Systemic Enamel Hypoplasia: Etiology, Classification, Clinical Presentation, and Treatment
Daria V.Dentist, endodontist, DMD
12 min read·February 12, 2026
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Enamel hypoplasia is a quantitative and qualitative developmental defect of enamel in permanent or primary teeth due to factors disrupting ameloblast function.
Systemic enamel hypoplasia refers to developmental defects in all teeth or a group of teeth formed during a particular developmental stage due to metabolic disorders in the child or fetus.
Etiology
Enamel hypoplasia results from impaired ameloblast function during the follicular stage of tooth development. Factors affecting ameloblasts can be divided into several groups specified below.
Prenatal factors
Diseases and pathological conditions during the mother’s pregnancy (gestosis, rubella, toxoplasmosis, alcoholism, vitamin A and D deficiencies, diabetes mellitus, hypoparathyroidism, syphilis, cytomegalovirus infection, heart, kidney, and lung diseases, hypertension, or anemia);
Exposure to ionizing radiation during pregnancy;
Hypoalimentation or malnutrition during pregnancy;
Prolonged medication use during pregnancy.
Neonatal factors
Prematurity and/or low birth weight;
Factors related to childbirth (birth trauma, asphyxia);
Neonatal hypocalcemia, toxic injuries, neurological diseases, hyperbilirubinemia, prolonged diarrhea and vomiting, and neonatal infections with high fever.
Postnatal factors
Calcium and phosphorus metabolism disorders;
Endocrine diseases (affecting thyroid and parathyroid glands);
Acute infections associated with fever;
Hypovitaminosis A, C, D, or E, nutritional dystrophy;
Congenital allergy and related water-salt metabolism disorders;
Alimentary tract diseases;
Diarrhea with toxic symptoms;
Hemolytic jaundice;
Phenylketonuria, alkaptonuria;
Renal disorders;
Congenital Heart Defects;
Mercury poisoning;
Prolonged medication use;
Radiation therapy of the jaws in early childhood.
Despite a wide range of causal factors, the resulting clinical signs of enamel developmental defects are similar. Decreased or impaired ameloblast function due to external influences leads to alterations in the enamel matrix construction and its mineralization.
Relationship between defect depth and localization with the exposure period
The severity and localization of enamel defects reflect periods of metabolic disorders in the child’s body coinciding with amelogenesis and depend on the stage of tooth formation when the etiological factor acts, as well as the intensity and duration of its effect.
Lesion depth
In systemic enamel hypoplasia, a group of teeth formed during the same developmental period is affected; in the event of severe disease or frequent recurrence in the child or mother, all teeth may be impacted.
The width of the defective enamel area depends on the duration of the etiological factor’s exposure period;
The defect depth reflects the intensity of the exposure;
The number of defects indicates the frequency of metabolic disorders in the body, occurring upon the development of a new disease or recurrence of a previous one.
Lesion localization
The localization of enamel defects can approximately indicate the age when ameloblasts malfunctioned.
Affected tooth groups
Causal factor exposure period
Temporary tooth defects
Intrauterine period
Defects in the permanent teeth at the incisal edges of central incisors, on canines and cusps of first molars, as well as lateral incisors of the mandible
From 6 months to 1 year
Defects of the lateral maxillary incisors
After 1 year from birth
The crowns of the teeth are affected up to the gingival third, as well as the occlusal surfaces of the premolars and second molars
Up to 3-4 years of age
Enamel defects in hypoplasia are irreversible, as tooth enamel cannot be remodeled, unlike bone tissue.
Epidemiology
The epidemiology of systemic enamel hypoplasia is characterized by a high global prevalence, averaging 25.3%, with significant geographical variability (from ~7% in affluent regions of Europe to >40% in Asia and Oceania).
Traditionally, the key causes are considered biological factors of the perinatal period: prematurity and low birth weight can increase the risk of defect development up to 60%.
It is also necessary to consider socioeconomic status: a statistically significant association between low family income in the patient’s childhood and the presence of enamel defects has been proven. The etiology of enamel hypoplasia is recognized as strictly multifactorial, where the quality of medical care can modify the influence of biological risks.
A study on a modern European population showed that with the availability of perinatal medicine, typical factors (cesarean section, prematurity) are successfully compensated and do not lead to enamel defects, whereas the living standard plays a crucial role. No significant gender differences were identified (men and women are affected equally frequently). Morphologically, the most common form remains furrow-form (linear) hypoplasia (found in 93% of cases), most often affecting the maxillary incisors.
Classification of systemic enamel hypoplasia
Spotted form;
Erosive (pitting) form;
Furrow form;
Wavy form;
Cup-shaped form;
Mixed (combined) form;
Enamel aplasia.
Anatomy
The type of enamel defects in systemic hypoplasia depends on the stage of enamel development when the exposure to the etiological factor occurred.
Type of defects
Developmental defects of enamel
White lines, opaque white, cream, yellow, or brown spots
Amelogenesis imperfecta
Pits, grooves, depressions, or large areas of enamel aplasia
Matrix deposition abnormalities
3D animation: clinical types of systemic enamel hypoplasia
Despite the variability of clinical forms, common signs of systemic enamel hypoplasia can be identified:
Teeth erupt already defective;
Defects usually have a relatively regular shape and even borders;
Multiple teeth are affected: they have defects that are at the same level, in the same area of the crowns, and typically are of uniform size and shape;
A group of teeth from the same developmental period is affected; the defects are symmetrical;
Defects are parallel to the incisal edges or occlusal surfaces of teeth, more often on the labial/buccal surface and cusps.
Microstructural changes in hard tissues
In enamel structure, changes in the width and direction of enamel prisms are observed.
In the dentin structure of affected teeth at the border with enamel, the dentin tubules are curved and have a less regular arrangement; in some areas, narrowing and widening of their lumen is visible, and the hydroxyapatite crystals are arranged more randomly and loosely.
Increased formation of tertiary dentin by the pulp may also be observed.
Diagnosis of systemic enamel hypoplasia
Diagnostic test
Clinical presentation
Visual examination
Presence of localized color change of the enamel or its thickness
Probing
Painless, but may be painful if areas of enamel aplasia or associated decay process are present
Percussion on affected teeth
Painless
Temperature test
The response to a temperature stimulus disappears immediately, or a few seconds after the stimulus ceases
Local radiolucencies with clear contours are identified in the enamel area on the X-ray (if there is an enamel thickness defect)
Clinical manifestations
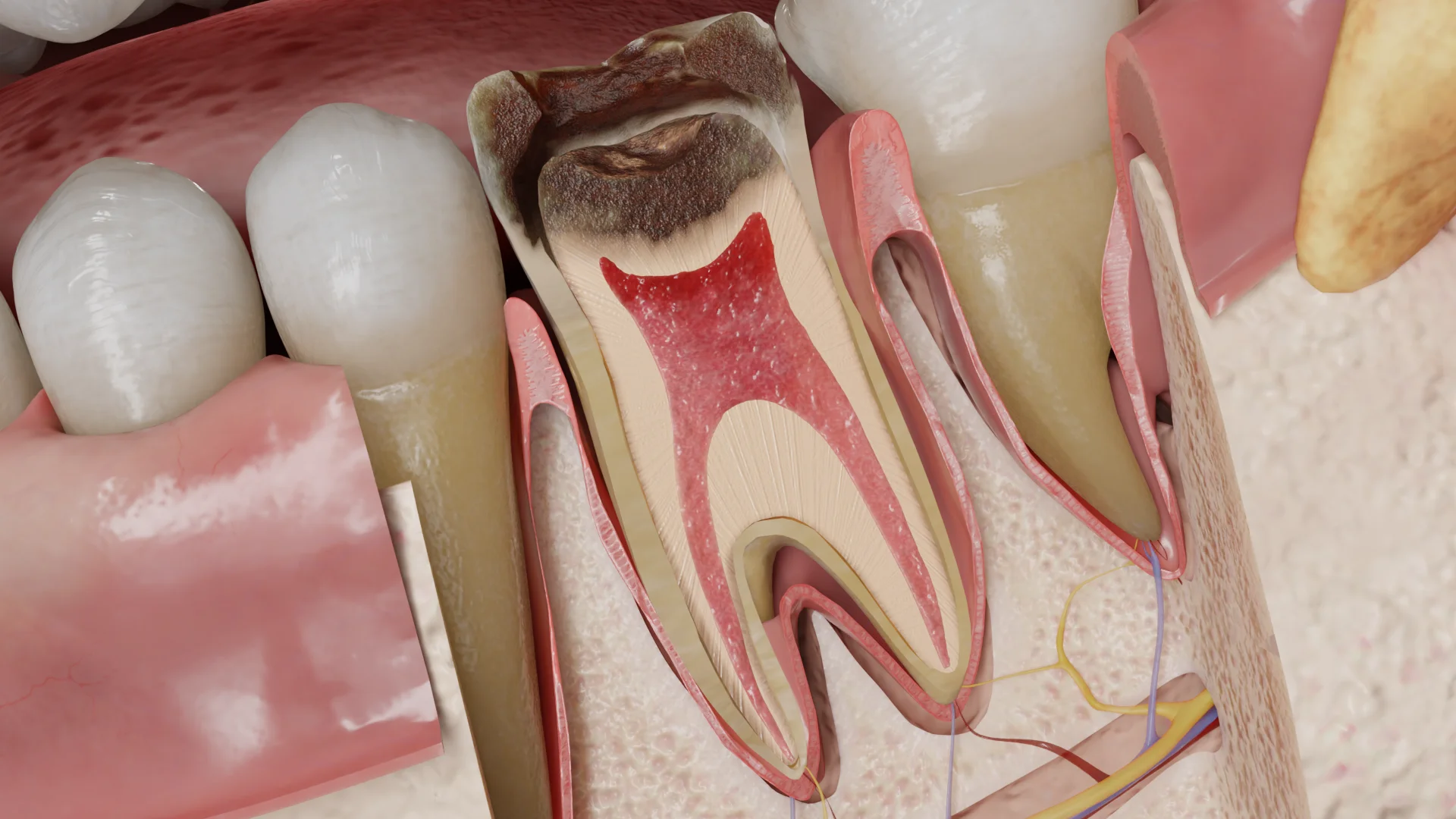
Spotted form
Spotted form of systemic enamel hypoplasia: 3D model
The patients can complain of a cosmetic imperfection. On the buccal surface of the teeth, in particular in the area of the cusps or incisal edge, spots are identified; they appear on an intact enamel and look milky-white, less often yellowish or brown, with clear boundaries and a smooth, glossy surface. The enamel in the affected area is of normal thickness. Over time, the spots do not change in size, shape, or color. The spots do not stain with methylene blue and are not detected on X-ray.
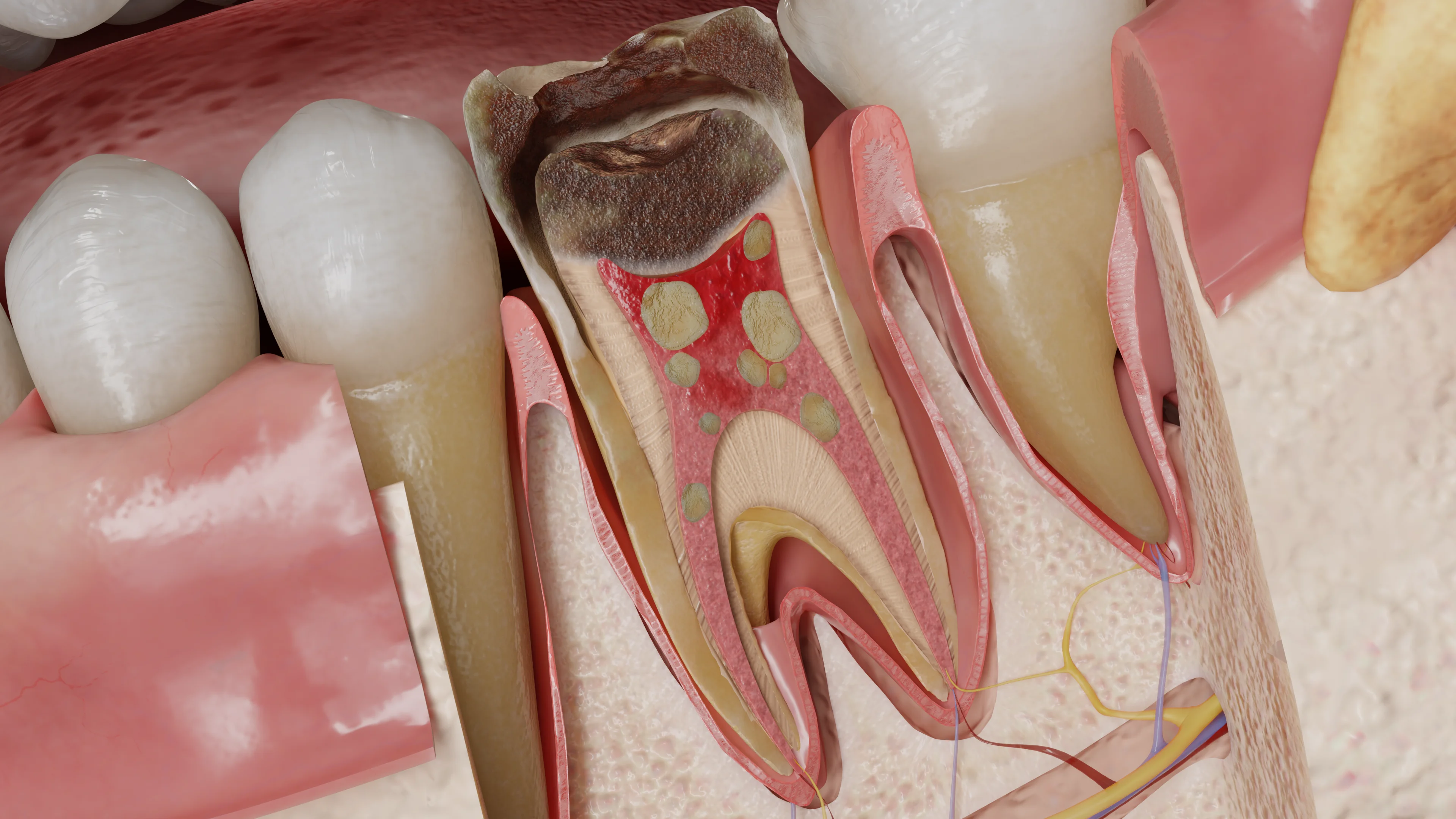
Erosive (pitting) form
Erosive (pitting) form of systemic enamel hypoplasia: 3D model
The patient may complain of a cosmetic defect or pain from chemical or thermal irritants (rarely).
On the enamel surface, depressions in the form of pits are identified, arranged horizontally and not connected with each other. The defects are usually round, with a smooth, dense bottom and shallow edges; the enamel is thinned in these areas. The pits are deeper on the labial/buccal surfaces of teeth and may be consistently stained with food pigments. Probing of the defects is painless.
Sometimes, the pitted form of systemic enamel hypoplasia can be associated with caries.
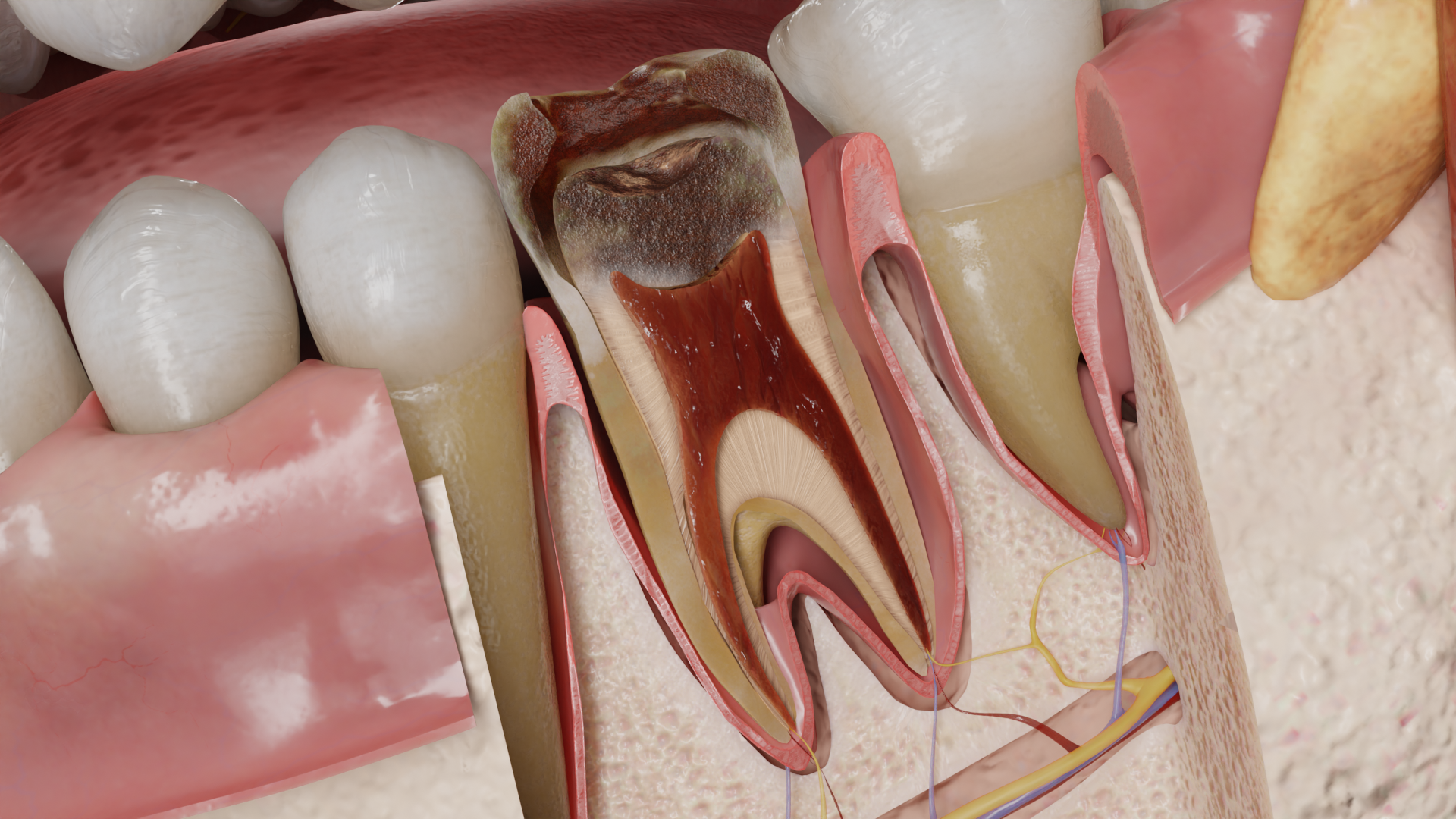
Furrowed form
Furrowed (linear) form of systemic enamel hypoplasia: 3D model
The patient complains of a cosmetic defect, sometimes of pain from mechanical, chemical, and thermal irritants, and of wear of the teeth.
Visually, depressions in the form of horizontal single or multiple grooves of varying depth and width can be seen on the teeth; the defects are located parallel to the incisal edge or occlusal surface.
At the bottom of the grooves, enamel is thinned or absent. When the enamel is partially preserved, the bottom of the defects is dense and smooth, with shallow edges. If the grooves affect the full thickness of the enamel, the bottom can be yellow or brown and have a rough surface, which may be painful when probed. If the groove is located on the incisal edge, it only has one wall, giving the impression that another, smaller tooth is “growing” from one tooth. In this case, premolars and molars exhibit underdeveloped cone-shaped cusps, devoid of enamel, which often chip due to mechanical stress. In the area of deep defects, caries may occur.
It’s a variant of the furrowed form of systemic enamel hypoplasia, where multiple thin horizontal grooves are visible on the tooth crown, partially merging with each other to form a wavy surface.
Cup-shaped form
Cup-shaped form of systemic enamel hypoplasia: 3D model
The patient may complain of a cosmetic defect, sometimes of pain from chemical or thermal irritants. The defects appear as cup-shaped depressions, oval or round, of varying size and depth.
The enamel at the bottom of the defects is thin or absent. If a thin layer of enamel is preserved, the edges, walls, and bottom of the defects are smooth, shallow, and dense, while in areas without enamel, the tissues are roughened and pigmented. If a cup-shaped defect is located in the area of the incisal edge of a front tooth, a semilunar notch forms on it. With defects on premolars and molars, their cusps are thinned and needle-like, prone to wear and chipping due to mechanical stress. Deep defects may also be affected by caries.
Mixed (combined) form
Mixed form of systemic enamel hypoplasia: 3D model
Depending on the severity of the defects, the patient complains of poor aesthetic appearance, pain from chemical and thermal irritants, tooth wear, and cusp chipping.
The mixed form of systemic enamel hypoplasia represents a combination of several defect forms on different teeth and even within a single tooth (combination/alternation of spots, pits, grooves, and cup-shaped depressions). Areas of deep defects, where enamel is completely absent, often fracture, chip, and wear away, and caries may also develop in these areas.
The patient complains of poor aesthetic appearance and pain from mechanical, thermal, and chemical irritants, as well as tooth wear and chipping. Enamel aplasia is a severe degree of enamel hypoplasia, characterized by local absence of enamel in certain areas or complete absence of enamel on the entire tooth crown.
Thinned areas of remaining enamel can wear over time, and caries may develop in areas of deep defects.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Treatment
Treatment of systemic enamel hypoplasia depends on the severity of the enamel lesions.
In the presence of lines and spots, remineralization, bleaching, and microabrasion techniques can be applied.
For increased tooth sensitivity, desensitizers are used as indicated.
In the presence of cavity defects, direct restoration with composite materials, glass ionomer cements (GIC), or compomer restorative materials is performed, and severely damaged hard dental tissues may be restored with esthetic veneers, overlays, or full crowns. It is important to note that patients with systemic enamel hypoplasia (except the spotted form) are more prone to develop caries and its complications.
In severe cases, when conservative methods are impossible, affected teeth are extracted with subsequent prosthetics.
FAQ
1. Can enamel be restored in hypoplasia with vitamins or pastes?
Unfortunately, no. Enamel defects in hypoplasia are irreversible because the enamel, unlike bone tissue, cannot regenerate (remodel). However, in the case of mild spotted forms, the appearance can be improved, and the enamel structure can be strengthened with remineralization, microabrasion, or whitening procedures. Deep defects require restoration with filling materials or crowns.
2. How to differentiate systemic hypoplasia from early caries?
There are several key differences that allow differentiating systemic hypoplasia from early caries. First, it is symmetry: in systemic hypoplasia, a group of teeth from the same developmental period is affected, and defects are symmetrically located on the same areas of homonymous teeth. Second, the time of appearance is important, as teeth erupt already defective, whereas caries develop only after eruption. The staining test is also informative: spots in hypoplasia do not stain with methylene blue (vital staining), unlike demineralization sites in early caries. Finally, differences are noticeable on the surface: in the spotted form of hypoplasia, it often remains smooth and shiny, whereas in caries it becomes matte and rough.
3. Can the condition of the teeth determine when exactly a defect developed in a child’s body?
The condition of the teeth allows fairly accurate determination of when exactly a defect developed in a child’s body since they function as a “biological archive.” The localization of the defect indicates the specific age at which the metabolic disorder occurred. Thus, defects in deciduous teeth indicate disorders during the intrauterine period. If the incisal edge of incisors and cusps of the first molars are affected, this indicates problems between 6 months and 1 year of age. Changes in the upper lateral incisors indicate a failure after the age of 1 year. If crown involvement is observed up to the gums, it indicates prolonged exposure to a negative factor up to 3-4 years of age.
4. Is hypoplasia associated only with the maternal medical conditions during pregnancy?
Hypoplasia is not exclusively associated with the maternal medical conditions during pregnancy, as its etiology is multifactorial. All provoking factors are divided into three main groups. Prenatal factors include maternal health conditions, toxicosis, and nutritional deficiencies. Neonatal factors include prematurity, with a risk of up to 60%, as well as birth injuries and Rh incompatibilities. Postnatal causes refer to the child’s health conditions in the first years of their life, such as acute infections, allergies, rickets, or the use of certain medications. Moreover, low socioeconomic status plays an important role, as it is often a marker of chronic resource deficiencies and malnutrition.
5. Why has the child developed horizontal grooves on their teeth?
This is the grooved form of hypoplasia. The number and depth of grooves indicate how often and how severely the child was ill (or had a metabolic disorder). The depth of the grooves indicates the intensity of the negative factor the tooth was exposed to. The number of grooves reflects the frequency of diseases: if the disease recurred, new grooves appear. Such defects require observation and often restoration, as enamel in deep grooves is thinned or absent, increasing the risk of caries.
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Moro C, Biehler-Gomez L, Attisano GL, Gibelli DM, Boschi F, De Angelis D, Cattaneo C. Investigating the etiology and demographic distribution of enamel hypoplasia. Heritage [Internet]. 2025 Oct 3;8(10):420.
Available from: https://doi.org/10.3390/heritage8100420
3.
Kühnisch J, Fresen KF. Prevalence of Enamel Hypomineralisation/Molar Incisor Hypomineralisation: A Scoping Review. Monographs in Oral Science [Internet]. 2024 Jan 1;32:100–116.
Available from: https://doi.org/10.1159/000538876
4.
Ammar N, Fresen KF, Schwendicke F, Kühnisch J. Epidemiological trends in enamel hypomineralisation and molar-incisor hypomineralisation: a systematic review and meta-analysis. Clinical Oral Investigations [Internet]. 2025 Jun 2;29(6):327.
Available from: https://doi.org/10.1007/s00784-025-06411-4
5.
Dehailan LA, Martinez-Mier EA. Evidence on the association of overall dietary factors, selected environmental, medical, demographic, and biological factors and developmental defects of enamel, including MIH and enamel fluorosis. Frontiers in Oral Health [Internet]. 2025 Dec 11;6:1616109.
Available from: https://doi.org/10.3389/froh.2025.1616109
6.
Sharma D, Ganesh M, Vellore KP, Kondamadugu S, Ali A, Bartarya T. Association of gestational age and birth weight with early childhood caries and developmental defects of enamel in children aged 3–6 years: A cross-sectional study. Journal of Indian Society of Pedodontics and Preventive Dentistry [Internet]. 2025 Oct 1;43(4):485–492.
Available from: https://doi.org/10.4103/jisppd.jisppd_342_25
7.
Palottil AS, Jeseem MT, Mohanan TVS, Sajitha PS. Prevalence of enamel defects in 12–15-year-old children visiting a tertiary care center – A cross-sectional study. Journal of Indian Society of Pedodontics and Preventive Dentistry [Internet]. 2025 Jul 1;43(3):334–338.
Available from: https://doi.org/10.4103/jisppd.jisppd_185_25
8.
Meena M, Aijazuddin A, Kumawat R, Saxena S, Rajput T, Jaidupally RR. Assessing the impact of diet on enamel hypoplasia in children. Journal of Pharmacy and Bioallied Sciences [Internet]. 2025 Jun 1;17(Suppl 2):S1972–S1974.
Available from: https://doi.org/10.4103/jpbs.jpbs_1818_24
9.
Neville B, Neville BW, Damm DD, Allen CM, Chi AC. Oral and maxillofacial pathology. Elsevier; 2023.
10.
Scully C, Flint S, Porter SR, Moos K, Bagan J. Oral and Maxillofacial Diseases, fourth edition. CRC Press; 2010.
11.
Regezi JA, Sciubba J, Jordan RCK. Oral pathology: Clinical Pathologic Correlations. Elsevier Health Sciences; 2016.
12.
Neville BW, Damm DD, Chi AC, Allen CM. Color Atlas of Oral and Maxillofacial Diseases. Elsevier; 2018.
13.
Prabhu SR. Handbook of Oral Pathology and Oral Medicine. John Wiley & Sons; 2021.
14.
Scully C, Welbury R, Flaitz C, De Almeida OP. Color Atlas of Orofacial Health and Disease in Children and Adolescents: Diagnosis and Management, Second Edition. CRC Press; 2001.
15.
Odell EW. Cawson’s Essentials of Oral Pathology and Oral Medicine. Churchill Livingstone; 2017.
16.
Laskaris G. Color Atlas of Oral Diseases in Children and Adolescents. Thieme; 1999.
17.
Ongole R, Praveen BN. Textbook of Oral Medicine, Oral Diagnosis and Oral Radiology. Elsevier India; 2012.
18.
Ghom AG, Ghom SA. Textbook of Oral Medicine. JP Medical Ltd; 2014.