




Vulvitis: Predisposing Factors, Clinical Manifestations, Diagnosis, and Treatment
Vulvitis refers to vulvar inflammation affecting the labia, clitoris, mons pubis, and vestibule of the vagina. Clinical manifestations, diagnosis, and treatment.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Tuberculosis (TB) is a life-threatening chronic granulomatous inflammatory disease caused by Mycobacterium tuberculosis. Genital TB in women is more common between the ages of 18 and 35.
3D Model of endometrium damaged by Mycobacterium tuberculosis:
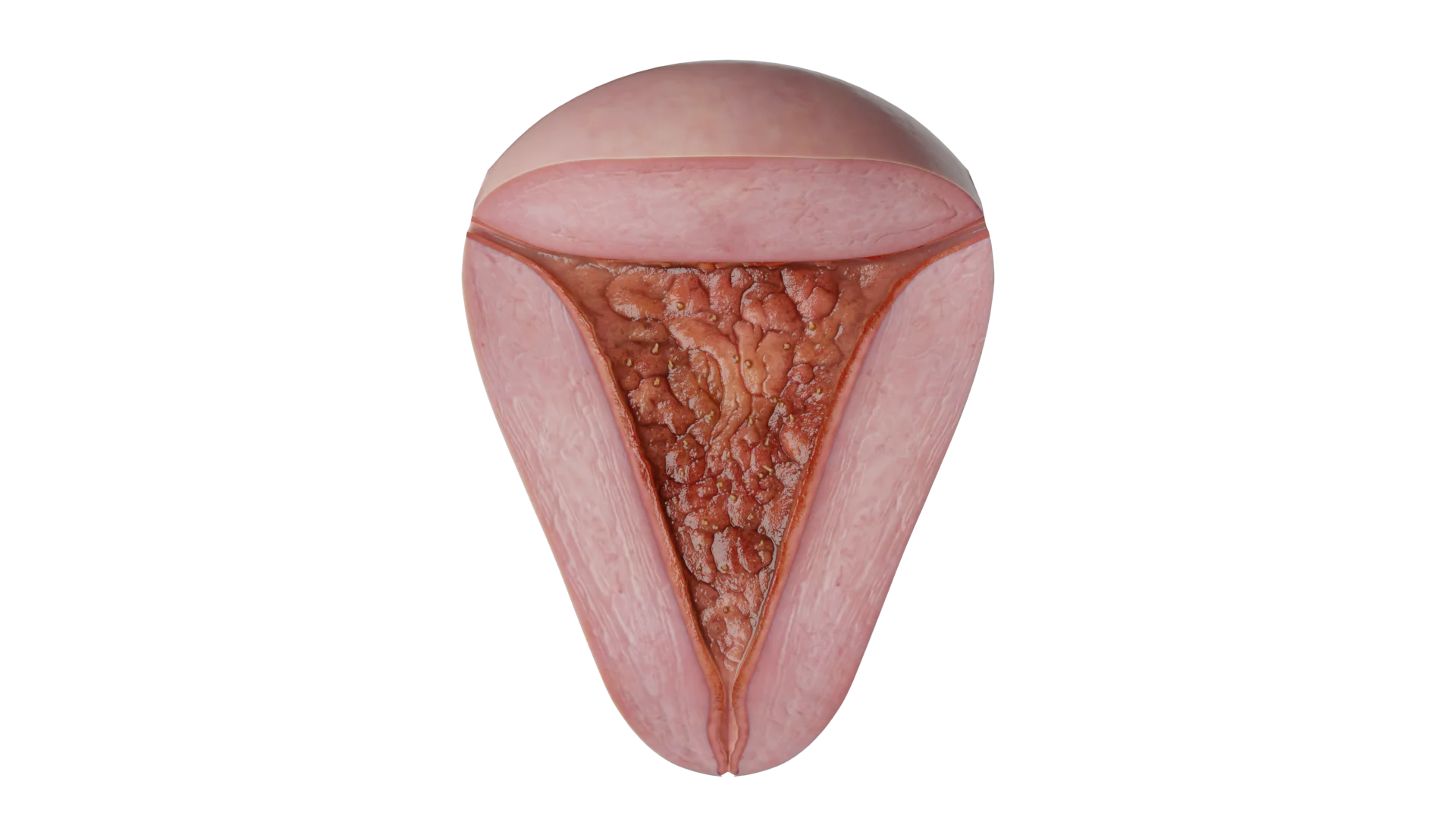 Endometrium damaged by Mycobacterium tuberculosis
Endometrium damaged by Mycobacterium tuberculosis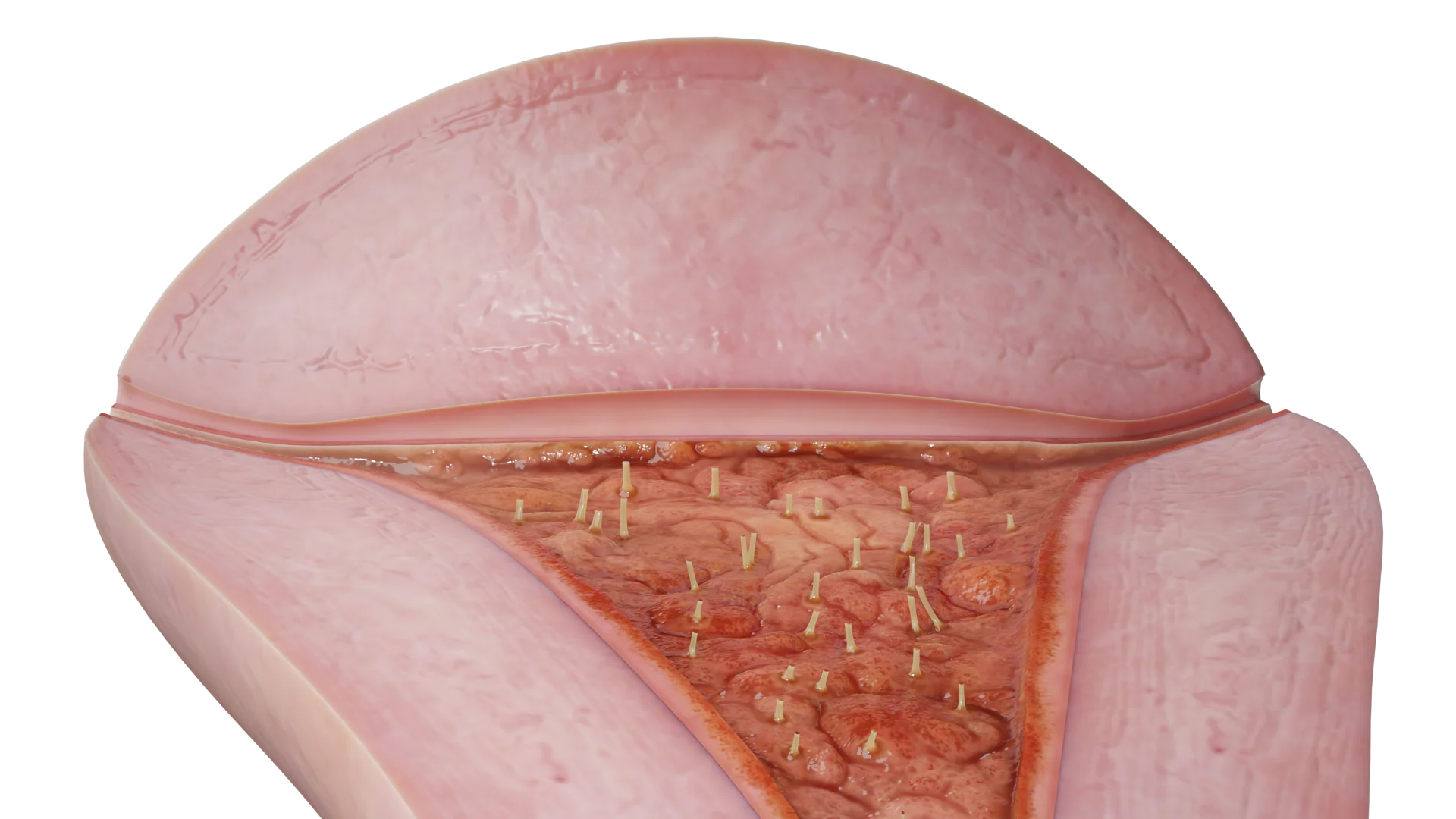 Synechiae in the uterine cavity formed as a result of endometritis
Synechiae in the uterine cavity formed as a result of endometritis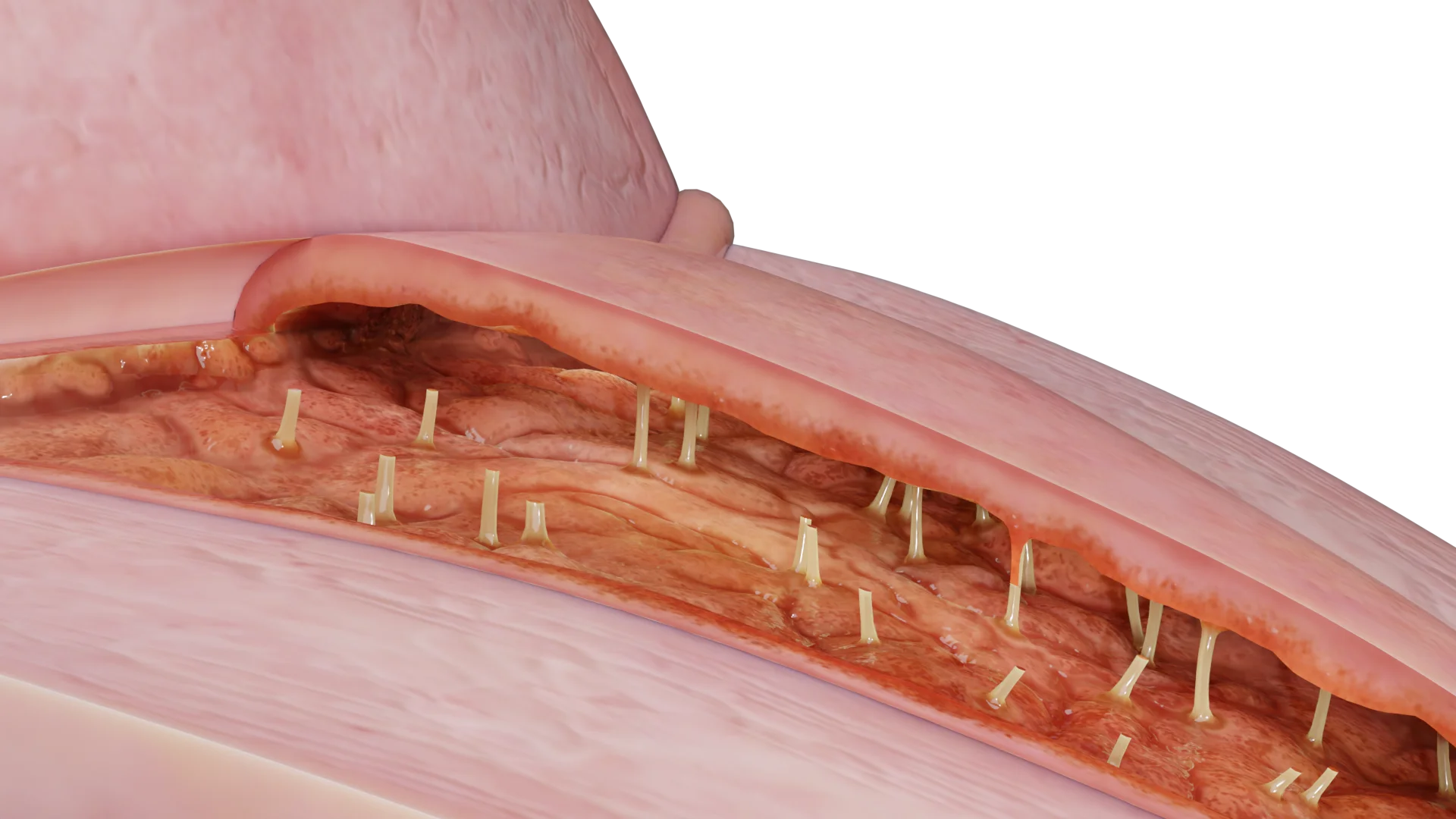 Tuberculous endometritis: posterior uterine wall
Tuberculous endometritis: posterior uterine wallTuberculous endometritis is a specific inflammation of the endometrium of the uterus caused by mycobacterial lesions of the mucous membrane. This disease develops slowly, is often asymptomatic in the early stages and can lead to irreversible changes in the uterus, which in turn can affect a woman’s reproductive function.
Manifestation of the disease, as a rule, is not associated with the onset of sexual activity. The onset of sexual activity may cause an exacerbation and transform a latent process into a reactive one. Isolated uterine involvement occurs in 10-15% of cases. In most cases, the uterus is affected together with the tubes (50-55%). The endometrium is most often affected (50-60%), in which tubercles characteristic of tuberculous lesions are formed.
The uterine mucosal glands near the tubercles are destroyed. If only the functional layer of the uterine mucosa is affected, the endometrium, together with the tubercles and mycobacteria, is rejected during the first menstruation, resulting in spontaneous cure. If the tuberculous process goes to the basal layer and deeper, the process of self-healing becomes more difficult.
The emergence of genital tuberculosis is more often associated with reactivation of mycobacterial infection from systemic distribution of mycobacterium during primary infection by hematogenous route. Direct transmission of mycobacteria between sexual partners has been established. Spread from other intra-abdominal foci is rare.
Manifestation of genital tuberculosis is varied and depends on the general condition and resistance of the organism. In most cases, the disease develops slowly, without any characteristic symptoms. Later it acquires a chronic, often recurrent course, especially when the uterine appendages and pelvic peritoneum are affected. Less often the disease begins acutely, accompanied by a significant rise in temperature, abdominal pain, with phenomena of irritation of the peritoneum. It has been established that a rapid onset of the disease in genital tuberculosis is observed in cases of mixed infection.
Common symptoms include:
On the genital side, patients complain of menstrual irregularities of the menstrual cycle type:
However, in the initial stages, women of reproductive age may be diagnosed with abnormal uterine bleeding. Patients also report low back and lower abdominal pain, and less frequently abnormal vaginal discharge, dyspareunia and infertility. In cases of self-healing, especially in childhood or puberty, scarring occurs as a result of healing, with partial or complete obliteration of the uterine cavity and atrophy of the endometrium, causing persistent primary amenorrhea.
Infertility develops in 60-95% of women as a result of genital tuberculosis. Primary infertility is more common than secondary infertility. The cause of infertility in tuberculosis is more often a lesion of the Fallopian tubes and less often – the lesion of the uterine mucosa. The diagnosis can be established after separate diagnostic scraping and culture for mycobacterial culture or PCR-diagnosis.
Histologic examination reveals perivascular infiltrates, fibrosis or caseous decay of tuberculin tubercle tubercles.
The use of cytologic examination of uterine cavity contents and cervical smears, which detects giant Langhans cells specific for tuberculosis, is relevant. Caseous necrosis is rare and is usually diagnosed in severe forms. It reveals an ulcerative lesion of the uterine mucosa, which is more often diffuse and progresses to the caseous form, penetrating into the thickness of the muscular wall of the uterus.
Pyometra forms when curd-purulent decay accumulates in the uterine cavity in cases of obliteration of the internal pharynx.
Microbiological methods are considered to be the most reliable diagnostic methods. Seeding of material from the uterine cavity is performed at least 3 times on dense artificial nutrient media. Also, the diagnosis of mycobacteria is possible using a highly sensitive and specific PCR method. However, this method has difficulties in interpretation and implementation, since the material for the study can lead to false-negative results. It is worth saying that sowing menstrual discharge for mycobacterial culture more often shows a positive result than biopsy samples.
Hysteroscopy as a diagnostic method has limited application.
Injection of tuberculin to assess the immune response. This is an additional method that alone cannot be used to establish or exclude the diagnosis of tuberculosis. Blood can also be tested for levels of interferon-γ, which is produced in response to mycobacterial antigens. This test is an alternative to skin testing.
If there is no possibility of histologic and bacteriologic examination, the diagnosis is established on the basis of the totality of the results of clinical examination. X-ray examination (hysterosalpingography) plays the leading role in this case.
Radiographs show features typical of genital tuberculosis:
Pathologic shadows are visualized during the review radiography of the pelvic organs. They are represented by calcinates in the tubes, ovaries, lymph nodes, foci of caseous decay.
Ultrasound examination of the pelvic organs is also possible, but a highly qualified specialist is needed to make a diagnosis.
Find more scientifically accurate content on our social media








Chemotherapy with antituberculosis drugs is the therapy of choice. The intensity and duration of treatment is determined by the clinical form, prevalence and phase of the disease. Inappropriate treatment can cause the development of drug resistance of the bacterium, which leads to a worsening of the pathologic process.
Drugs in the first (basic) class include:
Drugs from the reserve group are prescribed to patients with drug-resistant forms. The reserve group includes:
Antituberculosis therapy has significantly reduced the use of surgical treatment, which is now used for certain indications. The main indications for surgical treatment are:
Tuberculosis treatment guidelines recommend a minimum of 6 months of treatment, provided pyrazinamide is taken during the first 2 months of treatment and the body is receptive to therapy.
Surgical therapy usually consists of a total abdominal hysterectomy and bilateral salpingo-oophorectomy. Surgery should be performed at least 6 weeks after initiation of antituberculosis therapy, as antimicrobial therapy facilitates the extent of surgery and reduces the risk of perioperative complications.
Untreated TB poses a greater risk to a pregnant woman and her fetus than cured TB. Treatment should be started when the likelihood of TB is medium to high.
Features:
Treatment regimens for tuberculosis in pregnant women
| Diagnosis | Therapy |
|---|---|
| Latent tuberculosis infection | A course of rifampicin |
| A course of isoniazid with pyridoxine supplementation | |
| Active tuberculosis | The preferred initial regimen is isoniazid, rifampicin and ethambutol, followed by isoniazid and rifampicin |
| Streptomycin should not be used as it has been shown to have harmful effects on the fetus | |
| Pyrazinamide is not recommended because its effects on the fetus are unknown |
Drugs that are contraindicated in pregnant women:
Pregnant women being treated for drug-resistant tuberculosis should be counseled regarding the risk to the fetus because of the known and unknown risks associated with back-up-line antituberculosis drugs.
Breastfeeding is not contraindicated in women being treated with first-line antituberculosis drugs because the concentrations of these drugs in breast milk are too low to cause toxicity in the newborn.
For the same reason, drugs in breast milk are not an effective treatment for tuberculosis or latent tuberculosis infection in newborns. Rifampicin may cause orange staining of body fluids, including breast milk. Orange staining of body fluids is expected and harmless.
1. What is tuberculous endometritis?
2. What are the causes of endometrial tuberculosis?
3. How does tuberculous endometritis manifest?
4. Can I get pregnant with endometrial tuberculosis?
5. How can tuberculous endometritis be prevented?
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Tanner MR, Miele P, Carter W, et al. Preexposure Prophylaxis for Prevention of HIV Acquisition Among Adolescents: Clinical Considerations, 2020. MMWR Recomm Rep 2020;69(No. RR-3):1–12.
3.
Aflandhanti PM, Yovi I, Suyanto S, Anggraini D, Rosdiana D. Efficacy of pretomanid-containing regiments for drug-resistant tuberculosis: A systematic review and meta-analysis of clinical trials. Narra J. 2023 Dec;3(3):e402. PMCID: PMC10919689.
4.
WHO consolidated guidelines on tuberculosis: Module 4: Treatment and care [Internet]. Geneva: World Health Organization; 2025. Chapter 2, Drug-resistant TB treatment.
5.
WHO announces landmark changes in treatment of drug-resistant tuberculosis. Geneva: World Health Organization; 2022.
6.
Global Drug Facility [website]. Geneva: Stop TB Partnership; 2023.
7.
Sharma JB et al. (2020) “Genital tuberculosis in infertile women: Clinical, hysteroscopic, and histopathological features.”*Journal of Human Reproductive Sciences, 13(1), 3–9.
8.
Grace GA et al. (2019) Endometrial tuberculosis: A clinicopathological study in an infertility clinic.”* International Journal of Gynecology & Obstetrics, 147(2), 182–187.
9.
Malhotra N et al. (2018) Genital tuberculosis and infertility: A systematic review and meta-analysis. Human Reproduction Update, 24(4), 411–426.
10.
Bhanu NV et al. (2015) “A study of female genital tuberculosis with special reference to endometrial tuberculosis.” Indian Journal of Tuberculosis, 62(2), 84–88.




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io




