Systemic Enamel Hypoplasia: Etiology, Classification, Clinical Presentation, and Treatment
Developmental Enamel Defects: Systemic Hypoplasia. Overview of the Etiology, Clinical Forms, Diagnosis, and Aesthetic Restoration Techniques for Teeth.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
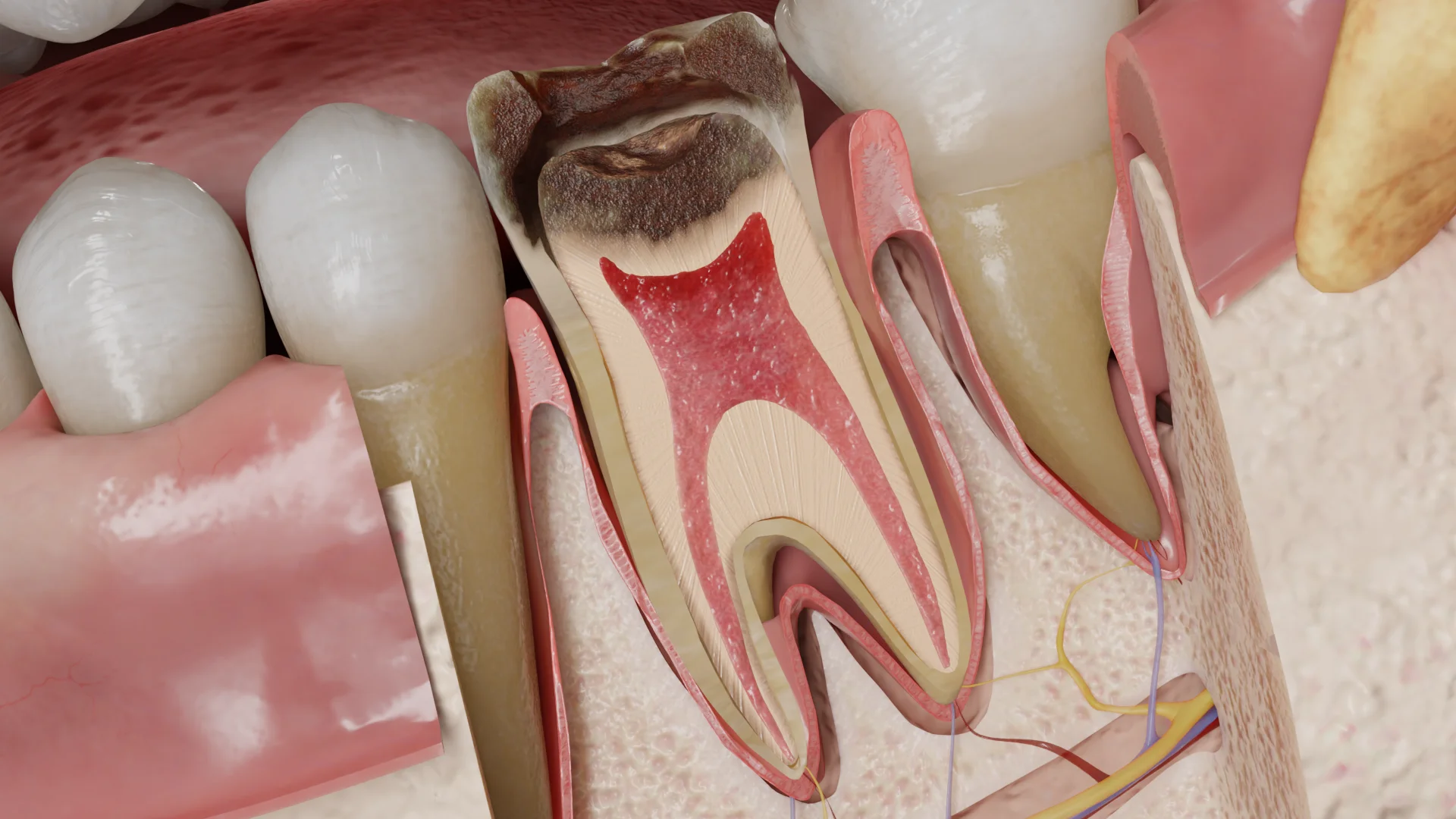
Irreversible pulpitis is an inflammation of the dental pulp that does not disappear when its cause is eliminated.
The main cause of pulpitis development is the penetration of the carious process into the pulp. It can also be caused by tooth trauma (mechanical injury, occlusal trauma, orthodontic tooth movement), iatrogenic factors (preparation without cooling, poor isolation of the working field, accidental pulp exposure, use of toxic lining and restorative materials).
During microbial invasion of the pulp, inflammatory defense mechanisms are activated, neutrophils accumulate, and immune cells gather. Neutrophils migrate from the pulp to the adjacent openings of dentinal tubules and release oxygen radicals, lysosomal enzymes, and nitric oxide, contributing to tissue destruction. The release of pro-inflammatory neuropeptides causes vasodilation and increased permeability of vessel walls. This leads to fluid exiting from the vessel lumen into the tissues.
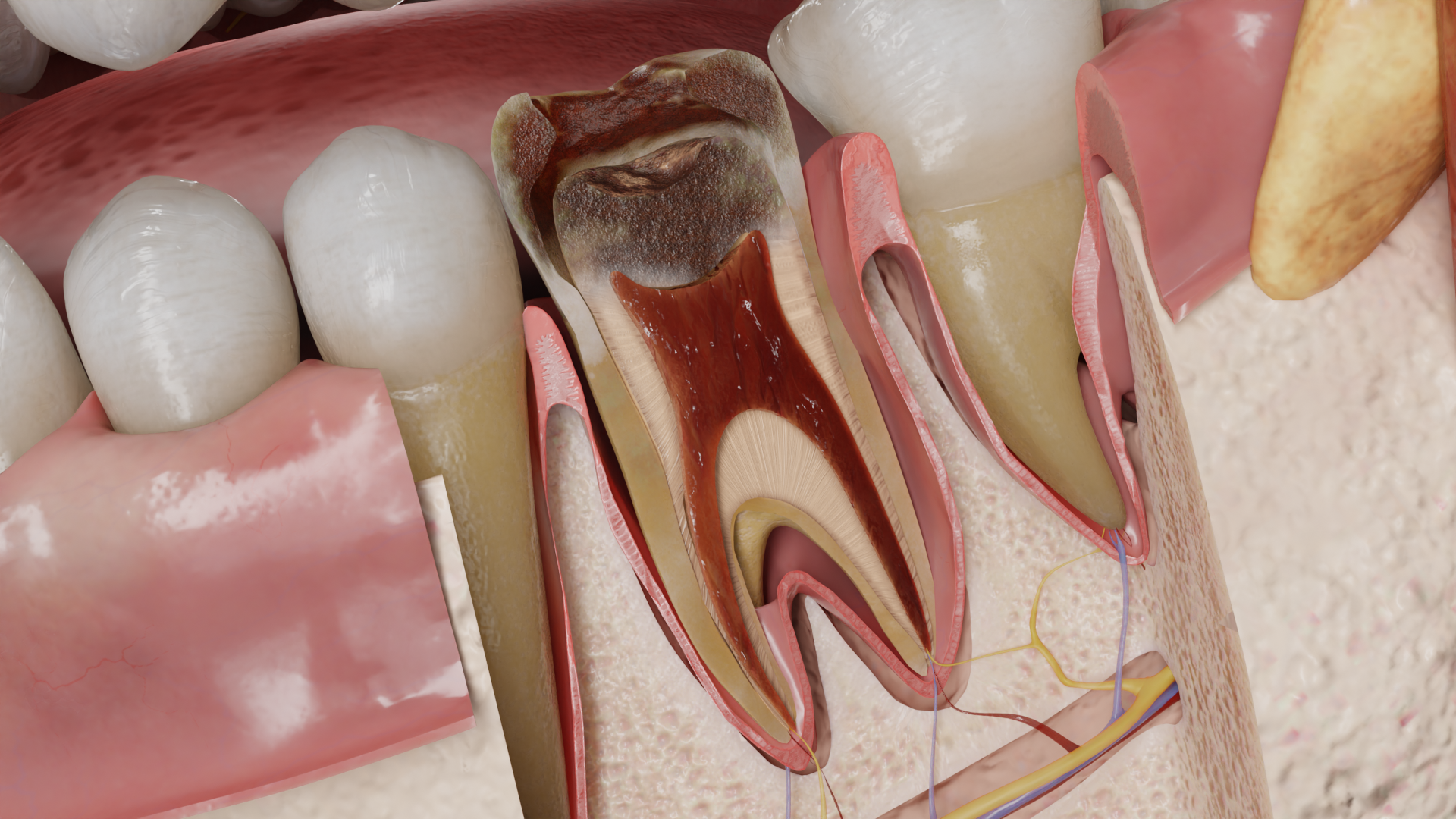
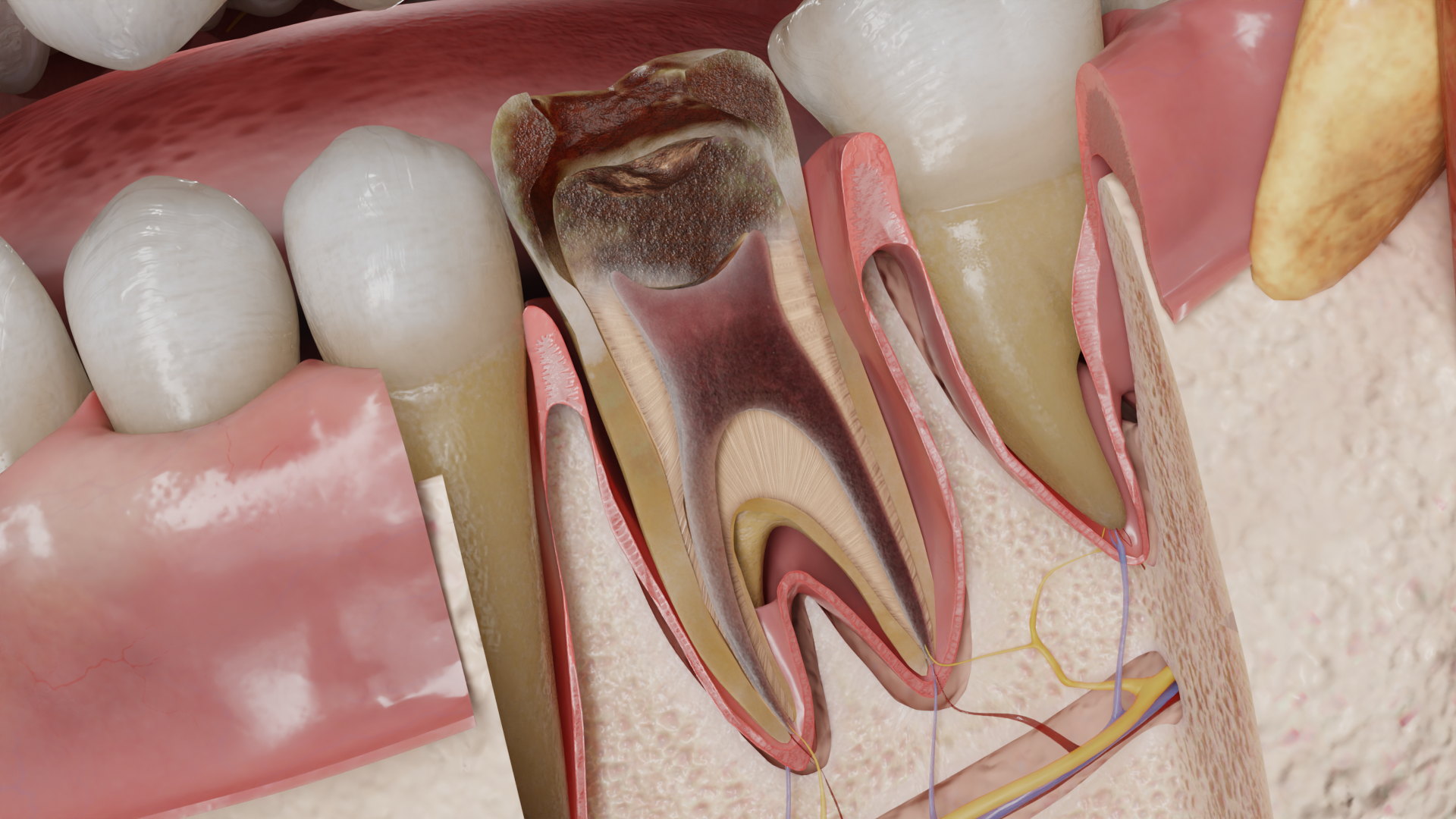
The exudate is initially serous, then sero-purulent and purulent. Pressure increases in the tissues, and a pulp necrosis focus develops. The necrosis zone is surrounded by an accumulation of neutrophilic granulocytes that phagocytize bacteria, and acellular tissue with signs of partial decay. In the surrounding tissues, a picture of chronic inflammation is observed: macrophages, fibroblasts, mast cells, and foam cells. Even a limited necrosis zone is a sign of reversible pulpitis transitioning to irreversible. The initial necrosis area slowly spreads deeper in the apical direction.
As a result of inflammation, purulent melting of the pulp and its necrosis may occur, or the acute process may transition to chronic if spontaneous evacuation of the exudate has occurred.
In chronic pulpitis, proliferative changes are dominant: inflammatory edema disappears, and fibrous elements grow extensively.
Inflammatory mediators, such as bradykinin and histamine, activate type C nerve fibers. C-fibers are unmyelinated, have low conduction velocity, smaller diameter, and a higher excitation threshold than A𝛅 fibers. They are located deeper and are mainly activated by heat, causing dull, aching, excruciating, prolonged, sometimes diffuse pain. Cold exposure in patients with symptomatic irreversible pulpitis can cause vasoconstriction and a drop in pulp pressure, which may provide temporary pain relief. C-fibers also differ from A fibers in their ability to maintain functional integrity during tissue hypoxia and continue to function for a longer time as inflammation progresses. The reaction of C-fibers indicates that pulp damage is irreversible.
Depending on the etiologic factor, the affected tooth may exhibit:
In an acute process, the pulp is edematous, hyperemic, and bright red in color. Small hemorrhages may be found around the vessels. Purulent exudate is initially found as a local accumulation, then spreads to the entire crown and root pulp. The pulp takes on a gray-red or gray color.
In a chronic process, the pulp is replaced by granulation tissue, and then by dense, coarse fibrous scar tissue of a whitish color.
In acute pulpitis, the patient complains of ‘spontaneous’ paroxysmal pain – a sensation that occurs spontaneously regardless of external stimuli. The frequency and duration of pain attacks and ‘light’ pain-free intervals change over time. In the initial stages, short pain attacks (minutes-hours) alternate with long pain-free intervals (hours-days). As the process progresses, the frequency and duration of pain attacks increase. Pain often occurs at night. The nature of the pain is dull, aching, excruciating, prolonged, sometimes sharp and throbbing, can reach considerable intensity and become unbearable. The pain often radiates to neighboring teeth, antagonist teeth, and may migrate.
Exposure to thermal, mechanical, and chemical irritants leads to a prolonged pain attack that persists after the irritant is removed.
Chronic pulpitis is characterized by a discrepancy between the weak expression of the pain symptom and the significant degree of tooth destruction. The patient complains of prolonged pain arising from the action of irritants, while spontaneous and nocturnal pain are usually absent.
Find more scientifically accurate content on our social media








Acute irreversible pulpitis with spontaneous pain is a condition requiring urgent care.
Endodontic treatment: involves complete removal of the pulp, mechanical and medicinal treatment of root canals, and their hermetic obturation followed by tooth restoration.
In permanent teeth with incomplete root formation, revascularization and apexogenesis techniques may be possible.
If the prognosis of endodontic treatment is unsatisfactory, the tooth should be extracted.
1. What is irreversible pulpitis?
2. What are the main causes of irreversible pulpitis?
3. How does acute irreversible pulpitis manifest?
4. What symptoms are characteristic of chronic irreversible pulpitis?
5. How is irreversible pulpitis treated?
6. Can irreversible pulpitis be treated without removing the pulp?
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Berman, L. H., & Hargreaves, K. M. (2020). Cohen’s Pathways of the Pulp Expert Consult. Elsevier.
3.
Jain N, Gupta A, N M. An insight into neurophysiology of pulpal pain: facts and hypotheses. Korean J Pain. 2013 Oct;26(4):347-55. doi: 10.3344/kjp.2013.26.4.347.
4.
Torabinejad, M., Fouad, A., & Shabahang, S. (2020). Endodontics: Principles and Practice. Elsevier.
5.
American Association of Endodontists. (2019, June 3). Guide to Clinical Endodontics – American Association of Endodontists.
https://www.aae.org/specialty/clinical-resources/guide-clinical-endodontics/
6.
Ricucci, D., & Siqueira, J. F. (2013). Endodontology: An Integrated Biological and Clinical View. Quintessence Publishing (IL).
7.
Bergenholtz, G., Hørsted-Bindslev, P., & Reit, C. (2013). Textbook of Endodontology. John Wiley & Sons.
8.
Hülsmann, M., Schäfer, E., Bargholz, C., & Barthel, C. (2009). Problems in endodontics: Etiology, Diagnosis and Treatment. Quintessence Publishing (IL).
9.
Beer, R., Baumann, M. A., & Kielbassa, A. M. (2004). Taschenatlas der Endodontie.
Loading test 6 questions




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io