a diagnosed pregnancy should be referred for a set of laboratory tests. Patients with risk factors may be offered additional laboratory tests if needed.
General clinical blood tests
Blood typing;
Red blood cell (RBC) antibody screen;
Complete blood count;
Urinalysis, urine culture.
Infection screening during pregnancy
Gonorrhea;
Chlamydia;
Syphilis;
Human immunodeficiency virus (HIV);
Hepatitis B virus;
Hepatitis C virus;
Rubella;
Varicella;
Human papillomavirus (HPV) if medical history reveals abnormal cervical screening;
Herpes simplex virus (HSV);
Asymptomatic bacteriuria;
Tuberculosis;
Group B streptococcus (GBS), one of the major causes of severe neonatal infections (e.g., sepsis, meningitis, pneumonia) within the first 7 days of life. Antenatal screening is generally recommended for all pregnant women from Week 36 Day 0/7 to Week 37 Day 6/7.
Pathology diagnosis:
Cervical culture to identify HPV DNA — screening for cervical cancer;
Thyroid stimulating hormone level — identification of thyroid gland diseases;
First Ultrasound
This is a mandatory examination typically performed in the first trimester to determine or confirm gestational age, EDD, and heartbeat.
US may also be indicated to:
Determine causes of vaginal bleeding;
Confirm ectopic pregnancy;
Identify a multiple pregnancy and monitor its course;
Detect any abnormalities of the uterus or other pathologies of the pelvic organs.
Patients complaining of bleeding or pain should be immediately referred for an ultrasound upon visiting a healthcare facility.
Genetic Screening
Irrespective of risk factors and maternal age, screening for fetal aneuploidy is a mandatory prenatal examination. Modern techniques based on cell-free DNA aim to identify an overall level of acellular DNA of chromosomes 21, 18, 13, and X. This test may be performed from Week 10 of pregnancy.
It evaluates the following risks in newborns:
Trisomy 21 — a genetic disorder caused by 3 copies of chromosome 21 in all body cells. This is the most common reason for Down syndrome.
Trisomy 18 — a genetic disorder caused by 3 copies of chromosome 18 in all body cells. This anomaly is referred to as Edwards syndrome.
Trisomy 13 — a genetic disorder caused by 3 copies of chromosome 13 in all body cells. This anomaly is known as Patau syndrome.
Monosomy X — a genetic disorder caused by the presence of only 1 copy of chromosome X. This anomaly is called Turner syndrome.
Note that this test only indicates the likelihood of aneuploidy. Biopsy of chorionic villi or amniocentesis are utilized for a more accurate diagnosis.
Aneuploidy tests are typically supplemented by alpha-fetoprotein (AFP) tests in pregnant women. Performed between Weeks 15 and 22 of pregnancy, this blood serum analysis helps detect neural tube defects. It should be stressed that it is not a part of the first trimester screening.
Genetic testing may also be performed prior to pregnancy. In this case there is no need for reexamination in the future. Genetic tests aim to identify hemoglobinopathy, cystic fibrosis carriers, and spinal muscular atrophy.
Patients with a relevant family history of genetic abnormalities must be referred for expanded carrier genetic testing.
Risk Factor Evaluation
Upon initial examination to prevent pregnancy complications a healthcare professional should assess certain risk factors (if any).
Preeclampsia
Preeclampsia is one of the leading causes of maternal morbidity and mortality. In patients with underlying liver or kidney conditions, early assessment may include a comprehensive metabolic panel and urine protein-to-creatinine ratio (UPRC).
African population (due to social, not biological factors);
Low income;
Patients 35 years of age or older;
In vitro conception;
Individual risk factors.
Patients with one or more high risk factors or two or more moderate risk factors should take low-dose aspirin starting from Week 12 to Week 28 of pregnancy (optimal duration of up to Week 16).
Diabetes mellitus
Gestational diabetes mellitus (GDM) may develop in 4 % of all pregnancies. Risk factors:
A history of a pregnancy complicated by GDM;
Excess weight or obesity;
A family history of DM;
Patients of certain ancestries (African American, Latin American, American Indian, Alaska Native, Native Hawaiian, or other Pacific Islanders);
Patients receiving antiretroviral therapy.
Early GDM screening is indicated in cases of multiple GDM risk factors. Unlike standard screening at Weeks 24–28, these tests are typically performed at Weeks 14–20.
Premature birth
Premature birth occurs in 10 % of cases. It is the main cause of perinatal morbidity and mortality.
Risk factors:
A history of premature birth;
Multiple pregnancies;
Cervical incompetence.
Depression screening
Women should undergo depression screening during the initial visit, at Week 28 of pregnancy, and in the postpartum. The screening should be performed using the Edinburgh Postnatal Depression Scale (EPDS). The Patient Health Questionnaire-9 (PHQ-9) may also be employed.
Psychoactive drug abuse
Alcohol, tobacco, cannabis, or teratogenic drug abuse is a widespread issue that may lead to various side effects.
Immune status assessment
All pregnant and breastfeeding women should be immunized in accordance with the vaccination schedule in effect in their country of residence. Vaccination is a reliable method to reduce the risk of certain diseases during pregnancy. During each pregnancy, women should be vaccinated against whooping cough and flu.
Pelvic floor muscles
At the early stages of pregnancy, a brief assessment of pelvic floor muscles should be performed (via palpation). Patients should then be instructed on how to properly constrict their muscles not involving any compensatory patterns (for instance, activating the gluteal or adductor muscles).
Frequency of visits during pregnancy
The frequency of visits is determined individually. Typically, patients with an uncomplicated first pregnancy should be followed every 4 weeks up to Week 28 of pregnancy, every 2 weeks at Weeks 28–36, and then every week until delivery.
At every visit, a healthcare professional should assess a set of data, including complete blood count and urinalysis, blood pressure, patient’s weight, fundal height to evaluate fetal growth, as well as fetal cardiac activity and movement corresponding to the gestational age.
Fetal ultrasound in 2nd and 3rd trimesters to assess anatomical features
The method helps assess fetal growth and anatomy and identify developmental abnormalities (if any). Ultrasound is recommended to specify:
Gestational age;
Fetal number;
Fetal viability;
Anatomy;
Placenta position;
Amniotic fluid volume;
Condition of the pelvic organs.
Optimal timing for fetal anatomy ultrasound:
From Week 18 to Week 22 of pregnancy in the second trimester;
From Week 32 to Week 35 of pregnancy in the third trimester.
Malformation screening aims to significantly reduce perinatal mortality and morbidity, as well as maternal morbidity. Prenatal testing provides data to therapeutically terminate a pregnancy for medical reasons. In this case, the termination is performed in the early stages of pregnancy, which is less psychologically traumatizing for patients.
Labor management in singleton pregnancy
The onset of labor after Week 24 of pregnancy is determined by regular painful uterine contractions that lead to dilation and effacement of the cervix.
The first stage of labor covers the timeframe from the onset of labor to full cervical dilation, up to 10 centimeters. In turn, the first stage of labor may be subdivided into the latent and active phases.
The latent phase of labor is characterized by gradual and relatively slow cervical dilation. It starts with regular uterine contractions and ends with complete cervical effacement.
The active phase lasts from approximately 6 cm to complete cervical dilation.
The second stage of labor ends with the delivery of the neonate.
The third stage of labor covers the period between the birth of a newborn and the delivery of the placenta.
Order of fetal movements through pelvis in occipito-anterior presentation
Head descent and flexion: The head enters the pelvis in an occipito-transverse position, while the fetal chin is tucked onto the chest.
Internal rotation toward occipito-anterior position: The movement happens at the level of the ischial spine when the interparietal suture takes a longitudinal position, and the point of fixation is set under the pubic symphysis.
Head extension: The movement occurs in the plane of the pelvic outlet.
External rotation: When reaching the levators, the shoulders rotate until the neonatal bisacromial diameter is set in an anteroposterior direction.
Anterior shoulder delivery: The process occurs when the fetal body bends posterolaterally.
Posterior shoulder delivery: The process occurs when the fetal body bends anterolaterally, then the rest of the body is delivered.
In cases of occipito-posterior presentation, the fetal head should be additionally bent after its internal rotation.
First stage of labor
Monitoring during first stage of labor (partogram)
A detailed medical history should be collected, and pregnancy progress should be assessed.
Abdominal palpation is performed to identify the fetal position and presentation; contractions frequency and duration should be recorded every 30 minutes.
The fetal status should be assessed, including its heart rate and the color/volume of the leaked amniotic fluid. Measurements should be carried out every 30 minutes or continuously by means of CTG.
The mother’s condition should also be evaluated. Her heart rate is monitored on an hourly basis, while blood pressure (BP) and body temperature are measured every 4 hours. Urinalysis (including ketone bodies and protein) is performed at 4-hour intervals as well. Analgesia may be administered if indicated.
Vaginal status evaluation: cervical dilation is monitored continuously, and the fetal head position should be determined every 4 hours or once the obstetric situation changes.
If indicated, amniotomy (rupture of the amniotic fluid sac) may be performed; the check-up is repeated 2 hours later.
Second stage of labor
Labor should start within 1 hour or 40 minutes of the active pushing phase in nulliparous and multiparous women, respectively. The fetal status is monitored continuously with CTG. A patient’s condition is also monitored closely in this period:
Consciousness;
Skin and mucosa color;
Heart rate and BP.
Women may choose their position for delivery:
Seated;
In a hand- and legstand or vertically;
In the supine position.
Crowning (visible top of the fetal head) tends to stretch the perineum and anus. At this stage, an obstetrician should prevent the fetal head from premature extension and control the labor speed. To this end, the obstetrician creates a minor obstacle with four fingers on one hand applied to the fetal head. If there is a threat of a perineal tear, episiotomy or perineotomy (a surgical incision of the perineum and the posterior vaginal wall) should be performed; however, the procedure should not be done routinely.
To reduce the risk of a perineal tear, the fetal head should not come out during a contraction. If the shoulders do not come out naturally, the first step is to carefully bend down the head. This technique facilitates the birth of the anterior shoulder. Then, the fetal head is lifted anteriorly, and the perineum is shifted inferiorly from the posterior shoulder, thus preventing trauma.
If this is ineffective a healthcare professional may opt for procedures used in shoulder dystocia. After birth, the umbilical cord is clamped (twice) and cut. If clamping is delayed for 2–3 minutes, it may lead to increased Hct (hematocrit) in infants. Te baby’s condition is assessed according to the Apgar score at minutes 1, 5, and 10 after birth.
If the delivery does not happen within 1 hour after the onset of the active pushing phase, surgical options may be considered. These include vacuum assisted delivery or a cesarean section.
Note that vacuum assisted delivery requires:
A live fetus;
Complete cervical dilation;
No amniotic sac;
Alignment of the mother’s pelvis and the baby’s head dimensions;
The fetal head located in the broad, narrow part of the cavity or at the pelvic outlet;
Occipital or occipito-anterior presentation;
Active participation of a parturient woman;
The patient’s informed consent.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Third stage of labor
The third stage of labor commences from the moment the fetus is born and lasts till the placenta, membranes, and umbilical cord are delivered. These structures are separated via less intense and painful contractions. During this process, the uterus significantly shrinks in size and takes a round shape, with the fundus located near the navel.
Before pushing, an obstetrician should perform controlled cord traction while holding the fundus of the uterus with their left hand. The umbilical cord should come off and stretch easily. In case the placenta delivery is complicated, specialized techniques may be applied.
The third stage of labor lasts approximately 30 minutes, irrespective of parity. If the process does not complete naturally, the placenta should be separated from the uterine wall and removed manually. This procedure is performed under anesthesia. A healthcare professional inserts their hand in the uterine cavity to determine the border of the placenta and separates it from the uterine wall twisting the wrist back and forth. Then, the placenta is removed by the umbilical cord via controlled cord traction, and the uterine cavity is checked again.
In cases of physiologic birth, blood loss does not exceed 250 ml or 0.5 % of a woman’s body weight. Otherwise, larger blood loss is considered pathological and requires a management strategy to halt the bleeding, accounting for the cause.
The causes of postpartum hemorrhage are as follows:
T (tonus): Inadequate uterine contraction — atony);
T (tissue): Retained placenta;
T (trauma): Injuries to the birth canal;
T (thrombin): Coagulation disturbances.
Irrespective of the blood loss volume, after the placenta has been delivered, a healthcare professional should examine the birth canal, the integrity of the placenta and membranes, and measure the woman’s heart rate and blood pressure. In case of bleeding, a pelvic exam and manual check of the uterine cavity are conducted. Additionally, lung auscultation is performed.
Late, or secondary postpartum hemorrhage (24 hours after delivery) may be caused by:
Remaining parts of the placenta;
Subinvolution of the uterus;
Postpartum infection;
Hereditary hemostasis disorders.
FAQ
1. What is considered a normal pregnancy?
A normal pregnancy is a physiological condition in which a single fetus develops in the uterus without complications affecting either the mother or the fetus. It typically lasts 280 days, calculated from the first day of the LMP. However, this time frame is approximate and may vary slightly.
2. Can a normal pregnancy occur with low hCG levels?
Low hCG levels in early pregnancy do not always indicate a problem. They may be associated with late ovulation or inaccurate estimation of gestational age. It is essential to monitor hCG growth pattern, as in early pregnancy, hCG levels should double every 48–72 hours.
3. What tests are required during a normal pregnancy?
During a normal pregnancy, a woman should undergo basic laboratory tests, including a complete blood count and urinalysis, as well as screening for infectious diseases such as gonorrhea, chlamydia, HIV, and hepatitis. It is also important to perform ultrasound examinations and genetic testing to detect aneuploidies and other abnormalities.
4. Is pregnancy possible after a chemical pregnancy?
Yes, pregnancy can occur again after a chemical pregnancy. However, it is important to consult a healthcare provider to determine whether further diagnostic evaluation is needed.
5. How does a normal pregnancy develop after an ectopic pregnancy?
A woman can become pregnant again after an ectopic pregnancy. However, a thorough medical evaluation is necessary to rule out any infectious or anatomical factors that may have contributed to the previous condition.
6. How long does a normal pregnancy last?
A normal pregnancy usually lasts 40 weeks, or approximately 9 months. However, variations are possible, and delivery may occur between Weeks 37 and 41 of gestation. This variation is considered normal provided that no complications are observed.
7. How should a normal pregnancy be managed?
To sustain a normal pregnancy, it is important to undergo regular prenatal check‑ups, monitor blood pressure, and track weight gain and edema throughout gestation. Ultrasound examinations help monitor fetal development, while maintaining proper nutrition and an appropriate level of physical activity support maternal health.
References
1.
VOKA Catalogue.
https://catalog.voka.io/
2.
Всемирная организация здравоохранения. Рекомендации ВОЗ по оказанию дородовой помощи для формирования положительного опыта беременности [Электронный ресурс]. – Женева : ВОЗ, 2023.
https://www.who.int (дата обращения: 30.07.2024).
3.
FIGO Guidelines. Guidelines for the Management of Normal Pregnancy and Intrapartum Care // International Journal of Gynecology & Obstetrics. – 2023. – Vol. 160, Suppl. 1. – P. 5–23. DOI: 10.1002/ijgo.14500.
4.
American College of Obstetricians and Gynecologists. Guidelines for Perinatal Care. 9th ed. – Washington, DC : ACOG, 2023. – 320 p.
5.
National Institute for Health and Care Excellence. Antenatal care for uncomplicated pregnancies [Электронный ресурс] : клинические рекомендации. – L. : NICE, 2023. – (NG201).
Royal Australian and New Zealand College of Obstetricians and Gynaecologists. Management of Pregnancy Care (C-Obs 3). – Melbourne : RANZCOG, 2024. – 42 p.
7.
Society for Maternal-Fetal Medicine. Guidelines for Antenatal Fetal Monitoring in Low-Risk Pregnancies // American Journal of Obstetrics and Gynecology. – 2023. – Vol. 228, № 5. – P. B2–B12. DOI: 10.1016/j.ajog.2022.12.001.
8.
Всемирная организация здравоохранения. Международная классификация болезней 12-го пересмотра (МКБ-12) : акушерские критерии. – Женева : ВОЗ, 2023. – 180 с.
9.
European Society of Gynaecological Oncology; European Society of Human Reproduction and Embryology. Optimal Management of Low-Risk Pregnancy: European Consensus Statement // Human Reproduction Open. – 2023. – Vol. 2023, № 3. – P. 1–15. DOI: 10.1093/hropen/hoac058.