Coccyx Fractures: Classification, Symptoms, Signs, Diagnosis, and Treatment
Aleksandr K.Orthopedic surgeon, MD
14 min read·September 02, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
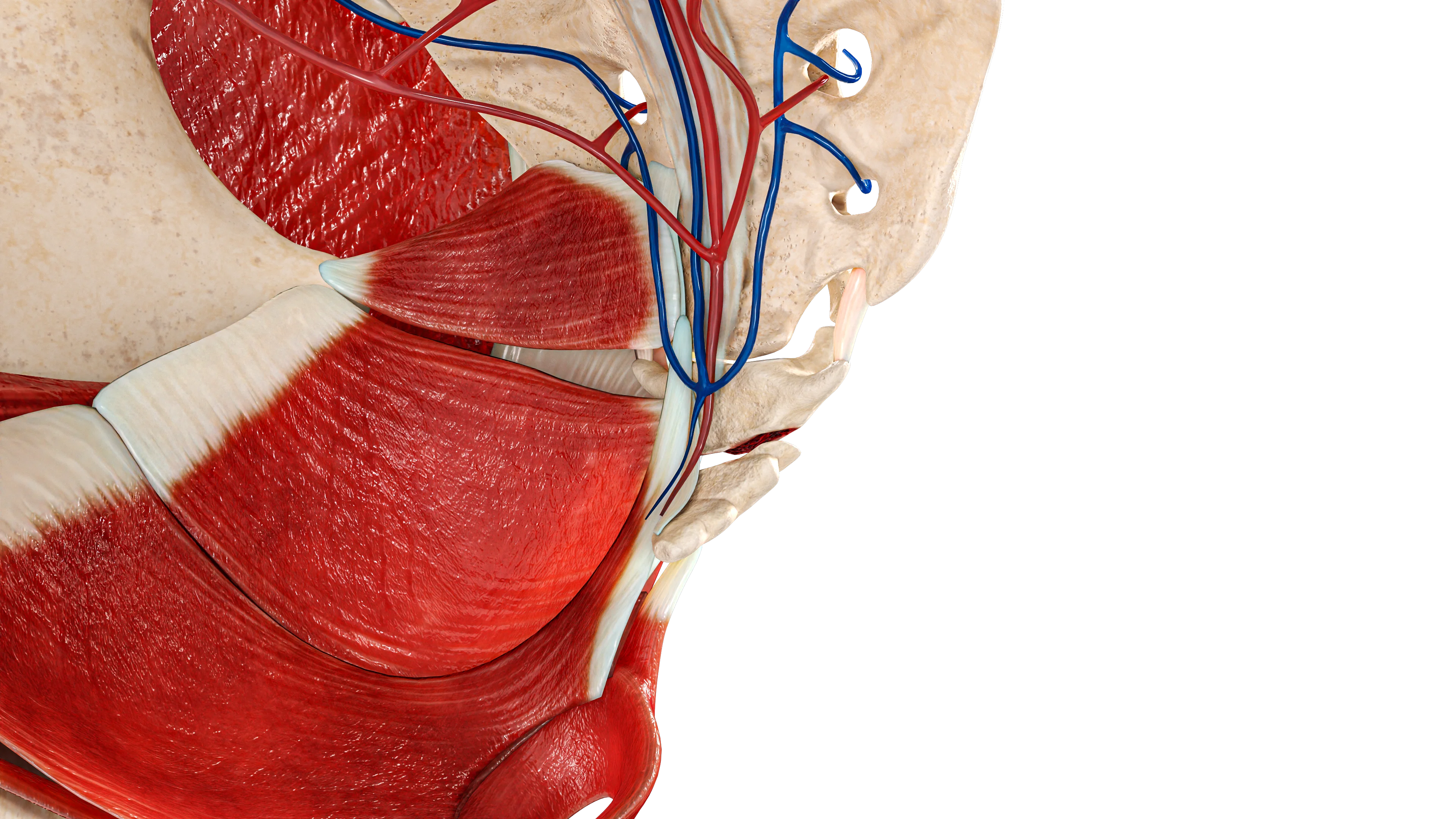
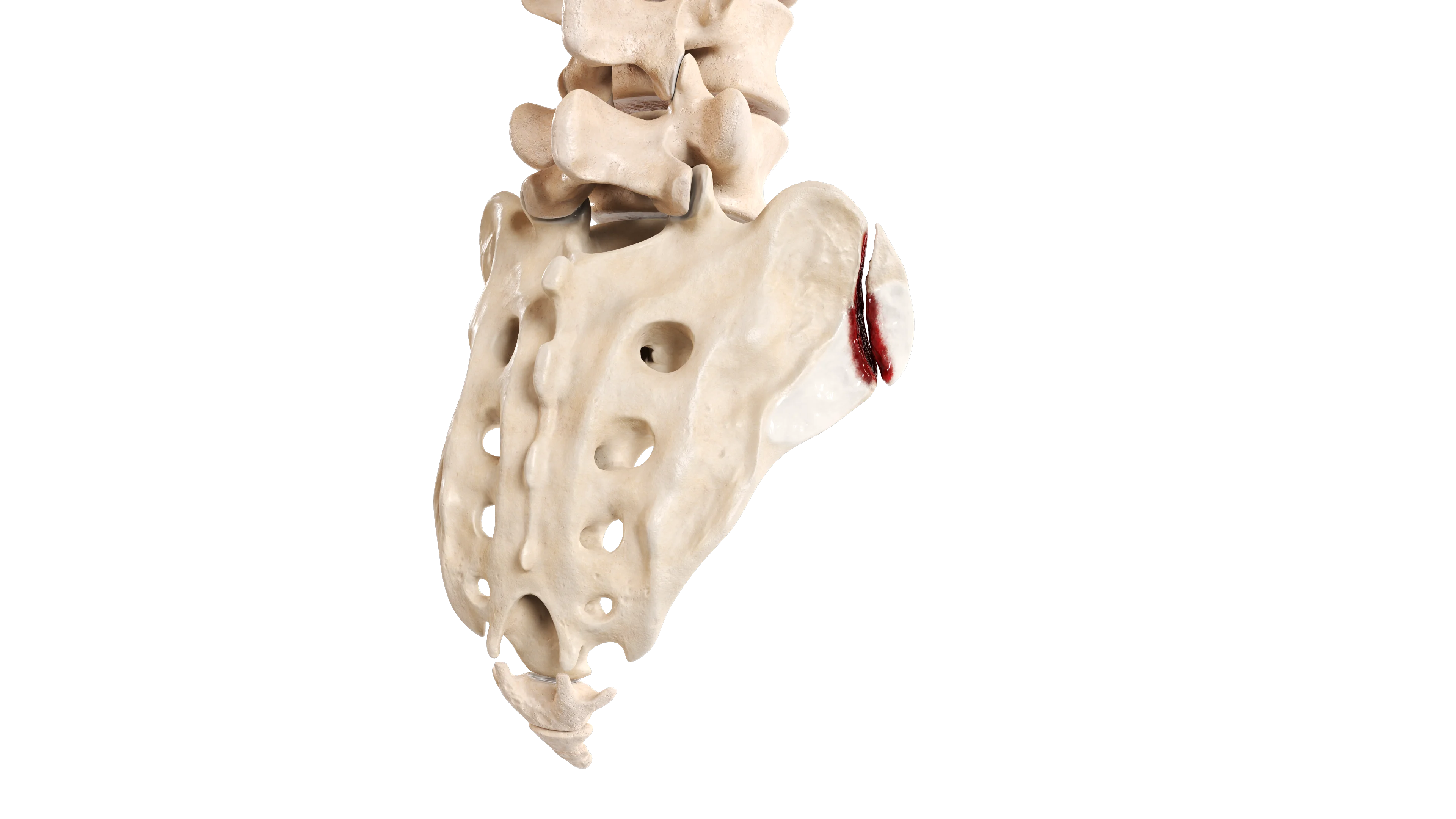
The coccyx is composed of three to five rudimentary vertebrae. It represents the caudal end of the vertebral column and is located inferior to the apex of the sacrum.
Coccyx fractures typically affect the terminal segment of the axial skeleton. Due to their relatively low incidence and subtle symptoms, this condition is always underestimated.
Etiology
Coccyx fractures are primarily caused by:
Direct trauma to the coccyx (e.g., falling backward from a seated position).
Obstetric injuries in women, resulting from pressure exerted by the fetus during labor.
Mechanisms of Injury:
The most common mechanism is a direct axial load, typically occurring during falls onto the buttocks while seated, where force is transmitted directly to the coccyx.
Dislocations or angular fractures may result from oblique or lateral forces.
During labor, the descending fetus can exert significant pressure on the coccyx, particularly in assisted or complicated deliveries.
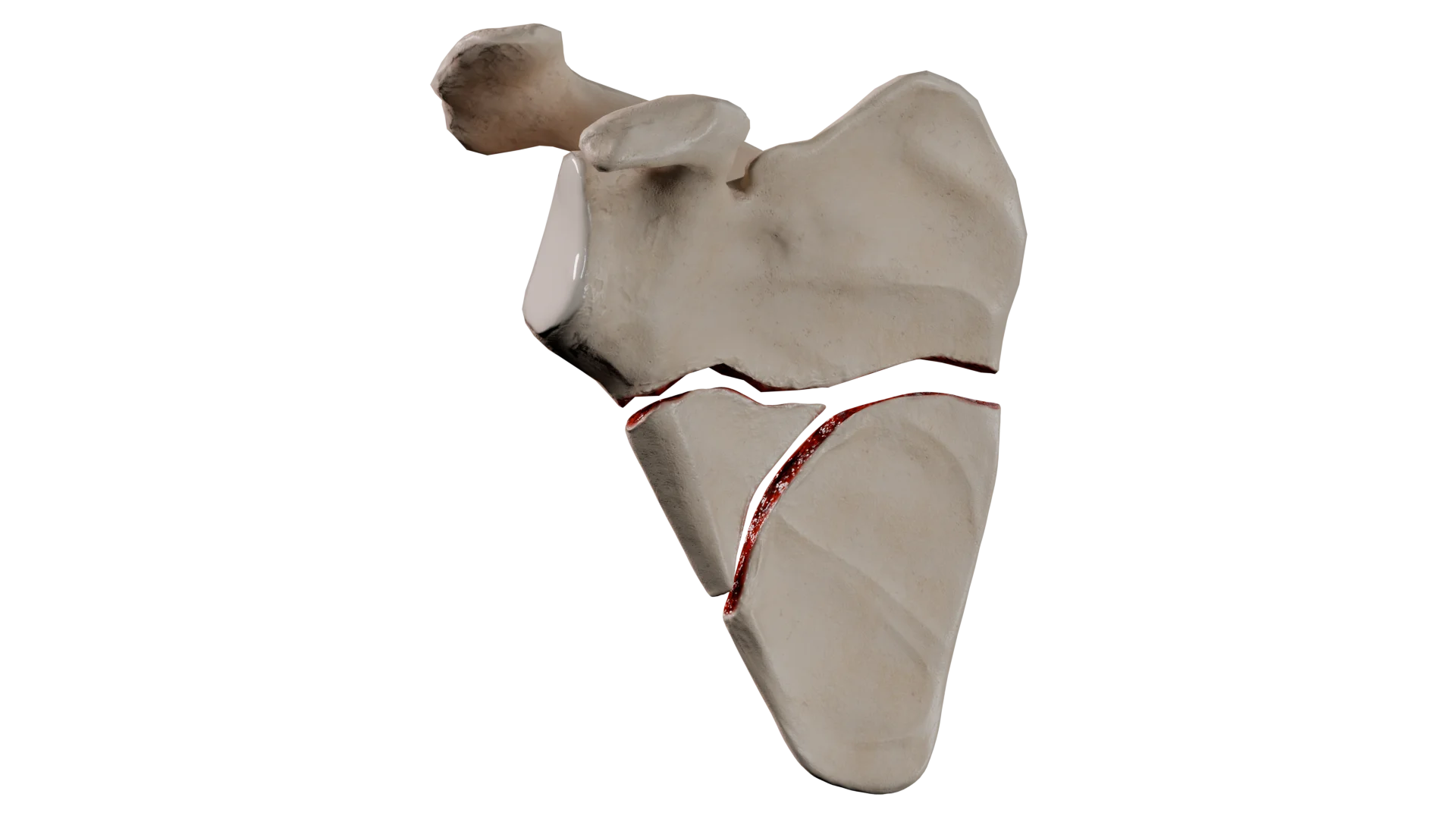
3D Animation: Coccyx Fracture
Epidemiology
Incidence: Coccyx fractures account for a small fraction of all spinal injuries.
Demographics: This type of injury is more common in women, likely due to a wider pelvis and obstetric factors.
Age Distribution: Coccyx fractures are most frequently seen in adults and adolescents; they are rare in children due to greater bone flexibility.
Risk Factors: Osteoporosis, contact sports.
Classification of Coccyx Fractures
There is no universally accepted classification system; however, coccyx fractures may be described as follows:
Non-displaced fracture: A crack without displacement of bone fragments.
Displaced fracture: Bone fragments are misaligned.
Comminuted fracture: The bone is broken into multiple pieces.
Dislocation or subluxation: Misalignment at the sacrococcygeal joint without a true fracture.
Diagnosis is based on clinical evaluation and radiologic imaging.
Clinical Evaluation
Medical History: Recent trauma, fall, or childbirth; onset of pain.
Physical Examination: Tenderness on palpation around the coccyx, swelling, bruising; pain worsens with sitting or standing.
Radiologic methods
Lateral X-ray: Optimal for visualizing dislocations and fractures of the coccyx.
CT (Computed Tomography) and MRI (Magnetic Resonance Imaging): Indicated in cases of non-displaced or comminuted fractures, or to exclude other pathologies (e.g., neoplasms).
Clinical presentation
Typical clinical manifestations in coccyx fractures include:
Pain: Sudden, sharp pain localized around the coccyx, exacerbated by sitting, standing, or defecation.
Local Signs: Pain on mechanical pressure over the coccyx, soft tissue swelling, bruising (in acute trauma).
Chronic Discomfort: In untreated or misdiagnosed cases, chronic coccydynia (persistent coccygeal pain) may develop.
Treatment of Coccyx Fractures
Non-surgical treatment
A conservative approach in coccyx fractures includes:
Rest and avoidance of pressure on the coccyx (e.g., use of a donut-shaped cushion).
Analgesics for pain relief.
Physical therapy: Pelvic floor muscle relaxation and gentle stretching in persistent cases.
Indications for conservative management include:
Most non-displaced, minimally displaced, or isolated fractures.
Absence of significant neurovascular compromise, open wounds, or persistent post-traumatic symptoms.
The prognosis is generally favorable, with recovery occurring over weeks to months.
Surgical therapy
Surgical therapy is rarely required and is reserved for severe cases.
Coccygectomy — surgical removal of part or all of the coccyx — is considered for chronic, refractory coccydynia (pain) after conservative therapy has proven ineffective.
Indications for surgical therapy include:
Persistent pain (chronic coccydynia) unresponsive to conservative treatment that hinders recovery for at least 6–12 months.
Malunion with significant angular deformity.
Soft tissue infections, pressure ulcers, or neurological deficits resulting from acquired coccygeal deformity.
Coccygectomy generally provides pain relief in carefully selected patients but carries risks such as delayed wound healing and infection.
Prognosis by Fracture Type
Unlike most long bones, the coccyx has limited weight-bearing function. However, it serves as a critical attachment site for ligaments, tendons, and pelvic floor muscles. Consequently, even minor fractures or deviations in alignment can lead to chronic pain (coccydynia) and discomfort while seated.
The prognosis depends on the fracture type, associated soft tissue injury, pre-injury coccygeal mobility, and the patient’s age and activity level.
Summary of Prognostic Data by Coccyx Fracture Type
Fracture Type
Healing Time (weeks)
Chronic Pain Risk
Likelihood of Complications
Prognosis
Without displacement
4–8
Low (10–20 %)
Minimal
Excellent; most patients recover with conservative therapy
With displacement
6–12
Moderate (20–30 %)
Malunion may cause persistent pain and sitting intolerance
Long-term pain may persist despite treatment
Comminuted
8-16
High (>30 %)
Fragment nonunion, instability, chronic pain
High risk, long-term pain and discomfort may persist. Sometimes, surgery may be required
Avulsion
4-8
Low to moderate
Instability, chronic pain is rare
Favorable if stable
Non-displaced fractures typically heal within 8 weeks if a conservative approach is chosen; chronic pain is uncommon. Approximately 30 % of comminuted and displaced coccyx fractures may result in chronic pain despite conservative treatment.
Predisposing factors for chronic pain include:
Significant fragment displacement;
Recurrent coccygeal trauma;
Inadequate initial treatment;
Psychosocial influences.
If pain persists for more than 6 months, with radiographic evidence of fragment displacement and failure of conservative therapy, coccygectomy (partial or complete coccyx removal) may be considered. Surgical success rates range from 70 % to 85 %, though risks include infection and tissue degeneration.
Regardless of fracture type, early diagnosis, acute pain control, effective rehabilitation, and patient education are critical for optimal outcomes.
Rehabilitation after Coccyx Fracture
Key rehabilitation principles include:
Pain management;
Guidance on proper posture;
Gradual return to daily activities.
Phases of Rehabilitation
Acute Phase (Weeks 0–2):: The primary focus is pain control, minimizing coccygeal load, and preventing complications. Use of donut-shaped cushions and avoidance of prolonged sitting help reduce pressure on the affected area. Walking and standing are also beneficial.
Subacute Phase (Weeks 2–6): Pelvic and core stability should be restored. During this period, patients should be encouraged to gradually increase their sitting time (with cushion support), begin strengthening and stretching gluteal, piriformis, and pelvic floor muscles.
Recovery Phase (Weeks 6–12): This period aims to restore pre-injury activity levels. Aerobic exercise, swimming, stretching, proprioception, and balance training are appropriate.
Full Activity (Week 12+): Patients are expected to resume their full daily and athletic activities.
Signs requiring special attention during rehabilitation include:
Worsening neurological symptoms: numbness, leg weakness, bowel or bladder dysfunction.
Signs of postoperative infection: fever, increasing swelling, redness around the sutures.
Unusual pain unresponsive to conservative therapy.
Immediate medical evaluation is warranted if any of these symptoms occur.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Management of Chronic Coccydynia
Treatment for chronic coccydynia is divided into stages and includes three levels of intervention:
Conservative therapy. Avoiding prolonged sitting without the use of specialized cushions. Nonsteroidal anti-inflammatory drug (NSAIDs) — either systemic or topical — may provide temporary relief. Short-term muscle relaxants may also be considered for coccygeal pain associated with pelvic or perineal muscle spasms. Physical therapy, manual therapy, and therapeutic rehabilitation are integral components of treatment. Psychological support may also be beneficial.
Interventional approach:
Corticosteroid injection therapy;
Ganglion impar blockade;
Gentle coccygeal mobilization (performed under sedation).
Surgical therapy (coccygectomy). Coccygectomy is reserved for cases with clearly documented instability, dislocation, or persistent pain unresponsive to exhaustive conservative therapy over a period of 6 months or more. Success rates reach up to 85 %, though the procedure carries risks of postoperative complications.
What are the main signs and symptoms of a coccyx fracture?
The hallmark symptom is sudden, sharp pain localized to the coccygeal region. Such pain typically intensifies when sitting, rising from a seated position, or during defecation. Additional signs may include tenderness to palpation over the injury site, soft tissue swelling, and bruising.
2. Why is a coccyx fracture potentially serious, and what are the possible consequences?
The primary concern is chronic pain syndrome, known as coccydynia. This condition can significantly impair a patient’s quality of life, causing persistent discomfort and intolerance to sitting. Malunited, deformed fractures may result in long-standing pain, occasionally requiring surgical intervention.
3. How long does it take for a coccyx fracture to heal?
Healing time depends on the fracture type: Non-displaced fractures typically heal within 4–6 weeks. Displaced fractures may require 6–8 weeks or longer, while complex comminuted fractures may take 8–16 weeks for complete union.
4. How is a coccyx fracture treated?
The vast majority of coccygeal fractures are managed conservatively. Treatment includes rest, use of donut-shaped cushions to relieve pressure from the coccyx while sitting, and analgesics. Surgical treatment (coccygectomy, or removal of the coccyx) is rarely indicated and reserved for cases of persistent chronic pain unresponsive to conservative therapy over 6–12 months.
5. What should be avoided after a coccyx fracture, and is walking allowed?
During the acute phase (first 2 weeks), direct pressure on the coccyx should be avoided. Prolonged sitting — especially on hard surfaces without orthopedic support — should be minimized. Walking and standing are not contraindicated and are generally beneficial, as they do not place direct load on the injured area.
6. What is the difference between a coccyx fracture and a severe contusion?
Symptoms of contusion and fracture are often similar, making clinical differentiation difficult without imaging. Definitive diagnosis requires radiologic evaluation. Lateral X-ray is the most informative modality for visualizing fracture lines or dislocations. In ambiguous cases, CT or MRI may also be indicated.
References
1.
VOKA Catalog.
https://catalog.voka.io
2.
Zhang Y, Gao G. Progress in the diagnosis and treatment of fracture-dislocation of the coccyx (Review). Exp Ther Med. 2025 May 6;30(1):127.
3.
Won H, Moon SY, Park JH, Kim JK, Kim HS, Baek SH, Kim SY, Lee YK, Koo KH. Epidemiology and risk factors of coccyx fracture: A study using national claim database in South Korea. Injury. 2020 Oct;51(10):2278-2282.
4.
Maigne JY, Doursounian L, Jacquot F. Classification of fractures of the coccyx from a series of 104 patients. Eur Spine J. 2020 Oct;29(10):2534-2542.
5.
Lin CH, Wu SY, Hu WL, Hung CH, Hung YC, Aurea Kuo CE. Laser acupuncture for refractory coccydynia after traumatic coccyx fracture: A case report. Medicine (Baltimore). 2020 Feb;99(6):e18860.
6.
Izci EK, Keskin F. Coccygectomy for coccygodynia: A single-center experience. Medicine (Baltimore). 2023 Jun 2;102(22):e33606.
7.
Celenlioglu AE, Sir E. Predictive factors affecting treatment success in ganglion impar block applied in chronic coccygodynia. Reg Anesth Pain Med. 2022 Jun 23:rapm-2022-103582.
8.
Guo F, Yang Z, Tang L, Ming F, Guo Y, Zhu Y. An intrapartum coccygeal fracture: An easily missed buttock pain. Eur J Obstet Gynecol Reprod Biol. 2019 May;236:259-260.