Hemothorax: Causes, Symptoms, Diagnosis, and Treatment

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Hemothorax is an accumulation of blood in the pleural cavity with a ratio of pleural fluid hematocrit to peripheral blood hematocrit of 50% or more.
Etiology
This pathology occurs due to damage of various sizes of arteries and veins of the lung parenchyma, chest wall, mediastinum, diaphragm, etc. The most common cause of hemothorax is chest trauma (non-penetrating, penetrating or iatrogenic). Non-traumatic causes (oncologic diseases, tuberculosis, coagulopathies, etc.) are less common.
In our application models, we consider variants of hemothorax of traumatic genesis.
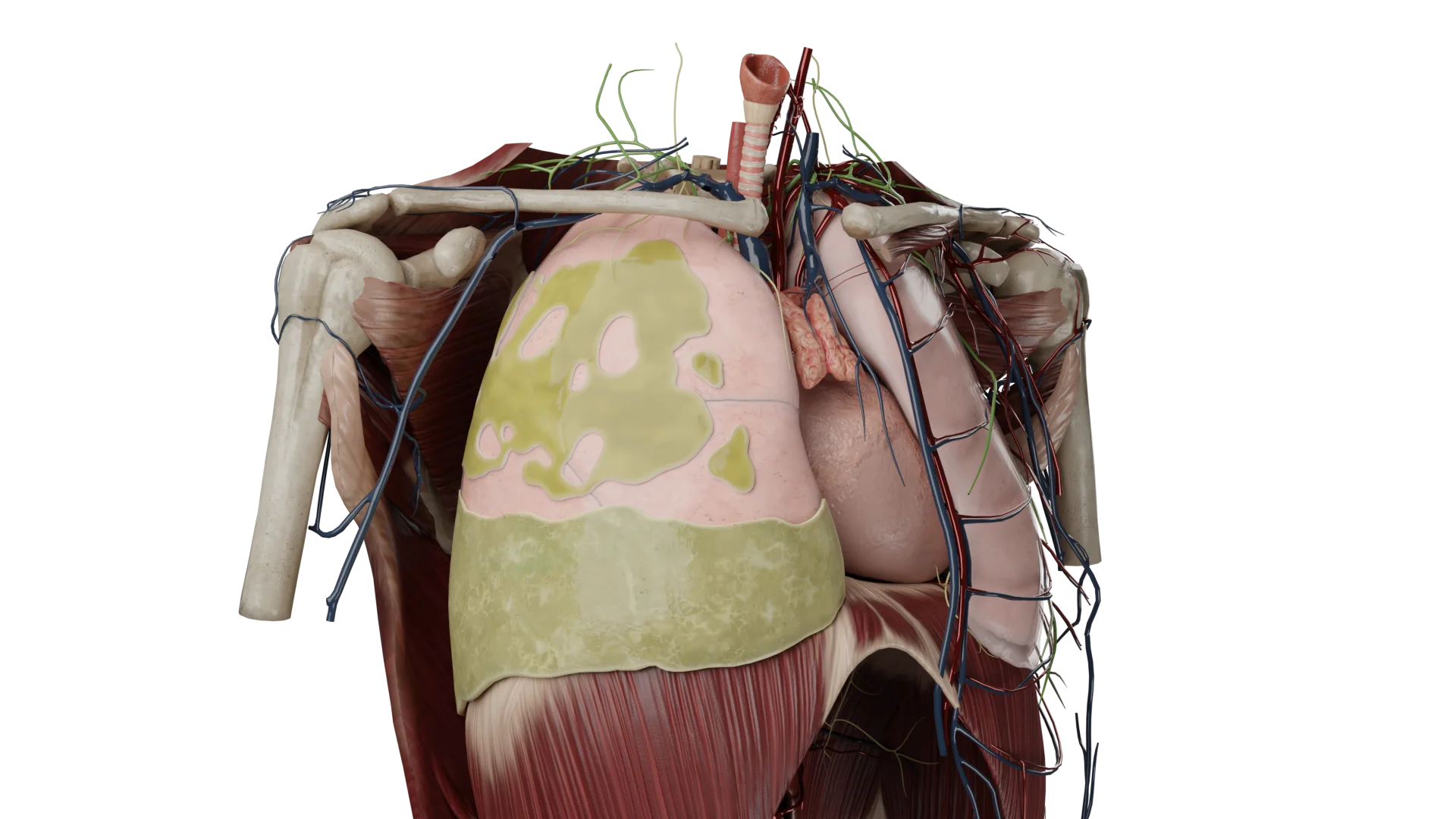
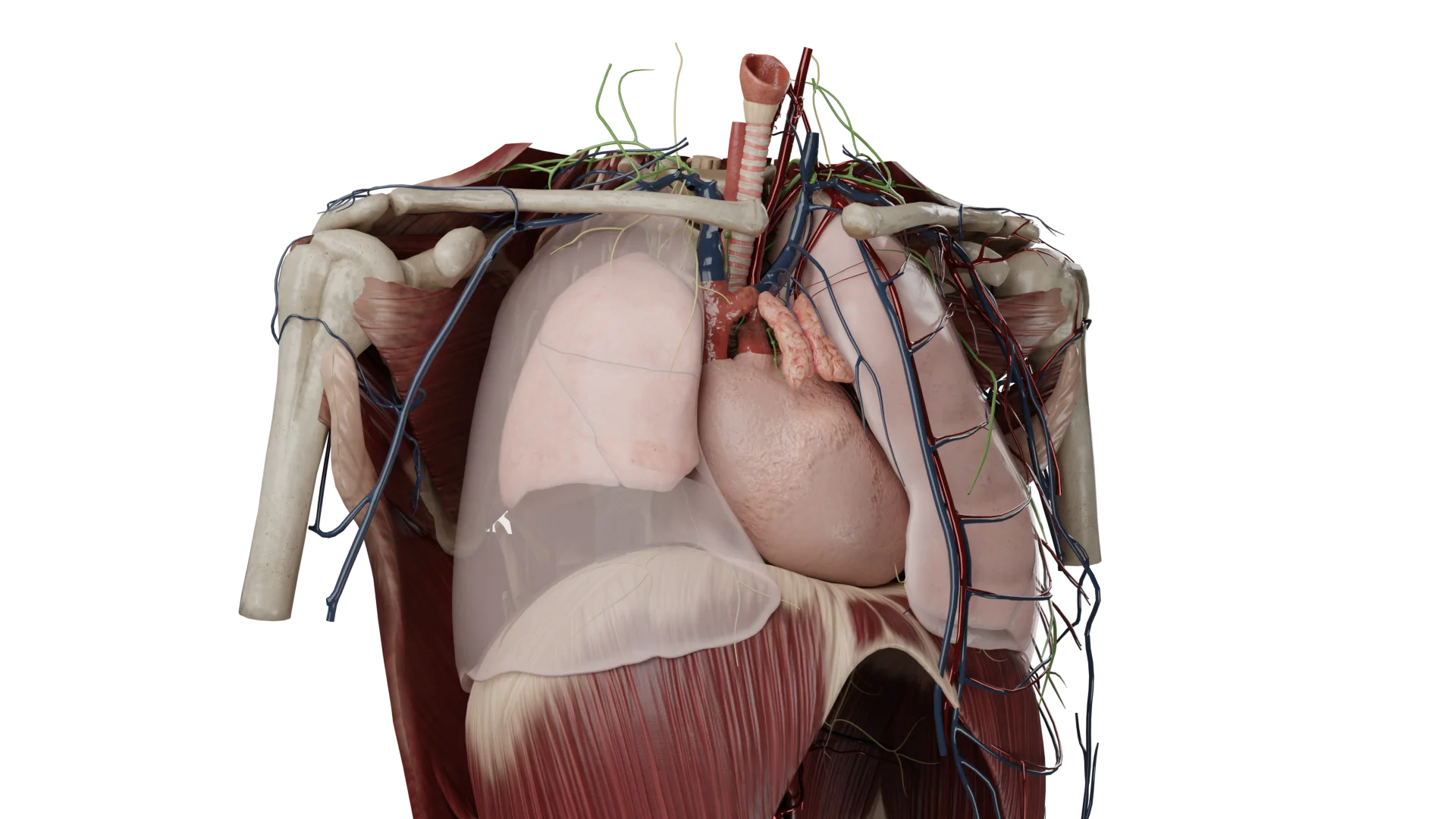
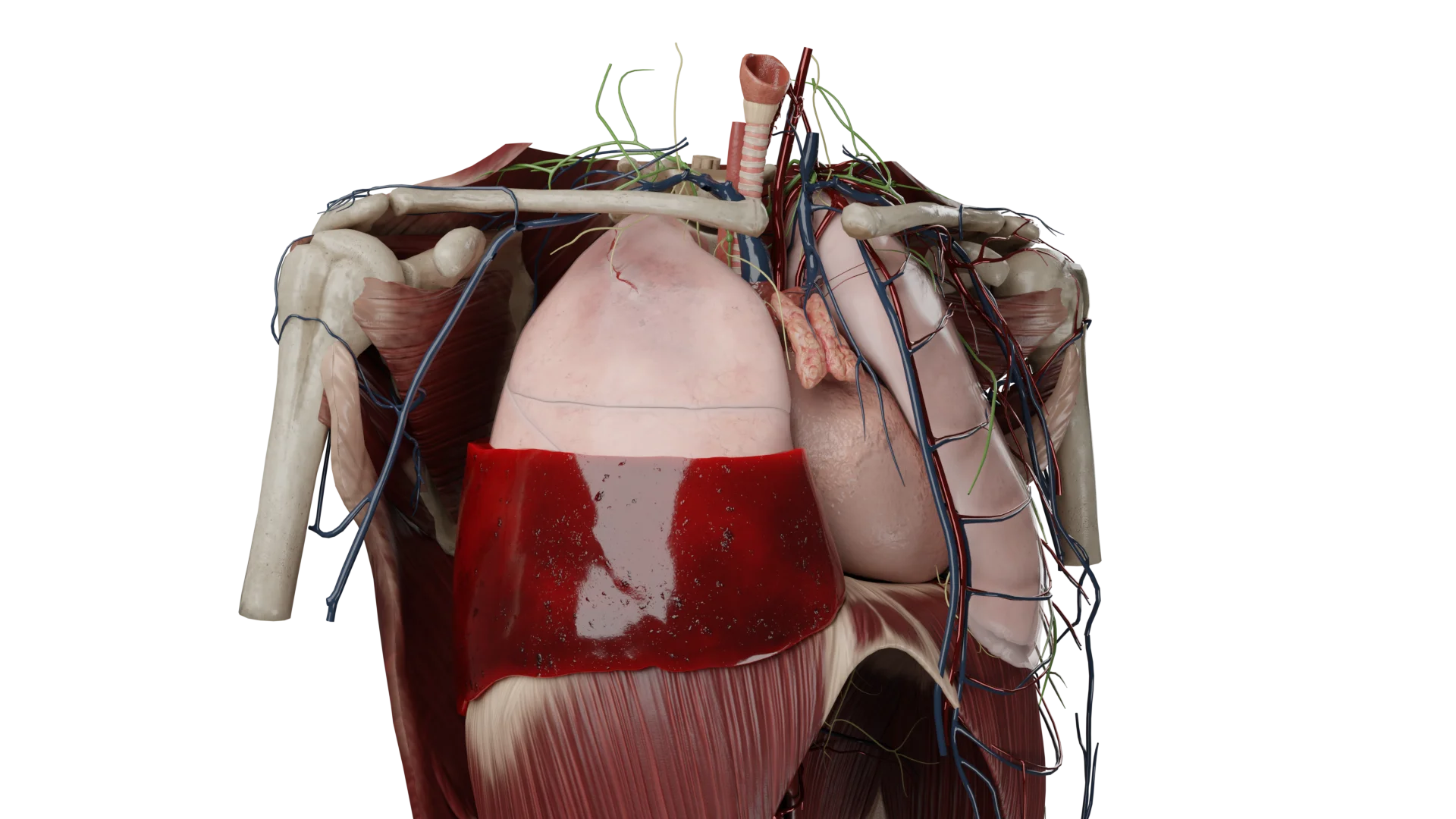
Anatomic Pathology
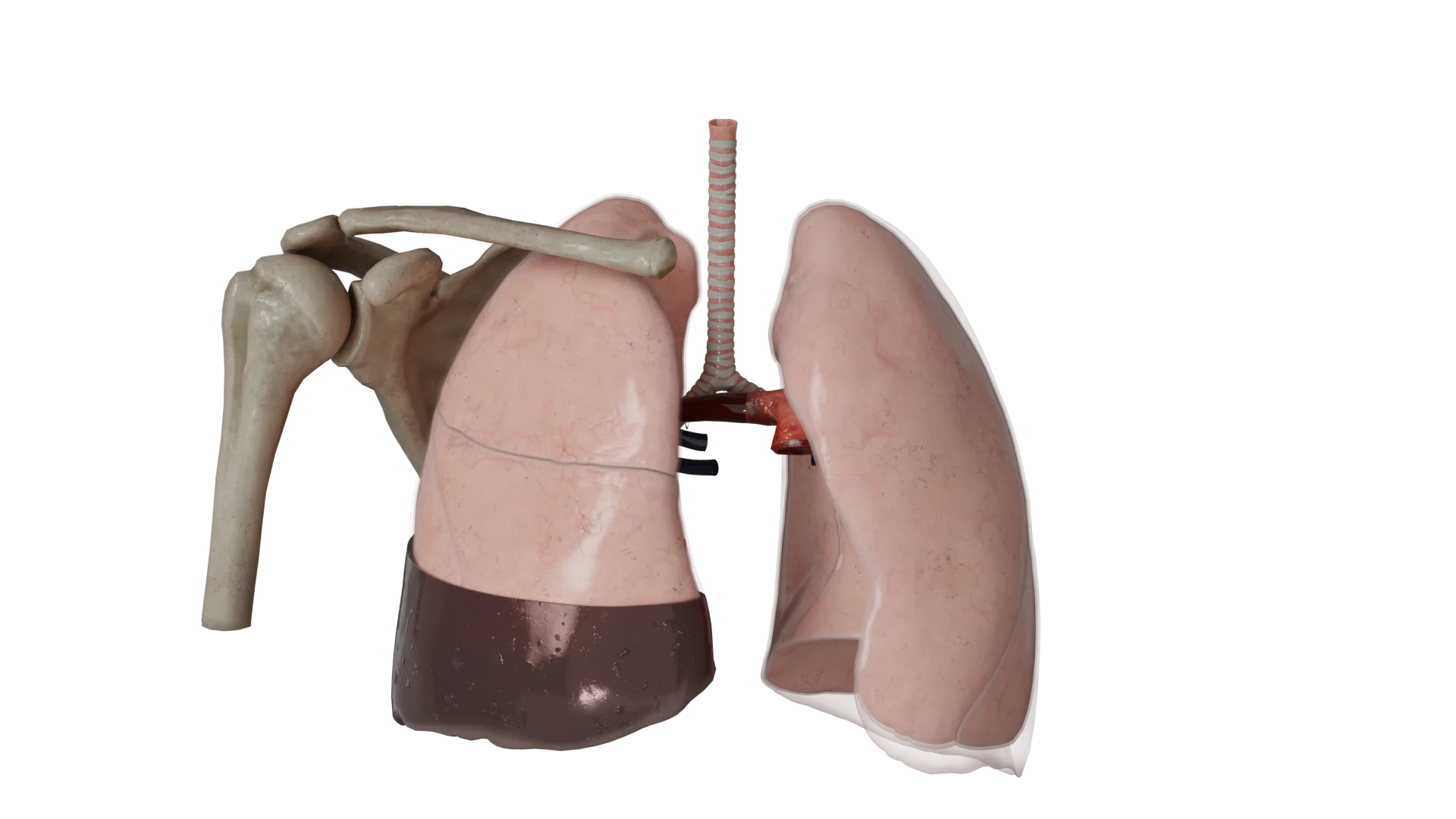
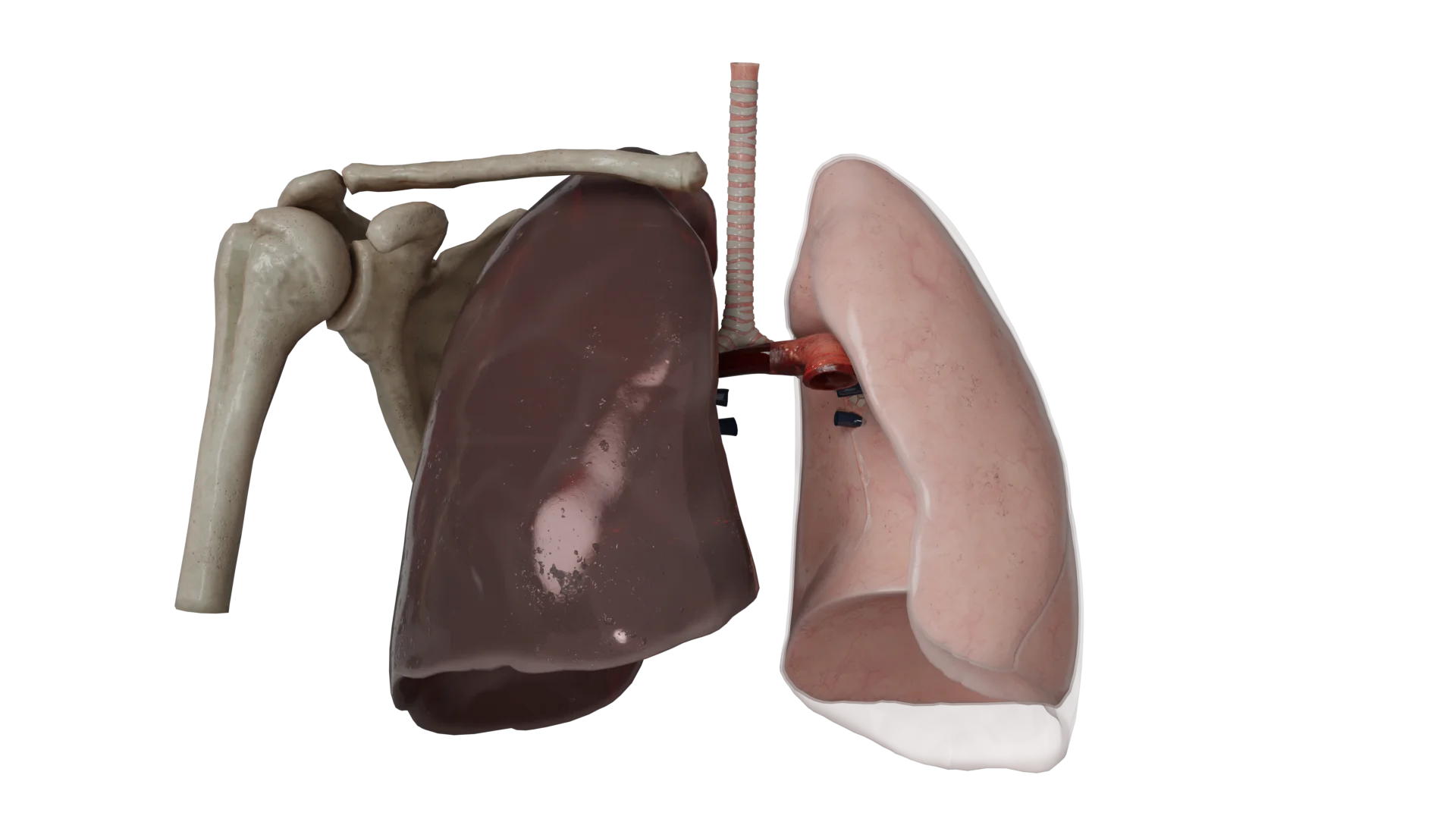
All hemothorax models present a mock-up of a person in the upright position.
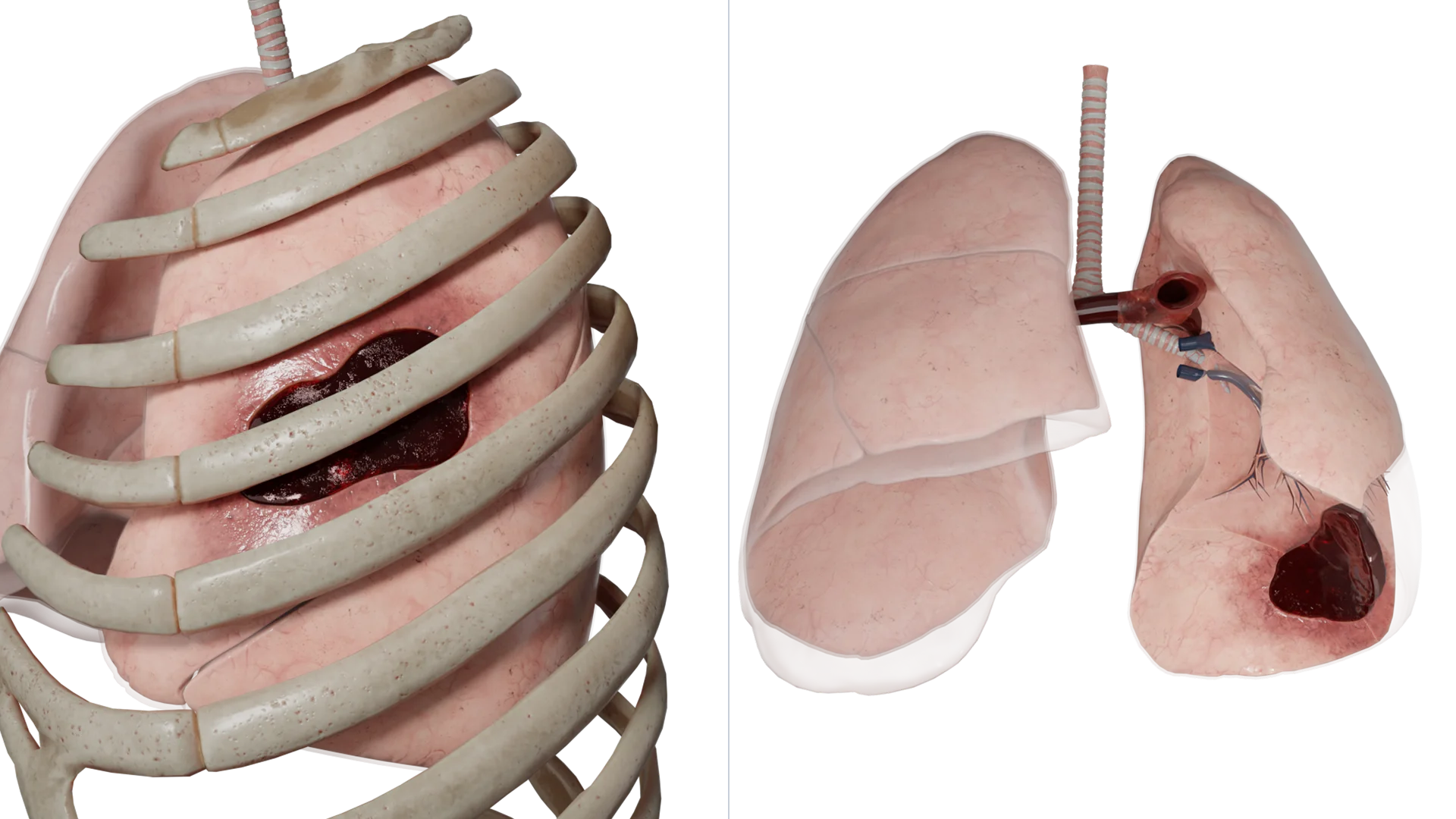
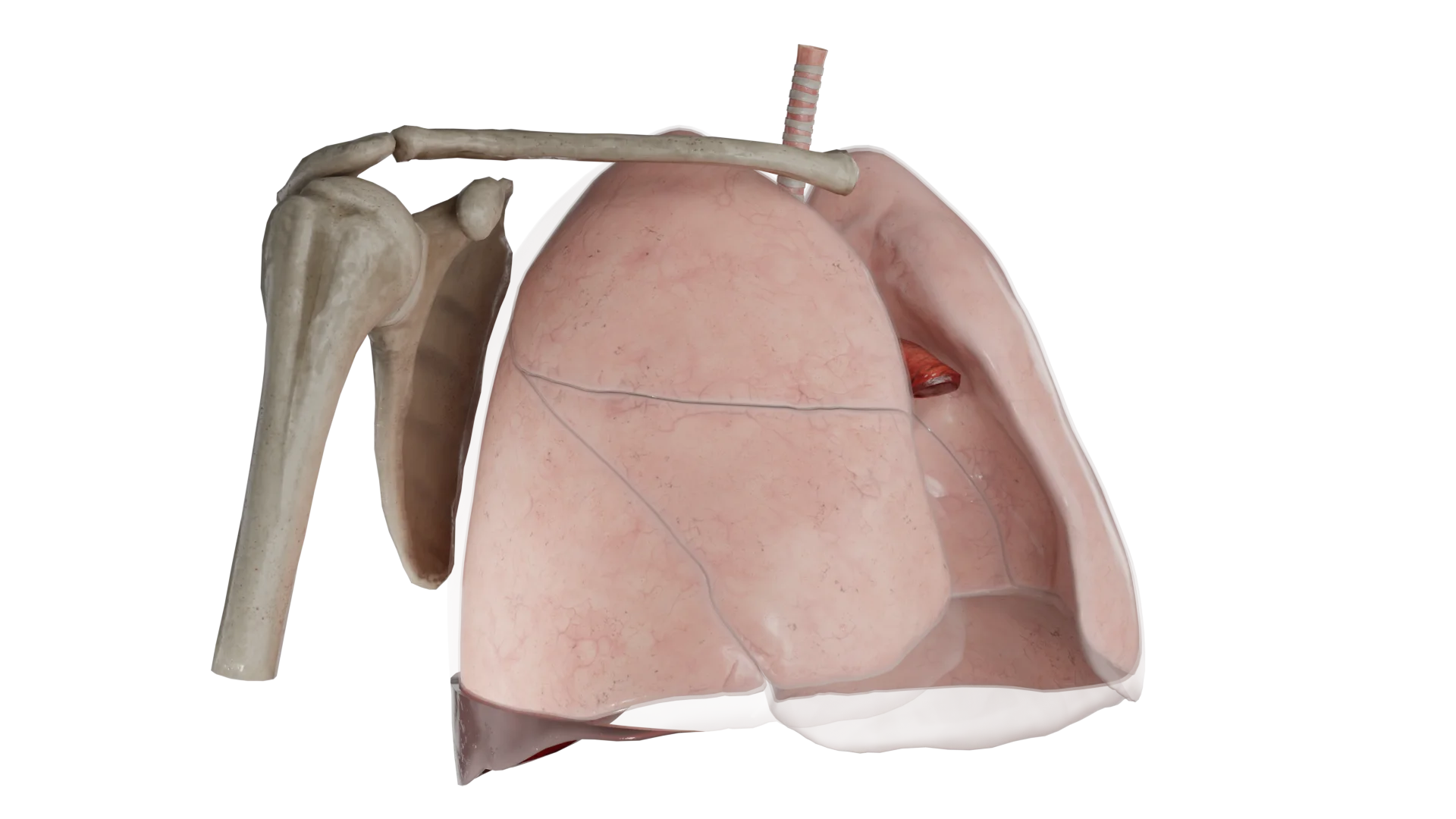
In hemothorax, a horizontal level of fluid can be seen, with a damaged intercostal vessel on the posterior surface of the chest. In moderate and massive hemothoraxes, the volume of blood presses on the lung and collapses it.
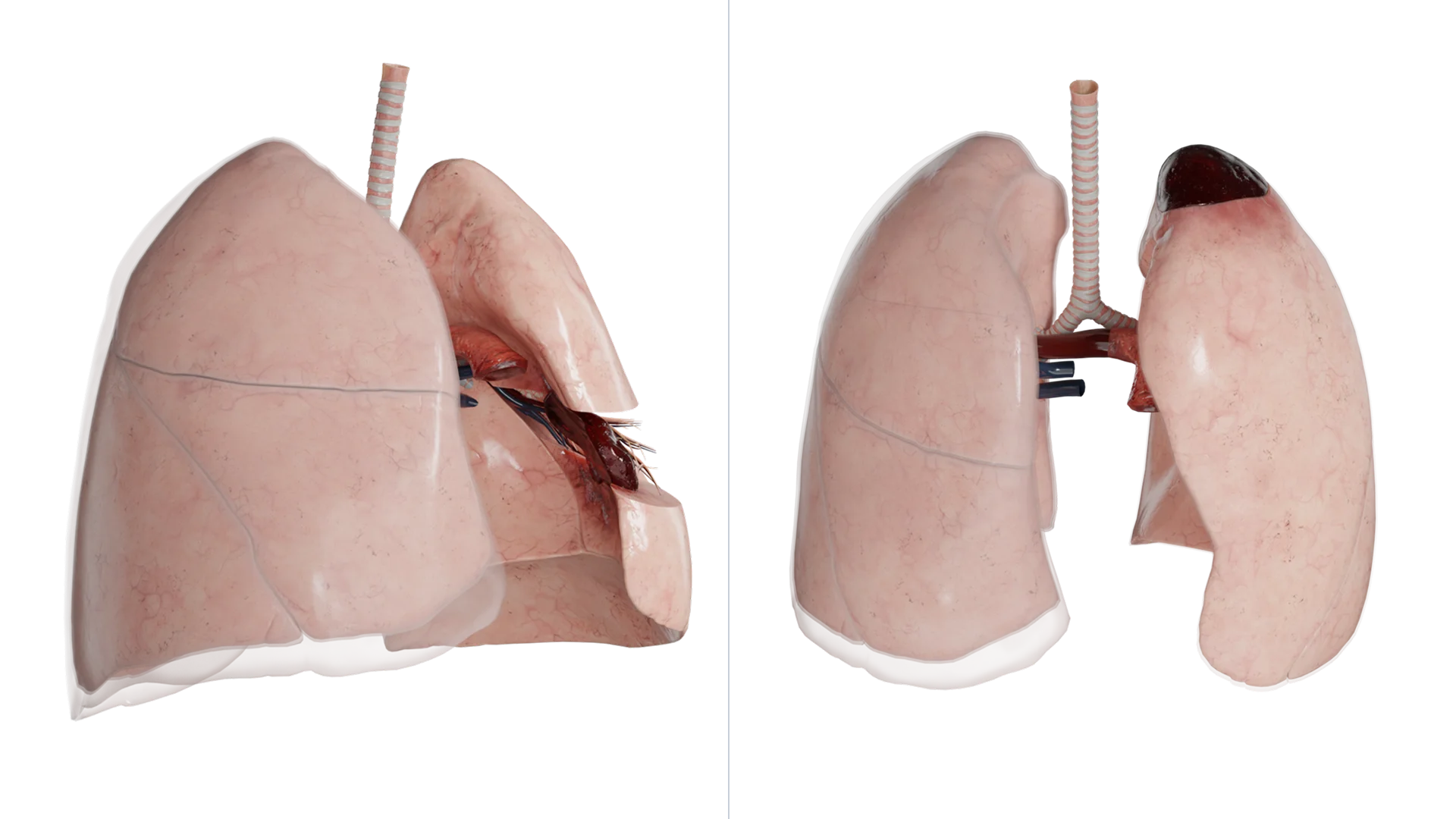
In models of detached hemothorax we see drained blood of various localizations.
Classification
By etiology, they are distinguished:
- Traumatic;
- Pathologic (due to disease);
- Iatrogenic (as a complication of medical interventions).
Hemothorax is classified according to the volume of blood in the free pleural cavity in adults (in children, due to the large amplitude of sex and age differences, it is better to use radiologic classification):
- Small (up to 400 ml);
- Medium (400 to 1000 ml);
- Massive (more than 1000 ml).
A detached hemothorax happens:
- Apical/apical;
- Intershare;
- Supradiaphragmatic;
- Paracostal;
- Paramediastinal.
By the presence of bleeding:
- With the bleeding that took place;
- With continued bleeding.
By the presence of complications hemothorax comes:
- Uncomplicated;
- Complicated, dividing into coagulated (fibrothorax) and infected (pleural empyema).
Pathogenesis
Internal bleeding in trauma leads to accumulation of blood in the pleural cavity, which further causes compression (compression) of the lung on the affected side, and with continued bleeding – to displacement of the mediastinum to the healthy side and compression of the healthy lung. Because of this, there is a decrease in respiratory volume and respiratory surface of the lung and, as a consequence, impaired gas exchange. Also displacement of the mediastinum with compression of hollow veins and pulmonary vessels has an unfavorable effect on hemodynamics. The clinic of acute respiratory and cardiac failure appears.
Clinical Manifestations
Uncomplicated hemothorax
Symptoms and signs may be due to the etiology of the hemothorax, such as pain from rib fracture. Clues to the diagnosis come from the patient’s medical history.
The course may be asymptomatic at low volumes of single blood loss. Or have a latent period (imaginary well-being) at a low rate of blood loss or overexpressed compensatory capabilities of the body. May have nonspecific symptoms in relation to the pathology: pain or discomfort in the chest, cough, dyspnea.
The most common manifestations include signs of tachypnea, tachycardia, and hypotension. The skin and mucous membranes of such patients are pale or cyanotic. In severe course of the process is characterized by a frequent thready pulse, suffocation in the supine position, lack of consciousness or loss of consciousness when the patient is verticalized.
Complicated hemothorax
When infection occurs, there is a clinic of general inflammatory syndrome: hyperthermia, fever, chills, pain on the affected side, cough, asthenic syndrome and so on.
Fibrothorax may be asymptomatic, with marked compression of the lung, the clinic of chronic respiratory failure joins.
Diagnosis of hemothorax
Anamnesis
Trauma (even minor), malignant neoplasm, or recent medical intervention are most commonly reported.
Physical examination
Carefully looking for any signs of trauma such as bruising or soreness of the ribs/chest wall is a must.
Physical examination findings are usually consistent with the clinic of any pleural effusion.
On percussion of the affected half of the chest there may be a shortening of the percussion sound, the upper border of fluid, if there is no pneumothorax, may form the Damoiseau line. The heart boundaries may be displaced to the healthy side.
At auscultation of the lungs is determined by weakening of respiratory noises or their absence.
The clarity of the physical signs of fluid depends on the magnitude of the hemothorax.
Chest radiography
Routine method of diagnosing hemothorax. It is a relatively quick and inexpensive method of investigation. It can provide information about the underlying etiology, concomitant complications (e.g. rib fracture), lung collapse, mediastinal displacement, etc., as well as the underlying cause. Hemothorax can usually be visualized when the volume of blood in the pleural cavity is greater than 500 mL in adults. In this case, the darkening on the radiograph occupies the pleural sinuses. In a medium hemothorax, the level of darkening reaches the angle of the scapula. In a large hemothorax, blood occupies almost the entire pleural cavity. However, early hemothorax may not be seen on radiographs if images are obtained in the supine position (typical of trauma).
This method does not have good screening capabilities in closed chest trauma, with a sensitivity of up to 50%. If significant clinical manifestations are present, the sensitivity increases only to 75%.
Ultrasound (ultrasound)
It has high specificity and allows to detect pleural fluid in the volume of 100 ml with an accuracy of 100%, and from 20 ml – with an accuracy of 75% (in adults). Ultrasound is an alternative method when computerized or magnetic resonance imaging (CT, MRI) is not possible. However, the study is difficult in subcutaneous emphysema and obesity.
One disadvantage of ultrasound is that it cannot provide confirmation of the etiology of hemothorax and associated information about other thoracic structures (e.g., aortic dissection) to the same extent as CT/MRI.
Computed tomography and magnetic resonance imaging
The methods have the highest diagnostic sensitivity in relation to hemothorax. Since they allow to characterize in 3D space both the presence of fluid and its localization, for example, in case of delimited hemothorax. The disadvantages are high cost, ionizing radiation in CT, the need to transport the patient to a specialized department, and the availability of devices is not in every clinic.
Additional diagnostic methods
Diagnostic puncture or drainage of the pleural cavity to visualize the aspirate. After collection of the contents, a Rouvelois-Gregoire test may be performed to determine whether bleeding is ongoing or has occurred.

Hemothorax treatment
Hospitalization in the surgical department under the supervision of a thoracic surgeon.
Hemothorax of less than 260-300 ml with separation (divergence) of pleural sheets 1.5-2 cm in adults usually resolves without complications and additional intervention. If the patient is stable in this situation, conservative treatment is possible with dynamic observation, serial hemoglobin analysis, repeated radiography or ultrasound to ensure that the hemothorax does not progress. Conservative treatments include symptomatic (including oxygen therapy), hemostatic, hemostatic, hemotransfusion, antiaggregant, immunocorrective, and antibiotic therapy.
Indications for blood evacuation (thoracocentesis and drainage) are progressive clinical course of hemothorax, blood volume more than 300-500 ml in adults and separation of pleural sheets more than 3 cm.
Thoracoscopy with blood removal for urgent indications is performed in the first 24-72 hours after trauma in the stable condition of the patient for residual, recurrent or coagulated hemothorax, preventing lung expansion, as well as for the prevention of infection.
The presence of 1500 ml or more of blood in the pleural cavity or dynamic inflow of more than 250 ml of blood hourly for three consecutive hours through the drainage tube are indications for emergency surgical intervention (thoracoscopy, thoracotomy). Vascular ligations, suturing of lung and/or pericardial wounds, removal of accumulated blood, etc. are performed.
FAQ
1. What is the danger of blood pooling in the pleural cavity?
• Lung compression: leads to respiratory failure;
• Mediastinal displacement: disrupts the heart and blood vessels;
• Massive blood loss: can cause hemorrhagic shock;
• Infection: development of pleural empyema (purulent inflammation);
• Fibrothorax: formation of scar tissue that limits the mobility of the lung.
2. What complications can occur with hemothorax?
• Pleural empyema: purulent inflammation of the pleural cavity;
• Fibrothorax: scarring of the pleural sheets resulting in restricted mobility of the lung;
• Hemorrhagic shock: due to massive blood loss;
• Sepsis: due to infection and spread of infection throughout the body.
3. When is surgical intervention required?
• Blood volume more than 1500 ml;
• Continued bleeding: more than 250 ml/hour through drainage;
• Convoluted hemothorax: when blood cannot be removed through drainage;
• Infected hemothorax: development of pleural empyema;
• Traumatic injuries: requiring wound closure or reconstruction.
4. How can complications of hemothorax be prevented?
• Strict adherence to recommendations: if necessary, timely drainage under the supervision of a surgeon, taking prescribed medications (antibiotics, hemostatics);
• Control examinations: X-ray, ultrasound or CT scan to assess the dynamics;
• Prevention of infections: observing sterility during dressings and drainage;
• Rehabilitation: breathing exercises to restore lung function.
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Patel NJ, Dultz L, Ladhani HA, Cullinane DC, Klein E, McNickle AG, Bugaev N, Fraser DR, Kartiko S, Dodgion C, Pappas PA, Kim D, Cantrell S, Como JJ, Kasotakis G. Management of simple and retained hemothorax: A practice management guideline from the Eastern Association for the Surgery of Trauma. Am J Surg. 2021 May;221(5):873-884. doi: 10.1016/j.amjsurg.2020.11.032. Epub 2020 Nov 17. PMID: 33487403.
3.
Васильев И.В., Ли В.Ф., Скороход А.А., Соколович Е.Г., Яблонский П.К., Клинические рекомендации по тактике лечения больных легочным кровотечением.
4.
Коржева И. Ю. Лёгочные кровотечения. Комплексная диагностика и лечение. Автореферат диссертации на соискание ученой степени доктора медицинских наук. Москва. – 2012. – С. 3-4.
5.
Walker S, Hallifax R, Ricciardi S, Fitzgerald D, Keijzers M, Lauk O, Petersen J, Bertolaccini L, Bodtger U, Clive A, Elia S, Froudarakis M, Janssen J, Lee YCG, Licht P, Massard G, Nagavci B, Neudecker J, Roessner E, Van Schil P, Waller D, Walles T, Cardillo G, Maskell N, Rahman N. Joint ERS/EACTS/ESTS clinical practice guidelines on adults with spontaneous pneumothorax. Eur Respir J. 2024 May 28;63(5):2300797. doi: 10.1183/13993003.00797-2023. PMID: 38806203.
6.
Choi WI. Pneumothorax. Tuberc Respir Dis (Seoul). 2014 Mar;76(3):99-104. doi: 10.4046/trd.2014.76.3.99. Epub 2014 Mar 29. PMID: 24734096; PMCID: PMC3982243.
