Skin Biopsy in Dermatology: Classification, Technique, and Diagnostic Value
Skin biopsy. This article covers punch, shave, and excisional techniques, specimen handling and fixation, and the role of biopsy in dermatology and oncology.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hematology
Hematopoiesis and blood-related disorders
Hepatology
Liver, gallbladder, and biliary tract diseases
Histology
Microscopic tissue and cell structures
Infectious diseases
Bacterial, viral, and parasitic infections
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Orthopedics
Bone, joint, and soft tissue disorders
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hematology
Hematopoiesis and blood-related disorders
Hepatology
Liver, gallbladder, and biliary tract diseases
Histology
Microscopic tissue and cell structures
Infectious diseases
Bacterial, viral, and parasitic infections
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Orthopedics
Bone, joint, and soft tissue disorders
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
PRP therapy (platelet‑rich plasma therapy), also widely known as plasmatherapy or autologous plasma therapy, is an invasive biostimulation technique in which a patient’s own blood plasma is injected to stimulate skin regeneration and to treat hair and scalp conditions.
PRP technology emerged in the 20th century, when concentrated platelets began to be used in the management of thrombocytopenia. After 1990, the method was introduced into dentistry and maxillofacial surgery, as platelets had demonstrated high regenerative potential. Somewhat later, PRP therapy became widely used in orthopedics and sports medicine, and in the early 21st century it entered dermatology and aesthetic medicine.
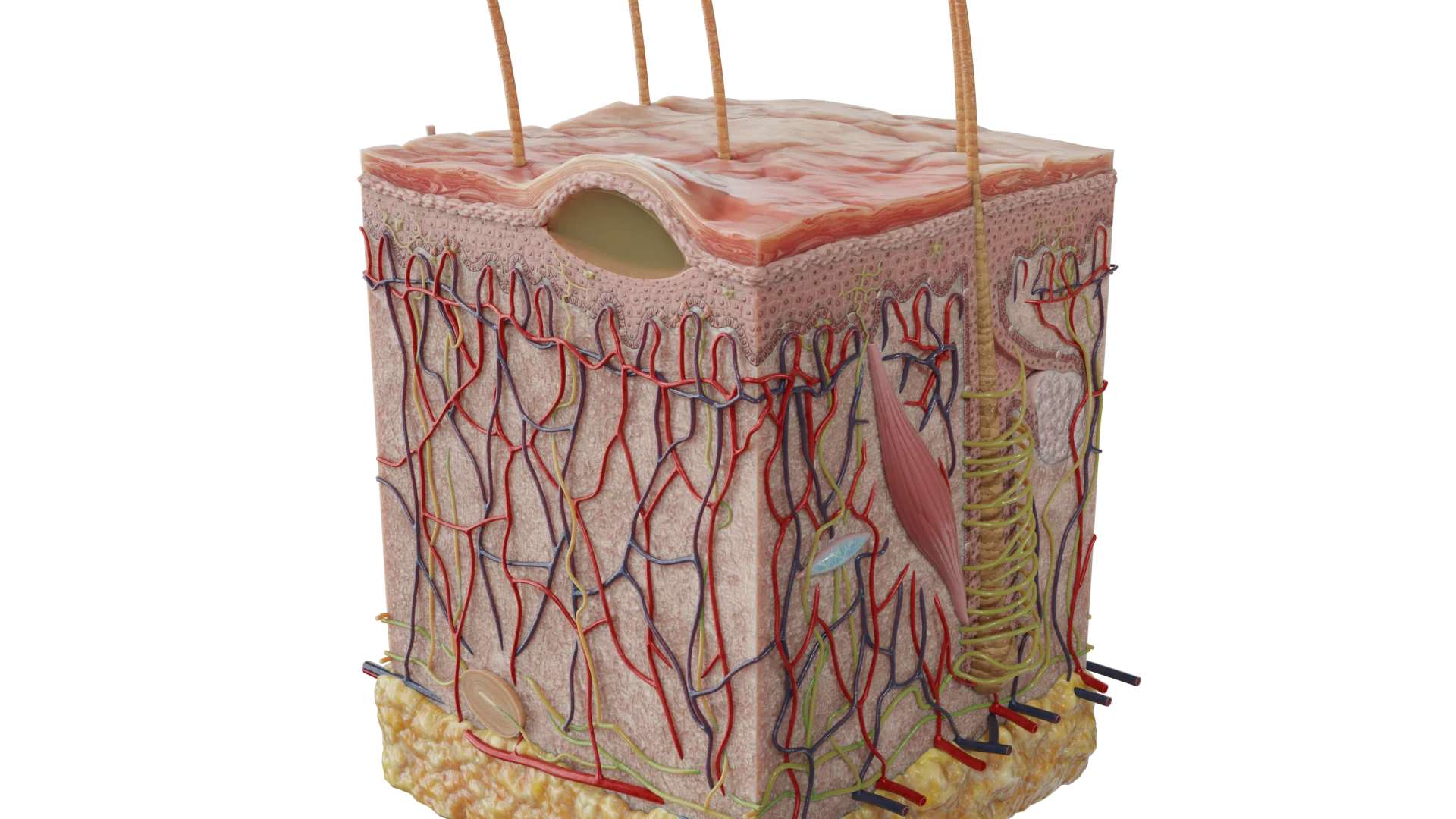
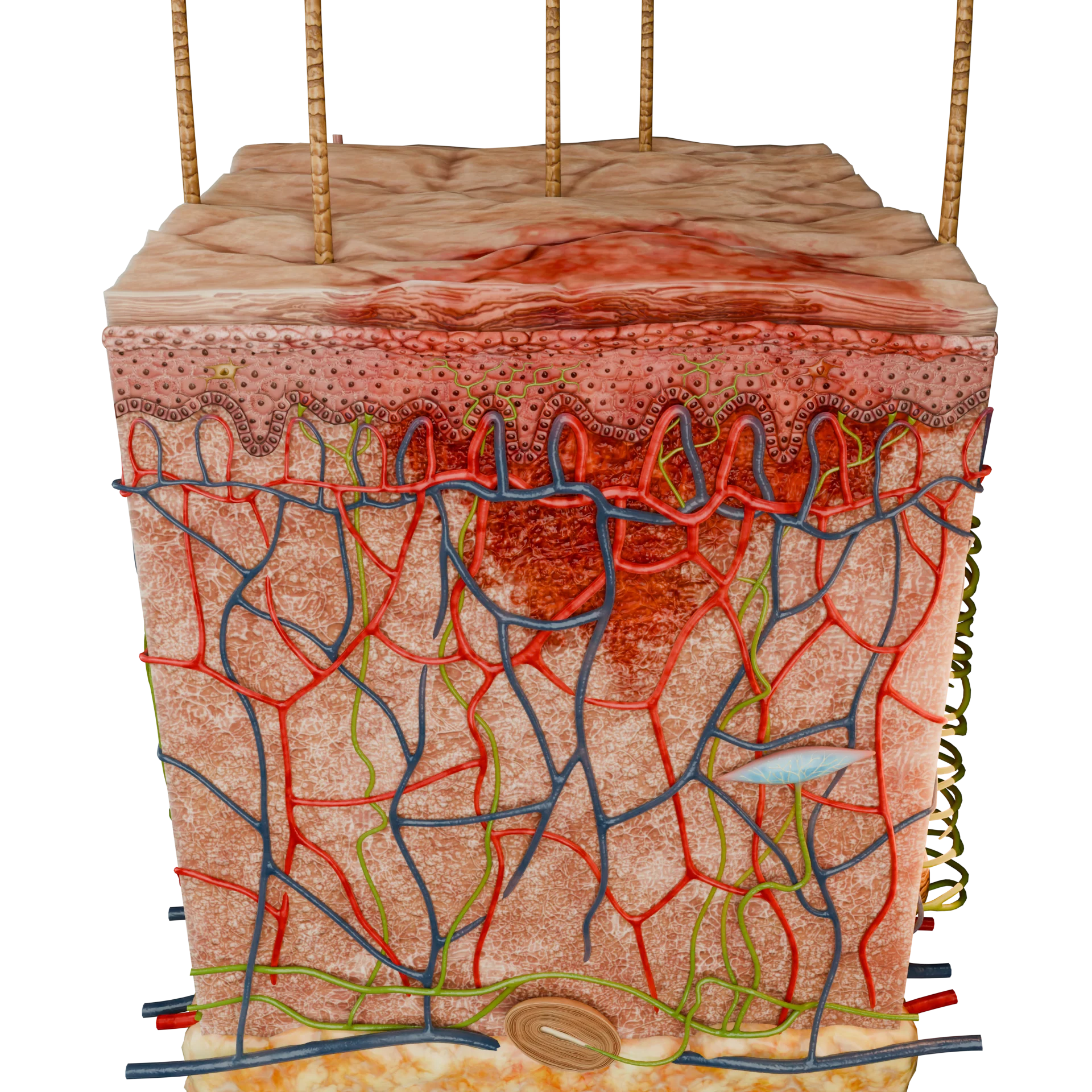
Injection of platelet‑rich plasma into the skin initiates a cascade of natural reactions:
As a result, powerful biostimulation of the face and body is observed, improving overall skin quality.
Platelet cytoplasm contains three types of secretory granules that are instrumental in therapy:
Growth factors stimulate migration and proliferation of fibroblasts, endothelial cells, and epithelial cells; promote extracellular matrix formation; intensify angiogenesis; and support connective tissue remodeling.
Key components of PRP therapy that contribute to its effectiveness include:
Different types of PRP therapy are classified by composition and concentration.
By composition of main components
By platelet concentration
Although many techniques for this procedure have been developed, all of them comprise several basic sequential stages:
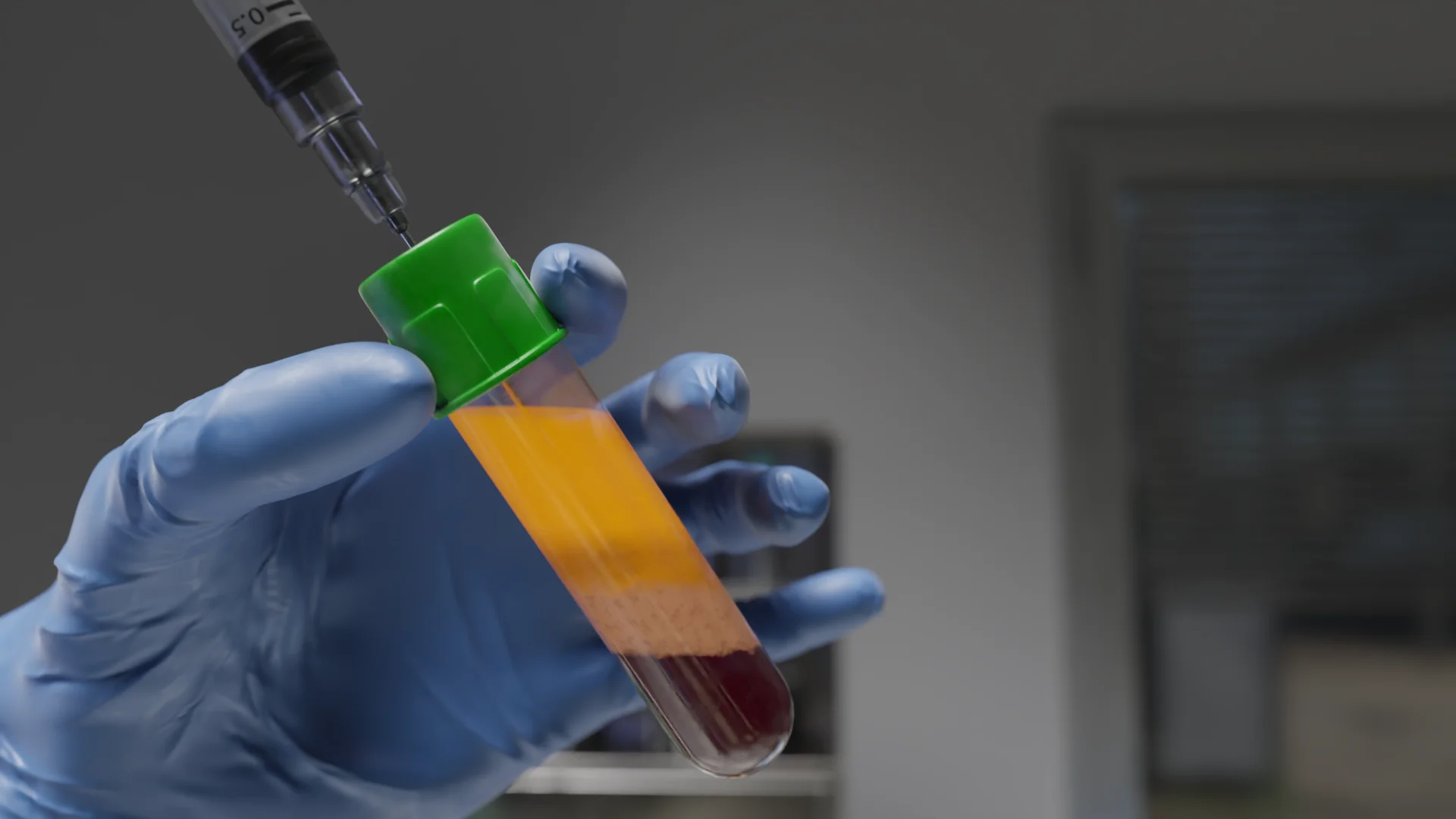
Depending on the required volume of plasma, an average of 10 to 200 mL of venous blood is collected into specialized vacuum tubes or standard anticoagulant syringes. Citrate, sodium heparin, lithium heparin, or complex preservatives may be used as anticoagulants.

PRP is obtained by single or double centrifugation of venous blood. During centrifugation, erythrocytes and platelets separate into three main fractions:

After cleansing the skin, applying topical anesthesia, and disinfecting the area, the obtained PRP is injected subcutaneously or intradermally using fine needles (30–32G) or cannulas, as well as via microneedling. Injection depth: 1–4 mm depending on the area.

During the first 48 hours it is recommended to: protect the skin from UV exposure, avoid baths and saunas, and limit intense physical activity.
Recommended course: 3–6 sessions spaced 2–4 weeks apart.
In aesthetic medicine, PRP therapy is used to address a wide range of concerns:

Hair and scalp PRP therapy improves microcirculation, activates follicular metabolism, and prolongs the anagen phase.
PRP therapy is considered effective and has a high safety profile, but in certain clinical situations it should be used with caution.
Side Effects: Most commonly limited to local reactions: swelling, erythema, and mild tenderness at the injection site. Small hematomas, slight itching, or firmness in the injection sites may also occur.
These manifestations usually resolve spontaneously within several hours or days and do not require specific treatment. Systemic reactions are extremely rare.
Benefits:
Limitations:
Find more scientifically accurate content on our social media








Beyond aesthetic medicine, PRP is actively used in:
Neurology: treatment of tunnel syndromes, neuropathies, and peripheral nerve repair.
1. PRP therapy vs. plasmolifting: what is the difference?
2. Is PRP therapy painful?
3. Is special preparation required?
4. How many sessions are needed for visible results?
5. Can PRP cause an allergy?
6. Can PRP be performed for acne?
References
1.
VOKA Catalog. [Electronic resource].
https://catalog.voka.io/
2.
Vladulescu D, Scurtu LG, Simionescu AA, Scurtu F, Popescu MI, Simionescu O. Platelet-Rich Plasma (PRP) in Dermatology: Cellular and Molecular Mechanisms of Action. Biomedicines. 2023 Dec 19;12(1):7. doi: 10.3390/biomedicines12010007. PMID: 38275368; PMCID: PMC10813350.
3.
Nilforoushzadeh MA, Roohaninasab M, Behrangi E, Jafarzadeh A, Nouri M, Zare S, Zare S. Phase I Clinical Trial: Evaluating the Efficacy, Safety, and Patient Satisfaction of Platelet-Rich Plasma (PRP) Injections and Microneedling for Androgenetic Alopecia Treatment. J Cosmet Dermatol. 2025 Sep;24(9):e70408. doi: 10.1111/jocd.70408. PMID: 40960112; PMCID: PMC12442246.
4.
Sadick NS, editor. Platelet-Rich Plasma in Dermatologic Practice. Cham: Springer; 2021. doi:10.1007/978-3-030-66230-1.
5.
Khetarpal S, editor. Aesthetic Clinician’s Guide to Platelet Rich Plasma. Cham: Springer; 2021. doi:10.1007/978-3-030-81427-4.
Loading test 6 questions
Table of Contents




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io