Post-Infarction Ventricular Septal Defect (PIVSD): Etiology, Pathogenesis and Treatment
Oleg K.Cardiovascular surgeon, MD
14 min read·December 23, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
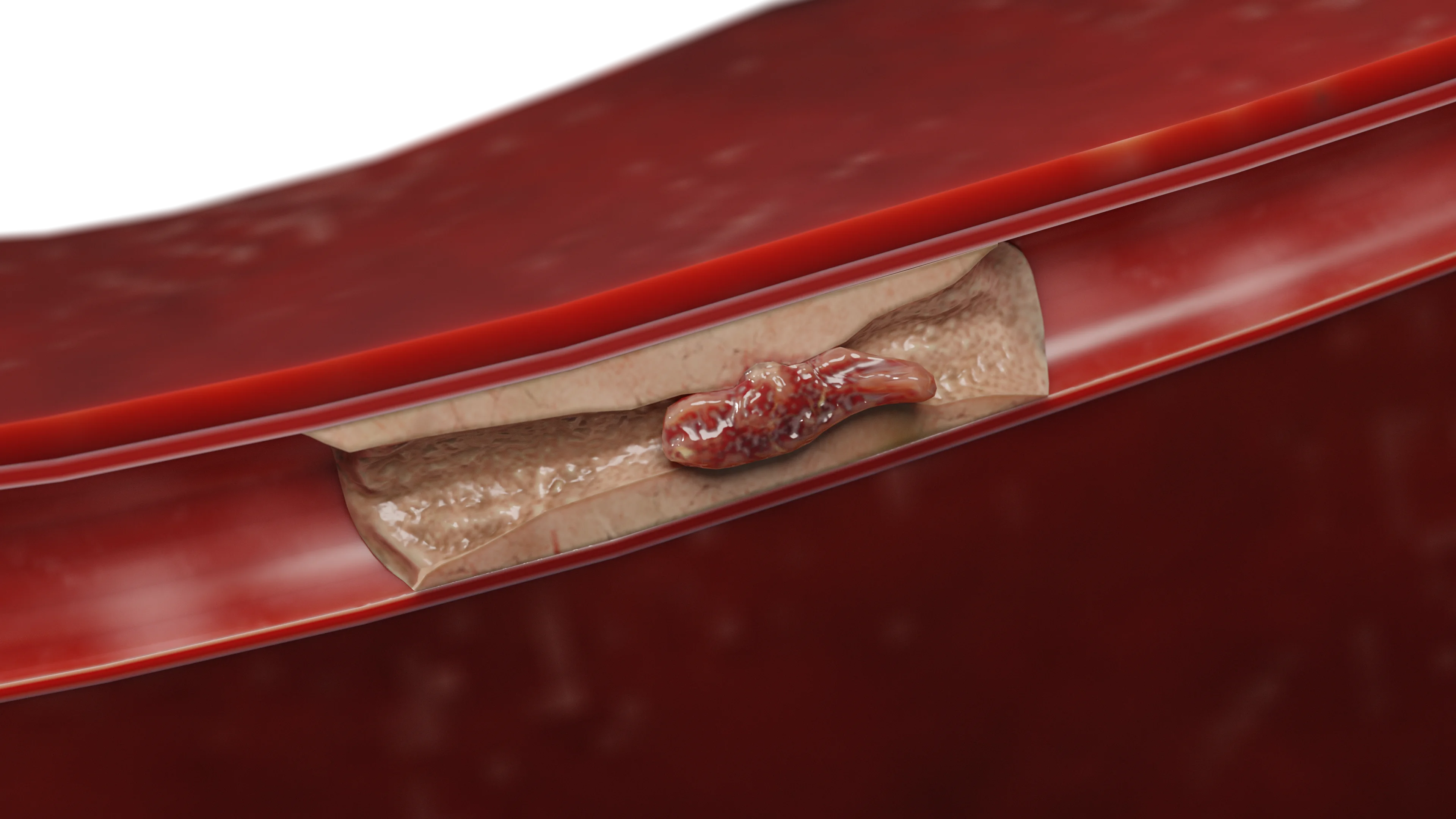
Post-infarction ventricular septal defect (PIVSD) is the formation of a tear (hole) in the ventricular septum of the heart after acute myocardial infarction (MI) in the zone of transmural necrosis. The resulting left-to-right bypass causes significant hemodynamic overload of the right ventricle and small circulation circle. On average, one in four patients without surgical intervention dies within the first 24 hours of developing this complication.
Ventricular septal defect (green arrow) and ischemic myocardial damage (yellow arrow) – 3D model
Etiology and underlying mechanisms of PIVSD
Epidemiology and timing
In current practice, with early reperfusion, the incidence of PIVSD has decreased to ≈0.2–0.5% of all MIs. Most often, ventricular septal defect develops on day 3–5 after infarction; cases in the first 24 hours or later (5–14 days) have also been described.
Localization and main mechanisms
The main artery associated with PIVSD is the anterior interventricular artery. Approximately 60% of cases of PIVSD are localized in the anterior/apical part of the septum, 40% in the posterior/inferior part.
The major mechanisms leading to ventricular septal rupture include:
Inadequate reperfusion. Late or inadequate reperfusion leads to continued necrosis and tissue weakening.
Mechanical loading. Increased pressure/load on the left ventricle (LV) after MI creates additional forces on the weakened septum.
Risk factors. Age-related changes, decreased collaterals, and multiregional coronary atherosclerosis increase the likelihood of interventricular septal rupture.
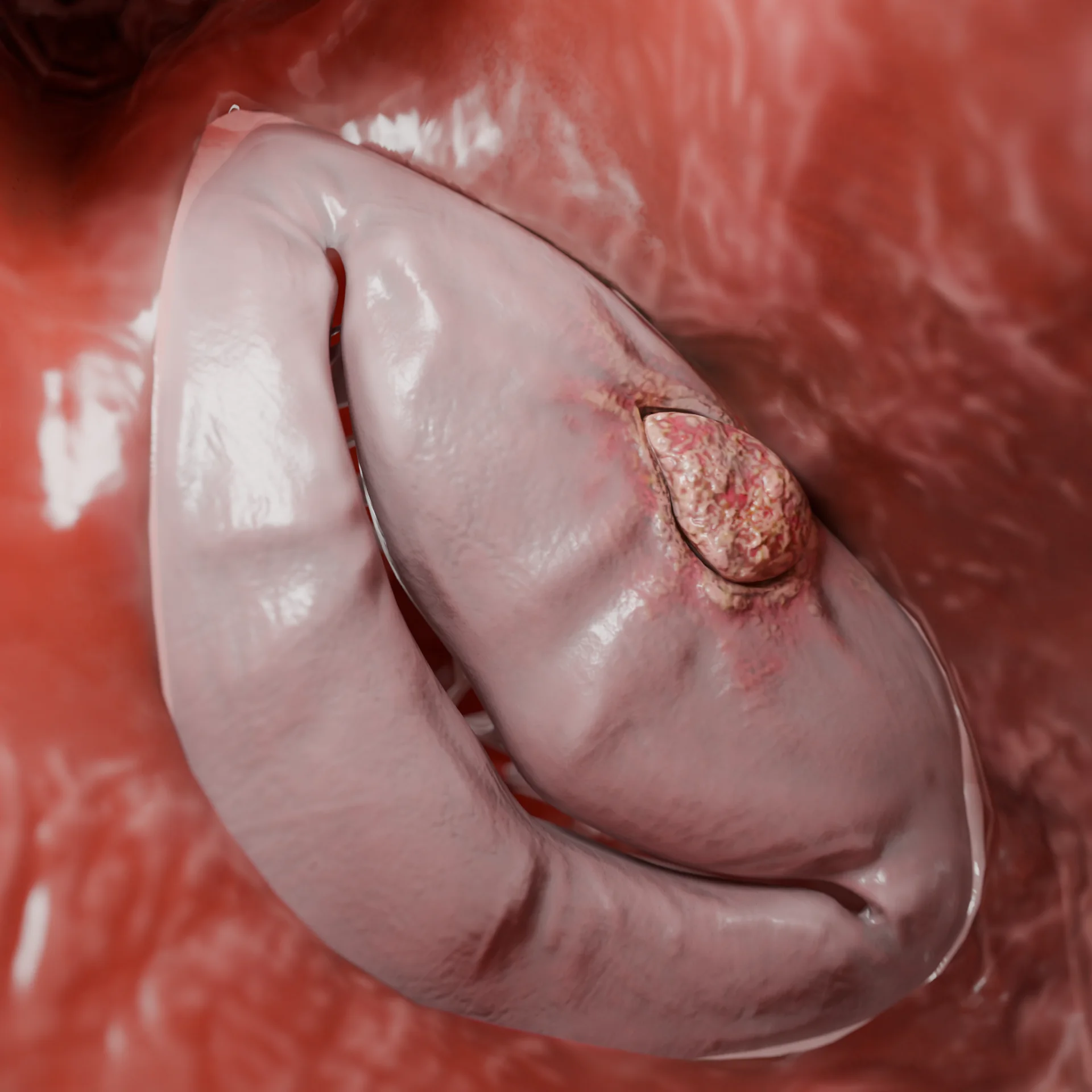
Occlusion of a branch of the left coronary artery – 3D modelThrombotic occlusion of the coronary artery due to critical narrowing by the atherosclerotic plaque – 3D model
Pathogenesis and hemodynamic disorders
Post-infarction ventricular septal defect causes a complex of hemodynamic abnormalities that most commonly lead to acute heart failure:
Septal wall necrosis. In transmural myocardial infarction, extensive necrosis of interventricular septal tissue occurs. Necrotized cardiomyocytes lose their strength.
Structural weakening. Necrosis is followed by enzymatic degradation, inflammatory edema, collagen lysis, and decreased mechanical strength of the septum. This is particularly evident in the first 3 to 5 days after MI.
Rupture and left-to-right bypass formation. Rupture of the ventricular septum occurs, and a pathway from the left ventricle (LV) to the right ventricle (RV) is formed. Excessive left ventricular ejection (left-to-right, or L-R bypass) causes hemodynamic disturbance.
Overload in the small circulation. A large volume of blood flows through the defect from the LV → RV → pulmonary vessels, which leads to increased pressure and volume in the small circulation.
Development of acute heart failure and pulmonary edema. Increased bypass flow leads to overloading of the RV and pulmonary blood flow, decreased effective LV ejection, increased pulmonary artery pressure, and development of pulmonary edema.
Cardiogenic shock and multiorgan failure. With massive defect and unstable hemodynamics, cardiogenic shock, organ hypoperfusion, and a high probability of death may develop.
In summary, infarction → septal necrosis → rupture → left-to-right bypass → overload of the RV and lungs → heart failure/shock.
Classification and clinical manifestations of PIVSD
Anatomical classification
There is no single international classification, but the following characteristics are used for choosing treatment strategy:
Anatomy of the rupture course: simple, complex (tortuous/multilevel course).
Localization: apical, anterior, posterior.
Time of emergence: early (<24 h), “classical” (day 3–5), late (up to 1–2 weeks).
Severity: assessment of defect size, number of defects, and their hemodynamic severity.
Clinical symptoms
The classic pattern of PIVSD includes:
Auscultation. Acute onset of a rasping systolic or systolic-diastolic murmur at the apex of the heart(a key symptom), often shortly after a heart attack. The nature of the murmur may vary depending on the size and number of defects.
Pulmonary symptoms. Pulmonary hypertension, pulmonary edema, and rapidly increasing dyspnea (due to left-right shunting and circulatory overload).
Shock signs. Hypotension, tachycardia, cold sweats, decreased diuresis (signs of cardiogenic shock in the event of massive defect).
General signs. Severe weakness, confusion (due to cerebral and organ hypoperfusion).
Complications. Arrhythmias and thromboembolism are possible.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Diagnosis and treatment methods
Diagnosis of PIVSD
Laboratory methods. Elevated troponin I/T and CK-MB (markers of infarction); elevated BNP/NT-proBNP (heart failure); lactate increase in cardiogenic shock.
Echocardiography (echoCG). The method of choice for diagnosis of ventricular septal defect. Visualizes the defect, left-to-right flow, bypass size, and assessment of LV and RV function. If visualization is poor, a transesophageal echoCG is indicated.
Coronary angiography. Used for coronary evaluation and revascularization planning.
Monitoring. Swan-Ganz catheter to assess RV pressure, pulmonary artery pressure, and cardiac index (especially in shock). Central venous pressure, invasive blood pressure, diuresis control.
MRI/CT of the heart. Rarely used in emergency settings, but may help clarify the size of necrosis and anatomy of the defect.
Treatment of post-infarction defect
The main goal is to stabilize hemodynamics and close the rupture.
Conservative methods. Used temporarily for stabilization. Include inotropes (dobutamine, milrinone) if ejection is reduced, vasodilators and afterload reducers (e.g., nitroprusside) with caution especially in hypotension. Beta-blockers, diuretics, antithrombotic drugs, etc. The use of certain groups of medications is very individualized and depends on the hemodynamic status of the patient.
Mechanical circulatory support: may be considered as a component of conservative therapy or as a bridge to surgical treatment. Support can be performed with intra-aortic balloon counterpulsation, veno-arterial ECMO, and percutaneous intracardiac microaxial pumps.
Interventional techniques (percutaneous closure): use of occluders through vascular access. Indicated for small defects, suitable anatomy and stable hemodynamics. The occluder is placed through transvenous-transarterial access under the control of echoCG and fluoroscopy.
VSD occluder – a generalized example
Surgical methods (gold standard):
Indications: defect of any size + hemodynamic instability (cardiogenic shock, pulmonary edema).
Technique: ventricular septal defect surgery is performed in the setting of cardiopulmonary bypass, most commonly using a patch (synthetic or autopericardial).
Strategy: it is preferable to perform delayed surgery (after 2–4 weeks) when the fibrous cord has formed and the tissues are stronger (provided the patient is stable).
In apical VSD, the incision is made through the infarcted left ventricular apex, followed by possible excision of the apical portion and Teflon sutures (more often two-row: mattress and wraparound) to form a new cardiac apex.
In some cases, the patch plasty technique with exclusion of the infarcted area is used, where the patch is sutured to healthy tissue on the endocardial side and isolates the LV cavity from the defect in the ventricular septum.
Alternative: if all methods are futile, orthotopic heart transplantation is considered.
FAQ
1. What is a post-infarction VSD?
It is a rupture of the interventricular septum that occurs after a myocardial infarction due to necrosis and destruction of the septal muscle.
2. When is it most common to develop a ventricular septal defect after a heart attack?
Usually on the 3rd to 5th day after transmural infarction, less often on the first day or 1–2 weeks later.
3. What symptoms may indicate a post-infarction ventricular septal defect?
Abrupt deterioration after MI, new loud systolic murmur, signs of dyspnea and heart failure.
4. How to confirm the diagnosis of ventricular septal defect?
The main method is echocardiography with color Doppler: visualizes blood flow through the defect and estimates its size.
5. Can post-infarction ventricular septal defect be treated medically?
Conservative therapy (inotropes, diuretics, vasodilators) is used temporarily for stabilization before surgery.
6. What are the risks of early surgery for post-infarction ventricular septal defect?
The edges of the defect are necrotic and friable, poorly holding the suture — high risk of repeated rupture or failure of sutures, so with stable hemodynamics, surgery is tried to postpone for 2–4 weeks from the time of myocardial infarction.
7. How is surgical closure of a post-infarction ventricular septal defect performed?
Usually through the left ventricle (for anterior defects) or through the right ventricle (for posterior defects), with placement of a patch over the healthy edges of the defect.
References
1.
VOKA Catalogue. [Electronic resource].
https://catalog.voka.io/
2.
Cubeddu, R. J., Lorusso, R., Ronco, D., Matteucci, M., Axline, M. S., & Moreno, P. R. (2024, May 14). Ventricular septal rupture after myocardial infarction: JACC Focus Seminar 3/5. Journal of the American College of Cardiology, 83(19), 1886–1901. DOI: 10.1016/j.jacc.2024.01.041.
3.
Artemiou, P., Gasparovic, I., Bezak, B., Hudec, V., Glonek, I., & Hulman, M. (2020, December). Preoperative extracorporeal membrane oxygenation for postinfarction ventricular septal defect: Case series of three patients with a literature review. Journal of Cardiac Surgery, 35(12), 3626–3630. DOI: 10.1111/jocs.15086.
4.
Nasso, G., Condello, I., Vignaroli, W., et al. (2025, January 2). Post-myocardial infarction ventricular septal defects: Incidence and treatment trends during and after the COVID-19 pandemic. Scientific Reports, 15(1), 445. DOI: 10.1038/s41598-024-84983-z.
5.
Al-Bulushi, A., Al Salmi, I., Ahmed, A. R., & Al Rahbi, F. (2023, November 30). Post-infarction ventricular septal defect: A quarter century experience. Sultan Qaboos University Medical Journal, 23(Special Issue), 22–30. DOI: 10.18295/squmj.12.2023.076.
6.
Sánchez Vega, J. D., Alonso Salinas, G. L., Viéitez Florez, J. M., et al. (2022, September 30). Optimal surgical timing after post-infarction ventricular septal rupture. Cardiology Journal, 29(5), 773–781. DOI: 10.5603/CJ.a2022.0035.
7.
Wilson, W. M., & Horlick, E. M. (2016, May 17). Management of post-myocardial infarction ventricular septal rupture. EuroIntervention, 12(Suppl X), X18–X23. DOI: 10.4244/EIJV12SXA4.
8.
Aparicio-Ortiz, A. D., Alonso-Jimenez, M. N., Espejel-Guzman, A., et al. (2024, January). Mechanical complications after myocardial infarction: A comprehensive review. World Journal of Cardiovascular Diseases, 14(1). DOI: 10.4236/wjcd.2024.141005.