Systemic Enamel Hypoplasia: Etiology, Classification, Clinical Presentation, and Treatment
Developmental Enamel Defects: Systemic Hypoplasia. Overview of the Etiology, Clinical Forms, Diagnosis, and Aesthetic Restoration Techniques for Teeth.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Periapical cyst is a pathologic cavity in the apex of the root of the tooth, with liquid contents and a lining of non-orogenic multilayered squamous epithelium, is a type of chronic apical periodontitis.

The cause of periapical cyst formation is microbial infection in the root canal system of the tooth. The main cells involved in the formation of this type of lesion are chronic inflammatory cells and epithelial cells of Malasse islets, which are remnants of the epithelium of the root sheath of Gertwig during tooth formation. These epithelial cells can be considered as unipotent stem cells.
During the inflammatory response, growth factors and cytokines are released in the tissues around the root tip, causing proliferation of epithelial cell islets of Malasse.
There are several theories for the formation of apical cysts.
As the epithelial islets grow, the central cells are removed from the source of nutrients and begin to undergo necrosis. Tissue decay products attract granulocytes and neutrophils to the necrosis zone, and microcavities form, which then merge to form a cystic cavity lined with multilayered squamous epithelium.
When an abscess forms in connective tissue, there is a proliferation of epithelial cells that cover the abscess cavity because they tend to fill open areas of connective tissue.
Epithelial tissue in the form of chaotically directed strands in the apical granuloma proliferates, epithelial strands unite to form a three-dimensional spherical structure of fibrovascular connective tissue, in which inflammatory cells are present; further, due to insufficient blood supply, it degenerates and a cyst cavity is formed. The cystic fluid is formed from the capillary network of the granuloma by transudation and exudation of the liquid part of the blood and as a result of the decay of the formal elements.
The cells of the epithelial lining of the cyst cavity are incapable of proliferation on their own without stimulation by cytokines and growth factors.
Cysts may slowly increase in size over time, probably due to degradation of the fibrous connective tissue capsule, matrix metalloproteinases, and resorption of surrounding bone. Inflammatory mediators and cytokines stimulate epithelial cell proliferation and also mediate bone resorption in foci of apical periodontitis. The epithelial cells of Malasse islets can also secrete factors that resorb bone tissue.
By affecting the surrounding structures, the cyst can push the roots of surrounding teeth, cause external resorption of tooth roots, push back and deform the wall of the maxillary sinus, or destroy it and penetrate directly into the sinus. In the absence of therapy periapical cysts can destroy a significant part of the adjacent bone tissue. In this case, the process may spread to the body and branch of the mandible, pathologic fracture of the mandible. Abscessing of the cyst may also occur over time.
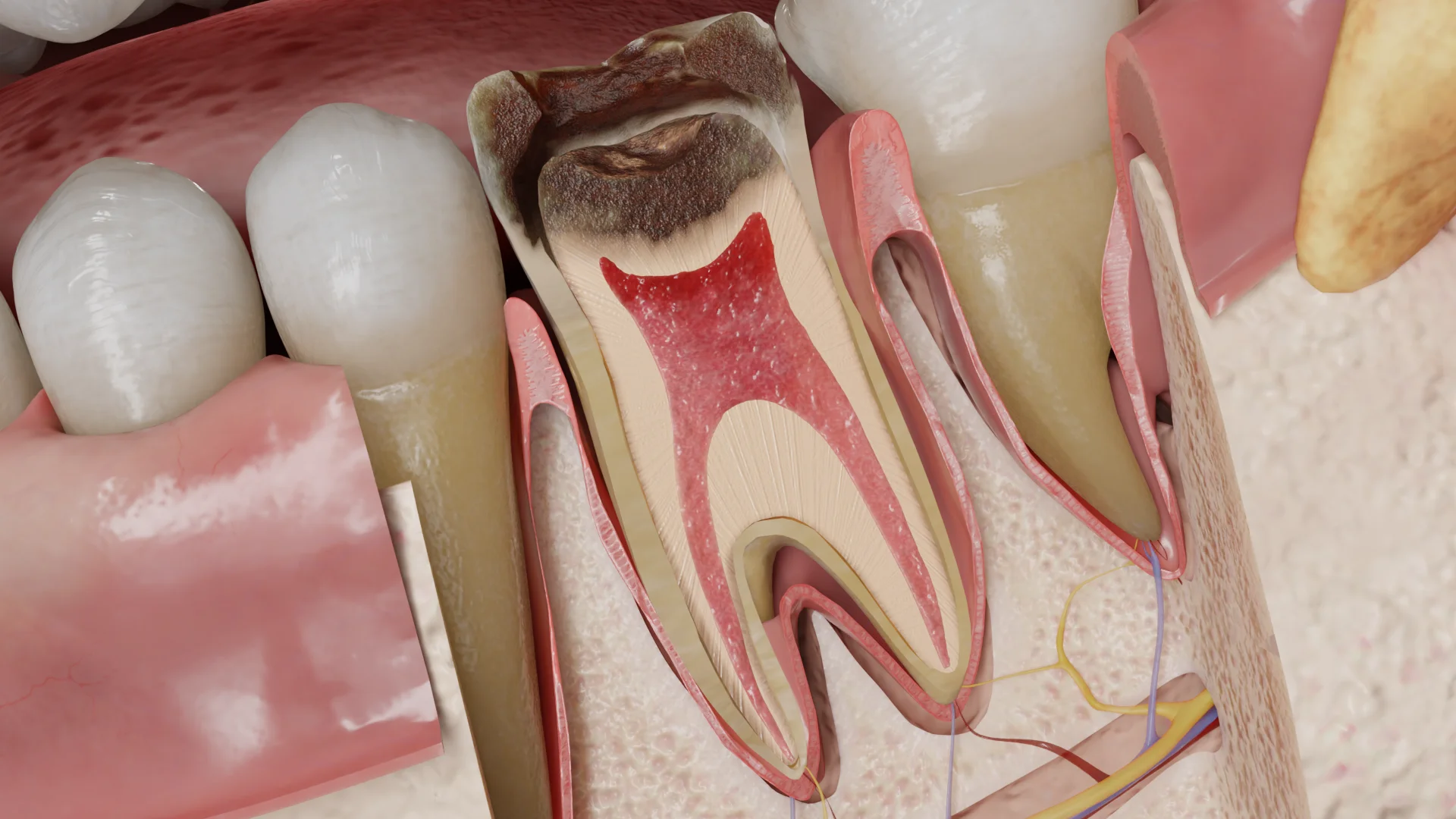
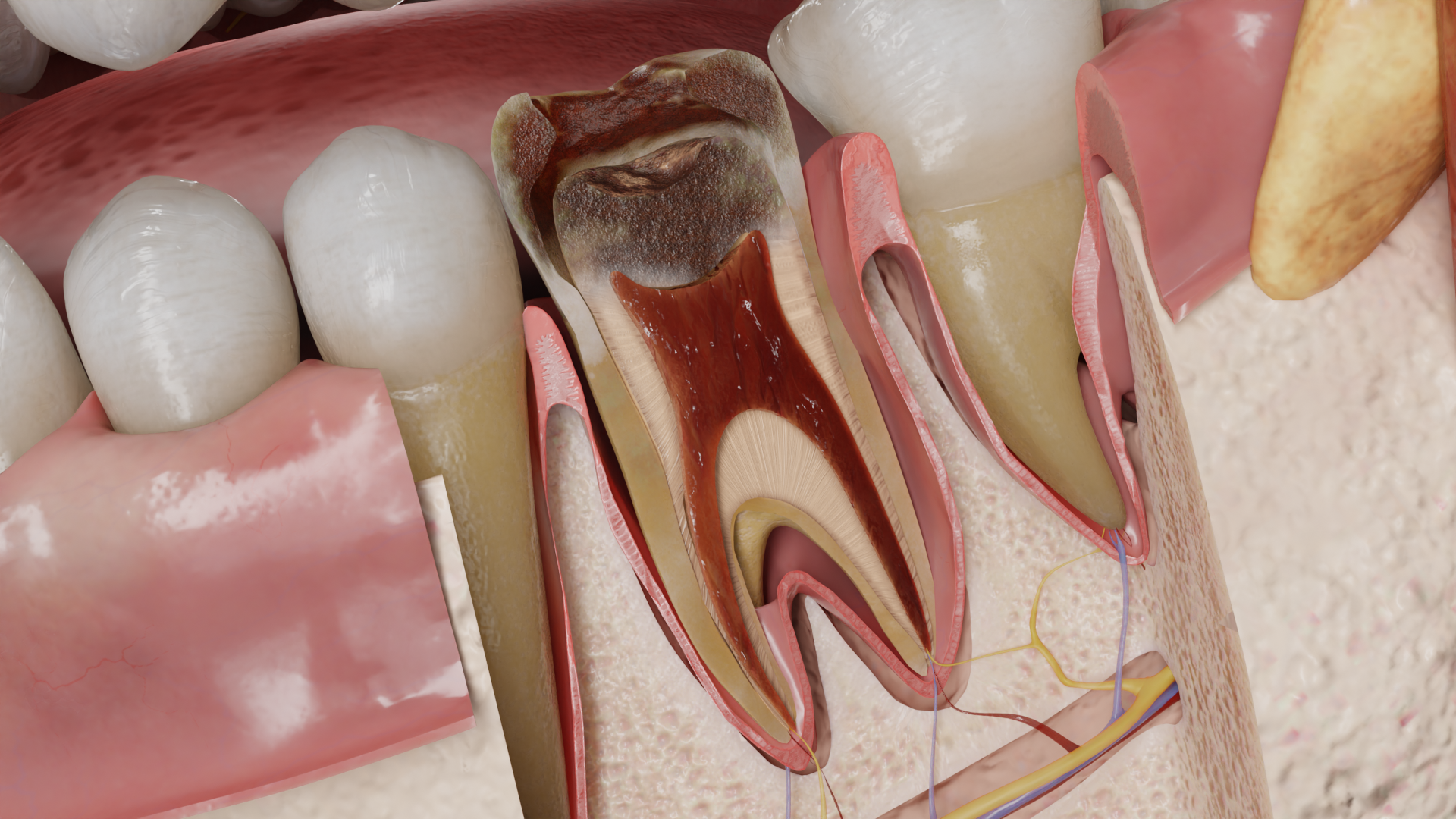
The affected tooth may be observed in the affected tooth:
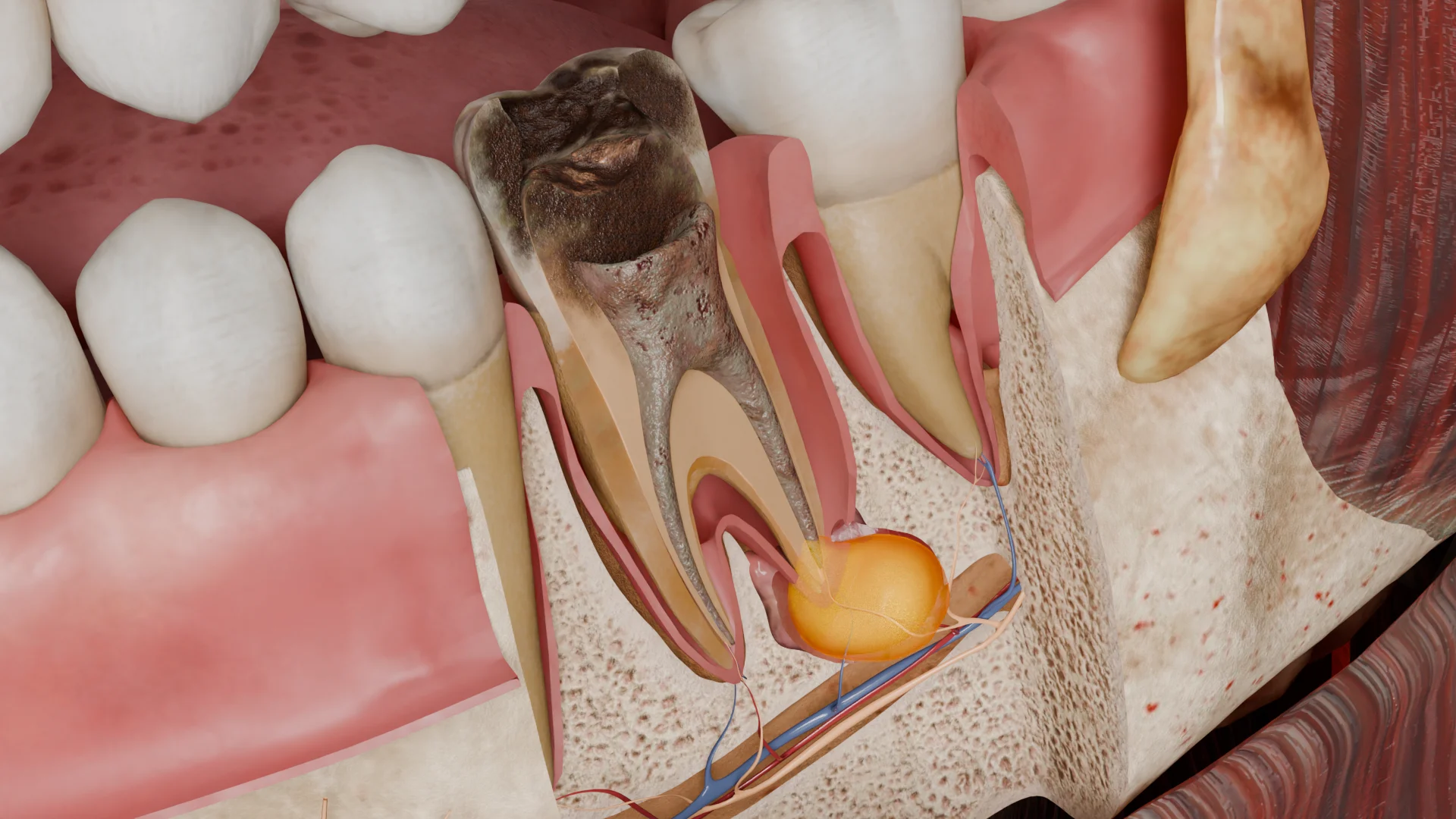
The pulp of the tooth is necrotic, yellowish-gray or gray-black in color. In the periapical area there is a focus of destruction of periodontal ligament and bone tissue. The periapical cyst itself is round or oval in shape, located in the area of the apex of the tooth root, and consists of the following elements:

To date, there are no non-invasive diagnostic tools available to accurately differentiate a granuloma from a cyst. The size of the lumen at the apex of the root on radiographs can be used only indirectly: if the size is between 10 and 20 mm, the probability of a cyst is up to 60%; if the size is more than 200 mm2, the probability is close to 100%. However, the final diagnosis is possible only after surgical biopsy or tooth extraction.
As a rule, the patient does not present any complaints. Most often cysts are an incidental finding on radiologic examination. The patient may complain of swelling on the lower or upper jaw, on the vestibular or palatal side. Visually in the tooth is determined deep carious cavity, restoration or traumatic defect, penetrating into the pulp chamber. Percussion of the tooth is painless, palpation of the transitional fold is also painless.
There may be a hemispherical jaw swelling, dense and painless on palpation, the mucous membrane in this area without visible pathologic changes. If the cortical plate in the area of the lesion is thinned, there may be bone crepitation in the area of the bulge when pressure is applied. If the cortical lamina of the jaw is destroyed, palpatory percussion of the causative tooth in the projection of the root apex may be felt. If the cyst is localized in the region of the maxillary incisors, the lower wall of the nasal cavity may swell (Gerber’s roll).
The causative tooth does not respond to temperature and electrical stimuli (an important diagnostic criterion in the presence of radiologic lucency in the periapical region of several teeth).
Find more scientifically accurate content on our social media








To date, there is no direct evidence whether periapical cyst regression can occur after nonsurgical endodontic treatment. Considering possible pathogenetic mechanisms, epithelial growth may cease after removal of a stimulating bacterial factor, such as after endodontic treatment. Subsequently, the epithelial lining may thin or disappear, creating conditions for healing.
Thus, the first stage is the endodontic treatment of the tooth: extirpation of non-viable pulp or removal of old filling material from the root canals, their instrumentation and drug treatment. In the course of instrumental treatment of the canals, intracanalicular puncture of the cyst is performed according to the indications. Subsequently, a hermetic obturation of root canals is performed with further restoration of the tooth.
In the presence of a large cyst (more than 3 cm), decompression may be performed according to the indications: reduction of the cyst size by surgical incision through the cyst wall and insertion of a drain, or extracanalicular aspiration and irrigation by puncturing the cyst with two large-diameter needles, aspiration of the contents and lavage with sterile saline solution.
In the future, if there is no healing of the periapical focus, enucleation of the cyst by periapical curettage, resection of the root apex with retrograde filling or amputation of the tooth root with simultaneous removal of the cyst shell is performed.
If the prognosis of endodontic treatment or periapical surgery is unsatisfactory, the tooth should be extracted.
1. What is a periapical cyst?
2. What are the symptoms of a periapical cyst?
3. How is a periapical cyst treated?
4. What is the danger of an untreated periapical cyst?
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Berman, L. H., & Hargreaves, K. M. (2020). Cohen’s Pathways of the Pulp Expert Consult. Elsevier.
3.
Torabinejad, M., Fouad, A., & Shabahang, S. (2020). Endodontics: Principles and Practice. Elsevier.
4.
American Association of Endodontists. (2019, June 3). Guide to Clinical Endodontics – American Association of Endodontists.
https://www.aae.org/specialty/clinical-resources/guide-clinical-endodontics/
5.
Ricucci, D., & Siqueira, J. F. (2013). Endodontology: An Integrated Biological and Clinical View. Quintessence Publishing (IL).
6.
Bergenholtz, G., Hørsted-Bindslev, P., & Reit, C. (2013). Textbook of Endodontology. John Wiley & Sons.
7.
Hülsmann, M., Schäfer, E., Bargholz, C., & Barthel, C. (2009). Problems in endodontics: Etiology, Diagnosis and Treatment. Quintessence Publishing (IL).
8.
Beer, R., Baumann, M. A., & Kielbassa, A. M. (2004). Taschenatlas der Endodontie.
9.
Petersson, A., Axelsson, S., Davidson, T., Frisk, F., Hakeberg, M., Kvist, T., Norlund, A., Mejàre, I., Portenier, I., Sandberg, H., Tranæus, S., & Bergenholtz, G. (2012). Radiological diagnosis of periapical bone tissue lesions in endodontics: a systematic review. International Endodontic Journal, 45(9), 783-801.
https://doi.org/10.1111/j.1365-2591.2012.02034.x
Loading test 6 questions




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io