Systemic Enamel Hypoplasia: Etiology, Classification, Clinical Presentation, and Treatment
Developmental Enamel Defects: Systemic Hypoplasia. Overview of the Etiology, Clinical Forms, Diagnosis, and Aesthetic Restoration Techniques for Teeth.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hematology
Hematopoiesis and blood-related disorders
Hepatology
Liver, gallbladder, and biliary tract diseases
Histology
Microscopic tissue and cell structures
Infectious diseases
Bacterial, viral, and parasitic infections
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Orthopedics
Bone, joint, and soft tissue disorders
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hematology
Hematopoiesis and blood-related disorders
Hepatology
Liver, gallbladder, and biliary tract diseases
Histology
Microscopic tissue and cell structures
Infectious diseases
Bacterial, viral, and parasitic infections
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Orthopedics
Bone, joint, and soft tissue disorders
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Pathological changes of the dental pulp represent a group of conditions characterized by structural and functional disruption of the dental pulp. These include hyperplasia (pulp polyp), necrosis (pulp death), and calcification (formation of pulp stones). Each of these conditions requires specific diagnostic and therapeutic approaches to prevent complications and preserve the tooth.
Pulp hyperplasia (synonyms: hyperplastic pulpitis, pulp polyp) is a form of irreversible pulpitis resulting from the chronic inflammatory growth of the pulp through the carious cavity to the tooth surface.
More commonly found in young patients. The precondition is the complete carious destruction of the roof of the pulp chamber. With such severe crown destruction, the pulp is exposed and subject to constant mechanical irritation and infection.
As a result, proliferation of connective tissue occurs, with its growth forming a richly vascularized polyp on a wide peduncle. Upon contact with gingival tissues, the pulp polyp may undergo epithelialization.
In the affected tooth, a deep carious cavity widely communicating with the pulp chamber is detected. The overgrown dental pulp protrudes from the carious cavity as a red-pink connective tissue growth resembling cauliflower.
Histologically, two types of pulp polyps are distinguished:
The size of the pulp polyps varies: it may slightly rise above the level of the pulp chamber’s roof or sometimes fill the entire carious cavity and protrude above the occlusal surface of the tooth.

The following methods are used for diagnosis:
However, due to the spread of microorganisms and their metabolic products, toxins, or enzymes from the pulp tissue into the periapical space, there may be an expansion of the periodontal ligament space, violation of the integrity of the cortical plate, a radiolucent periapical lesion, or condensing osteitis.
Hyperplastic pulpitis is usually asymptomatic. The patient’s history may reveal that the tooth was once painful, but then the pain disappeared, leaving only slight tenderness and bleeding from the carious cavity during meals. There may also be complaints of prolonged pain from thermal stimuli.
During oral cavity examination, a large carious cavity is revealed filled with a fleshy tumor-like formation resembling “cauliflower”. In some cases, the tissue is red-pink, dense, covered with epithelium, and comparatively insensitive to palpation; in others, it is bright red, bleeding upon the slightest touch.
Probing at the base of the cavity reveals a wide peduncle connecting the formation to the underlying pulp tissues. The overgrown tissue is insensitive to superficial probing, while deep probing at the root canal openings is painful.
Endodontic treatment is performed (complete pulp removal, mechanical and chemical treatment of the root canals, and their airtight obturation with subsequent tooth restoration).
In primary teeth and permanent teeth with undeveloped roots, if indicated, the method of pulpotomy may be used (partial pulp removal preserving the tooth’s vitality).
If the prognosis of endodontic treatment is unsatisfactory, the tooth should be extracted.
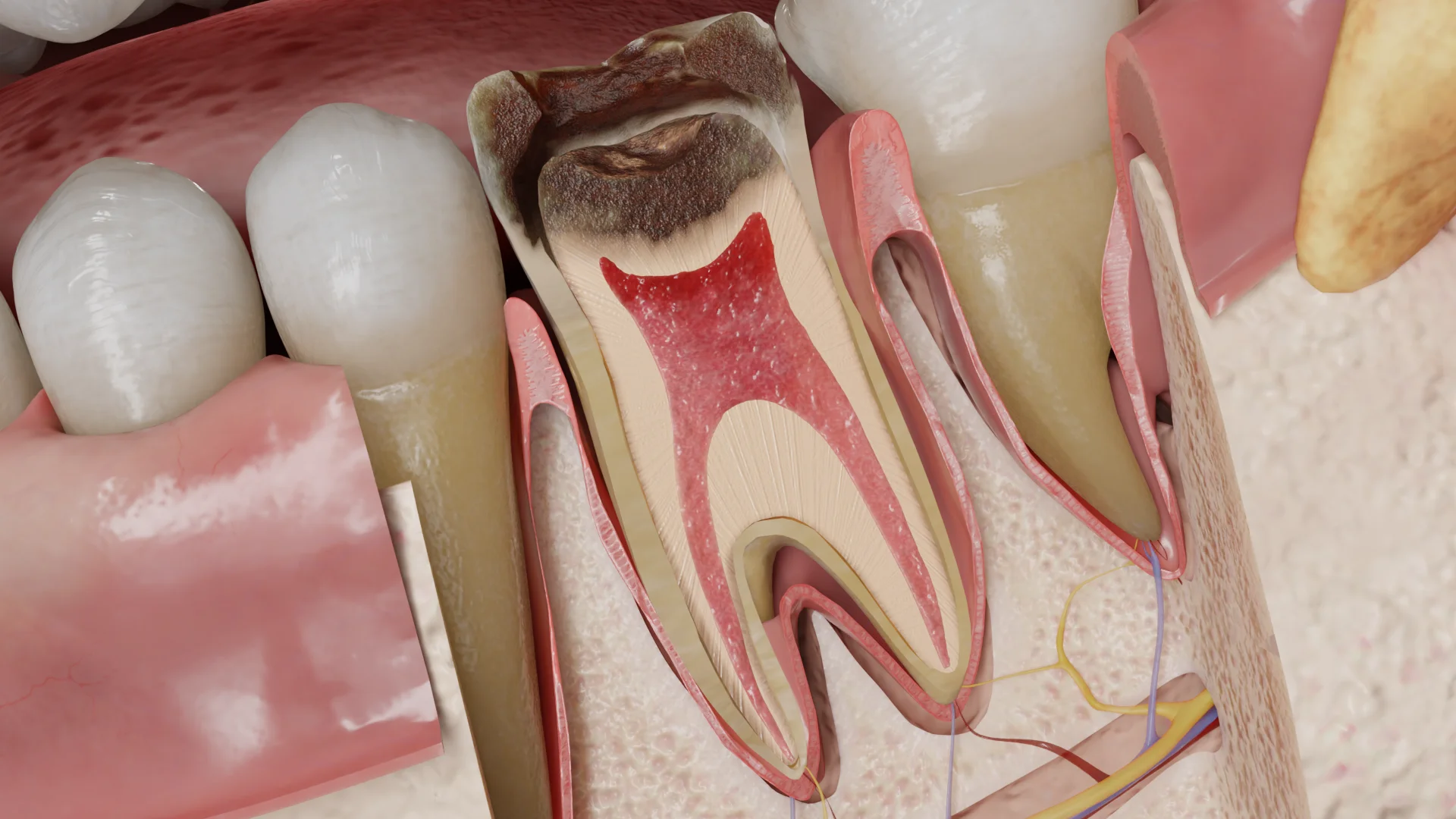
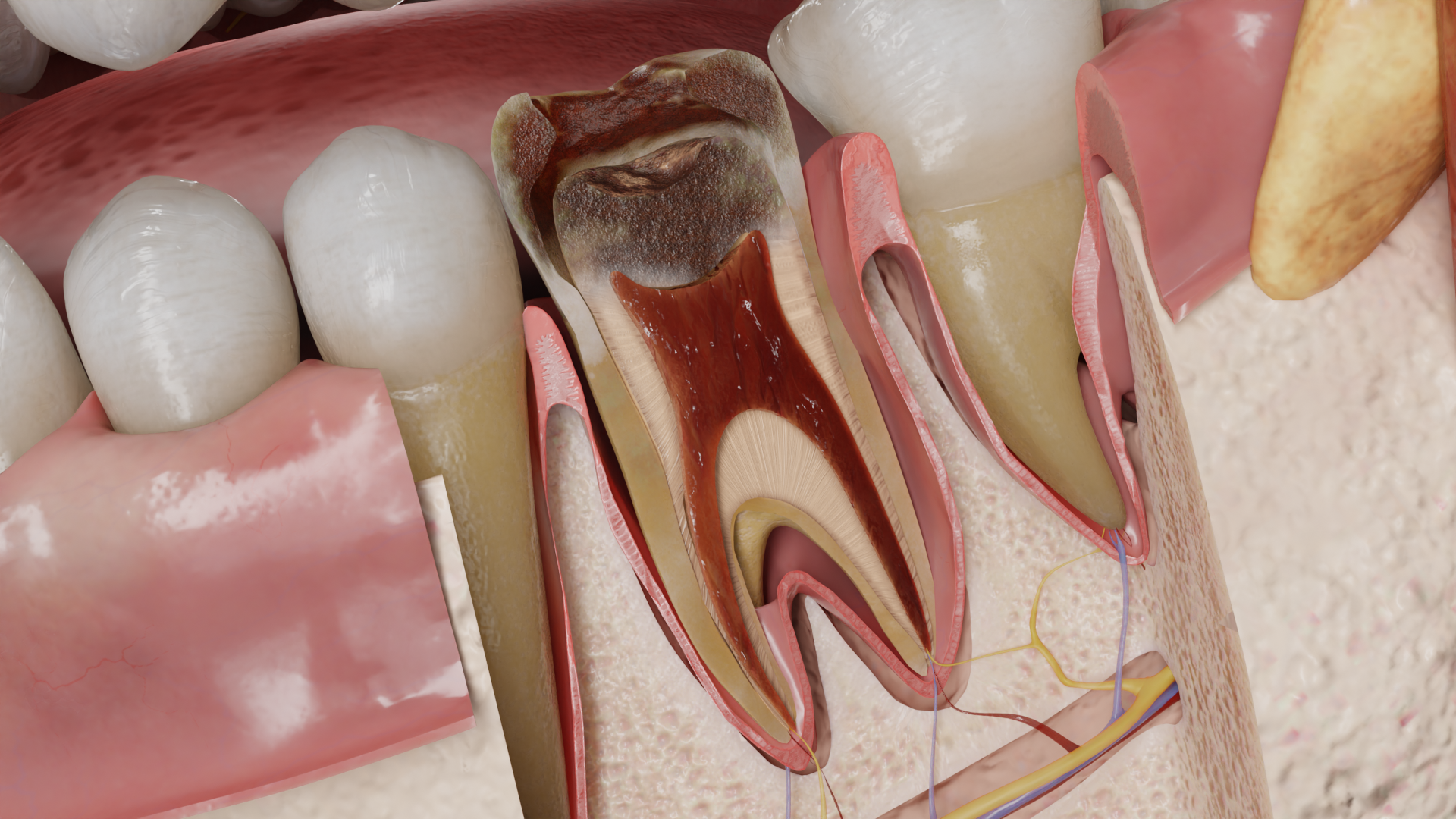
Pulp necrosis is an irreversible condition characterized by the death of the dental pulp.
Pulp necrosis may be partial or complete.
Factors contributing to pulp necrosis
| Group of factors | Description |
|---|---|
| Infectious | Penetration of bacterial infection into the dental pulp (outcome of irreversible pulpitis) |
| Mechanical | Acute and chronic dental injury |
| Thermal | Overheating of the pulp, for example, during the preparation of a tooth for prosthetic structures without air-water cooling |
| Chemical | Toxic damage to the pulp with the use of devitalizing pastes, toxic liners and filling materials, or during the treatment of the carious cavity with aggressive liquids |
| Dental congenital abnormalities | Dental evagination (dens evaginatus), dental invagination, “tooth within a tooth” (dens invaginatus, dens in dente) |
Penetration of microflora into the pulp in irreversible pulpitis leads to colliquative (wet) necrosis. During the exudative stage, tissue edema increases, and processes of tissue hypoxia, anaerobic glycolysis, and acidosis are exacerbated. Purulent exudate contains enzymes released from lysosomes of disintegrating neutrophils. These enzymes cause tissue liquefaction of the pulp, increase vascular permeability, promote the formation of chemotactic substances, and enhance phagocytosis. The resultant tissue destruction zone slowly spreads deeper in the apical direction.
If there is an exudate outflow through the carious cavity, pulp necrosis may slow down, and the root pulp can remain vital for an extended period. In a closed pulp chamber, rapid and total pulp necrosis occurs.
Disruption of pulp blood supply due to acute or chronic tooth trauma causes ischemia and hypoxia in the pulp. Oxidative phosphorylation, intercellular, and transcellular transport processes cease, leading to cytoskeleton and cellular membrane collapse, resulting in coagulative (dry) tissue necrosis.
In pulp necrosis, blood supply within the pulp is absent, and nerve endings cease to function. After total pulp necrosis, the tooth becomes asymptomatic until the pathological process extends into periapical tissues.
However, exposure to a thermal irritant can produce a dull pain, linked to residual fluid or gas in the pulp space expanding and spreading into periodontal tissue.
Moreover, in partial pulp necrosis in multirooted teeth, pulp testing in one root may show no response, while another may give a positive response, complicating diagnosis.
Depending on the etiologic factor, the affected tooth may exhibit:
In colliquative necrosis, the pulp is moist, gray-black, and has an unpleasant putrid odor. In coagulative necrosis, the pulp is dry, dense, and yellowish-gray in color.

| Method | Clinical presentation |
|---|---|
| Collection of complaints and history | The presence, nature, and location of pain, recent dental treatment, injury |
| Visual examination | The dental crown may appear grayish due to the penetration of pulp breakdown products into the dentin tubules |
| Tooth percussion | Painless |
| Palpation along the transitional fold | Painless |
| Temperature test | No reaction to a cold stimulus. The thermal test may be positive in partial pulp necrosis in multirooted teeth. The tooth may react to a hot stimulus with a dull pain |
| Electrical pulp testing | The pulp does not react to an electric current; threshold sensitivity at high (greater than 100 µA) current strength is associated with a response from periodontal tissues |
| Bite test | Usually negative, positive on one of the cusps if there is a tooth fracture |
| Radiography (intraoral contact radiography, radiovisiography, orthopantomography, cone beam computed tomography) | A carious cavity, restoration, or traumatic defect adjacent to/penetrating the pulp chamber, usually without changes in the periapical region. Widening of the periodontal ligament space may occur due to the infiltration of toxins into the periapical tissues |
| Diagnostic preparation | This method is applied only when other methods cannot be used or their results are ambiguous. The tooth is prepared without anesthesia using a small-sized bur, assessing the presence/absence of pain sensations |
Pulp necrosis is usually asymptomatic. The history may reveal that the tooth previously ached, then the pain subsided after a while.
The patient may complain of tooth discoloration, a foul odor emanating from the tooth, or prolonged pain from heat. In the presence of a cracked tooth or when the inflammatory process spreads to periapical tissues, the patient may also complain of pain while chewing.
Endodontic treatment of the tooth is conducted: complete removal of the destroyed pulp, mechanical and chemical treatment of the root canals, and their airtight obturation with subsequent tooth restoration.
If the prognosis of endodontic treatment is unsatisfactory, the tooth should be extracted.
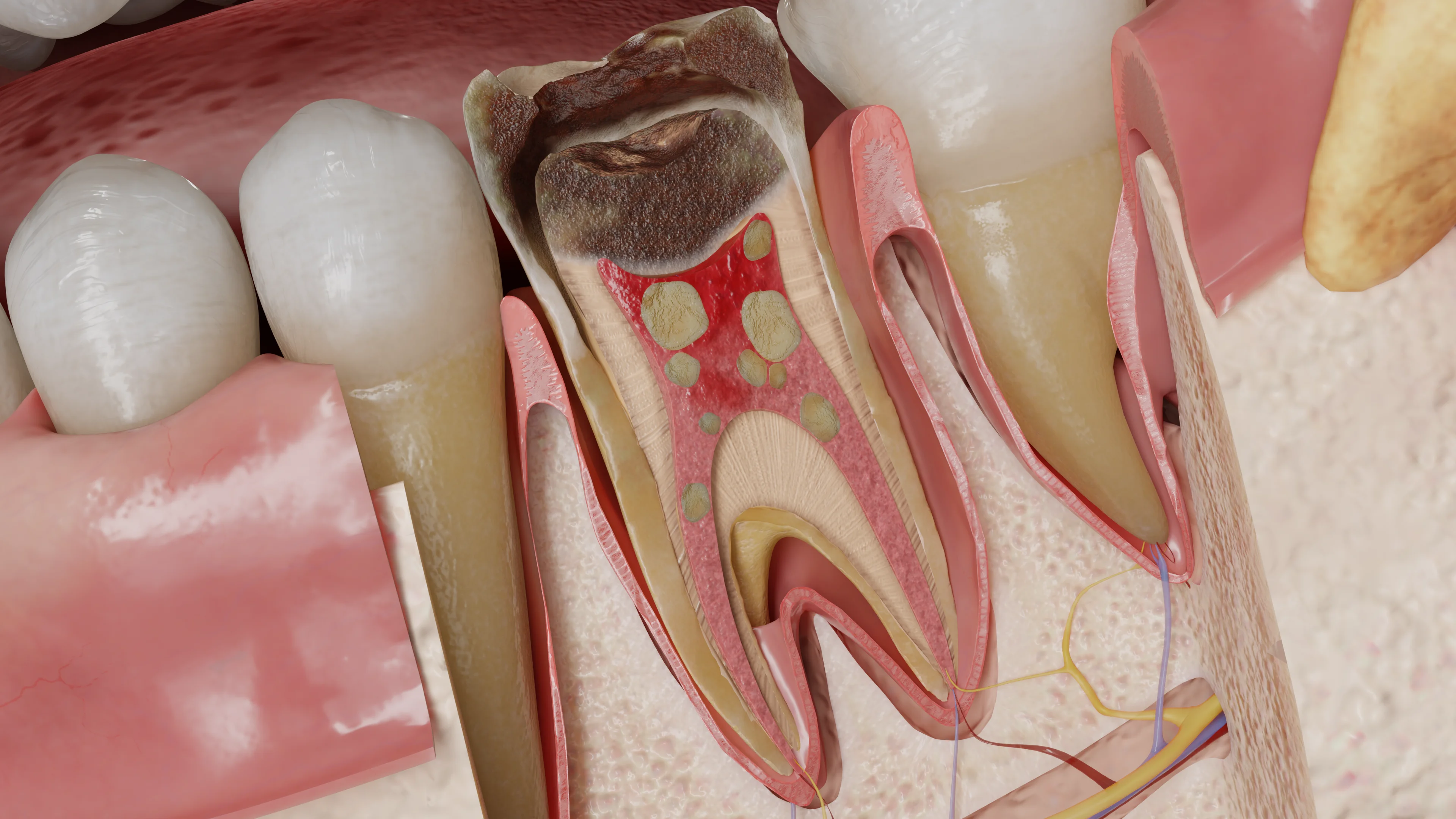
Pulp calcification (synonyms: pulp stones, denticles) refers to abnormal hard tissue formations within the pulp.
To date, the exact cause of pulp calcification is unknown. Possible etiological factors include:
Calcifications may form around foci of necrotized cells, clots in blood vessels, collagen fiber bundles, or epithelial cells. Tissue or blood vessel death, around which denticles then form, may result from external factors (microflora during a carious process, temperature fluctuations, mechanical impacts, toxins). Calcium phosphate crystals can be deposited directly in cells.
The connective tissue of the pulp, exhibiting a form of protective action, delineates necrotized tissue from vital tissue by encapsulation in fibrodentin. Diffuse calcifications in root canals are primarily deposited along collagen fibers or blood vessels.
So-called true denticles, having a dentin-like structure with tubules, are rarely found and form as a result of the disruption of remnants of Hertwig’s epithelial root sheath, with odontoblasts arranged concentrically around.
Without visible tissue damage, the cause of pulp calcification remains unknown. Calcifications often appear in an apparently healthy pulp, indicating that functional stress is not a requisite for denticle formation.
Teeth affected by caries exhibit significant mineralization enhancement compared to intact teeth. As the carious process progresses, the number and prevalence of pulp stones increase. Under chronic irritation of odontoblasts by bacterial toxins, the pulp responds by depositing secondary dentin, forming a barrier to the carious process. Reduction of the pulp chamber resulting from hard tissue formation by cells of the vital pulp can lead to complete obliteration of its lumen.
Mechanical or occlusal injury to the teeth may lead to calcifying metamorphosis—a condition of partial or complete radiologic obliteration of the tooth cavity and root canals. The mechanisms of this reaction are not fully understood, yet it is proposed that odontoblasts and possibly other mesenchymal cell populations within the pulp may lose autonomous regulatory control during neurovascular damage and regeneration, causing disorganized hard tissue deposition.
Injury of teeth with incomplete root formation causes rupture of incoming blood vessels, leading in turn to pulp infarction. A wide apical foramen allows periodontal connective tissue to proliferate and replace infarcted areas, carrying cells capable of differentiating into either cementoblasts or osteoblasts.
Pulp calcifications can be observed in multiple teeth. Calcifications revealed in all teeth suggest their genetic nature.
The presence of pulp calcifications decreases the number of its cells. This reduces the pulp’s regenerative capacity. Moreover, intensive mineralizations in the tooth cavity and root canals can complicate access and treatment of a root canal.
A tooth with pulp calcification might be intact, have a carious cavity, or show signs of pathological attrition, injury, erosion, an abfraction defect, or a restoration. Denticles can be localized in the coronal and/or root pulp at the openings of root canals.
The following types are distinguished:
In relation to the wall of the pulp chamber:
In the pulp’s coronal part, isolated concentric pulp stones are usually observed, whereas in the root pulp, calcification tends to spread diffusely. The size of denticles varies from microscopic particles often associated with arteriole walls to proliferations occupying the entire pulp chamber.
| Method | Result in pulp calcification |
|---|---|
| Tooth percussion | Painless |
| Palpation along the transitional fold | Painless |
| Thermal test and electric pulp testing | The sensitivity threshold to thermal and electrical stimuli may increase, and with marked obliteration, the sensitivity test loses its informativeness |
| Radiography (intraoral contact radiography, radiovisiography, orthopantomography, cone beam computed tomography) | Single or multiple darkening in the pulp chamber, with complete obliteration — absence of the pulp chamber and root canal lumen. Complete obliteration cannot be diagnosed solely radiographically and must always have clinical confirmation, as even if the root canal lumen is not visualized, it may be patent for endodontic instruments |
Pulp calcification can be asymptomatic and is often detected incidentally during radiologic examination. With marked obliteration of the pulp chamber, the tooth’s crown may appear more yellowish compared to adjacent teeth.
Find more scientifically accurate content on our social media








Pulp calcification as such does not require treatment. Elimination of possible provoking factors is carried out (treatment of caries and non-carious lesions, selective occlusal grinding in occlusal injury, replacement of inadequate restorations, or adjustment of orthodontic forces).
Endodontic treatment is performed if signs of irreversible pulpitis or apical periodontitis are present according to indications.
1. Can pulp hyperplasia be left untreated if it doesn’t hurt?
2. Why does a tooth sometimes react to heat in pulp necrosis?
3. Can pulp necrosis always be detected on an X-ray?
4. Can pulp stones cause pain?
5. Should pulp stones be removed before root canal treatment?
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Berman LH. H, Hargreaves KM. Cohen’s Pathways of the Pulp. Elsevier; 2020.
3.
Suresh K, Bajaj N, Nayak A, Chapi DmK, Patil S, Rani A. Pulp polyp – A periapical lesion: Radiographic observational study. Journal of Indian Academy of Oral Medicine and Radiology [Internet]. 2015 Jan 1;27(1):68.
Available from: https://doi.org/10.4103/0972-1363.167085
4.
Torabinejad M, Fouad A, Shabahang S. Endodontics: Principles and Practice. Elsevier; 2020.
5.
American Association of Endodontists. Guide to Clinical Endodontics – American Association of Endodontists [Internet]. American Association of Endodontists. 2019.
Available from: https://www.aae.org/specialty/clinical-resources/guide-clinical-endodontics/
6.
Ricucci D, Siqueira JF. Endodontology: An Integrated Biological and Clinical View. Quintessence Publishing (IL); 2013.
7.
Bergenholtz G, Hørsted-Bindslev P, Reit C. Textbook of Endodontology. John Wiley & Sons; 2013.
8.
Hülsmann M, Schäfer E, Bargholz C, Barthel C. Problems in endodontics: Etiology, Diagnosis and Treatment. Quintessence Publishing (IL); 2009.
9.
Beer R, Baumann MA, Kielbassa AM. Pocket Atlas of Endodontics. 2006.
10.
Smaïl-Faugeron V, Glenny AM, Courson F, Durieux P, Muller-Bolla M, Chabouis HF. Pulp treatment for extensive decay in primary teeth. Cochrane Database of Systematic Reviews [Internet]. 2018 May 31;2018(5).
Available from: https://doi.org/10.1002/14651858.cd003220.pub3
11.
Mando A, Laflouf M, Tolibah YA. The Management of Hyperplastic Pulpitis in Immature Permanent Molar Using Vital Pulp Therapy: A Case Report with 12 Months Follow-Up. Case Reports in Dentistry [Internet]. 2024 Jan 1;2024(1):5280168.
Available from: https://doi.org/10.1155/2024/5280168
12.
Abdulwahab MA, Alqahtani MS, Alshammari AA, Jiffri SE, Alasim AM, Alsharidah FM, Alqunfuthi NI, Alnamnakani BA, Alshahrani RS, Alshahrani NA, Aljohani RN, Almintakh MAL. Etiologies, risk factors and outcomes of dental pulp necrosis. International Journal of Community Medicine and Public Health [Internet]. 2021 Dec 5;9(1):348.
Available from: https://doi.org/10.18203/2394-6040.ijcmph20214793
13.
Flanagan TA. What can cause the pulps of immature, permanent teeth with open apices to become necrotic and what treatment options are available for these teeth. Australian Endodontic Journal [Internet]. 2014 Dec 1;40(3):95–100.
Available from: https://doi.org/10.1111/aej.12087
14.
Loya PR, Nikhade PP. Correlation of pulp calcification and cardiovascular Conditions: A literature review. Cureus [Internet]. 2023 Oct 18;15(10):e47258.
Available from: https://doi.org/10.7759/cureus.47258
15.
Farias Z, Sousa J, Faria C, Vieira J, Sobral A, Silveira M. Pulpal calcifications in orthodontically moved teeth: Scoping review. Journal of Clinical and Experimental Dentistry [Internet]. 2023 Jan 1;15(9):e773–e780.
Available from: https://doi.org/10.4317/jced.60777
Loading test 6 questions
Table of Contents




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io