Breast Cyst: Etiology, Classification, Clinic, Diagnosis and Treatment
Svetlana D.Surgical oncologist, MD
20 min read·October 15, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
A breast cyst is a non-tumor benign breast disease that is a round or oval mass with fluid contents originating from the terminal ductal lobular unit (TDLU). It is the most common cause of focal masses in the breast.
Breast cyst: 3D modelBreast cyst (sagittal section): 3D model3D animation: breast cyst
Cysts can be single or multiple and vary in size from nonpalpable microcysts detected only by instrumental diagnostic methods (ultrasound, mammography, MRI) to macrocysts that deform the contour of the breast and can be detected visually.
Breast cysts are part of a broader non-tumor pathologic process called fibrocystic mastopathy or fibrocystic breasts.
Cysts are the most common focal pathology of the breast. Their prevalence, according to different studies, varies from 37.5% to 70%. Cysts are most often diagnosed in the following groups of patients:
The underlying ethology of breast cysts is an imbalance of sex hormones. Increased estrogen levels and decreased progesterone levels trigger glandular hyperplasia and fibrosis.
These changes result in thickening of the epithelium, causing the developing terminal lobule to undergo involution. Disruption of the normal formation of the terminal duct-valve unit leads to obstruction of the excretory duct. Release of epithelial acinar fluid causes it to dilate with the subsequent formation of a fluid-filled cavity.
The main causes of breast cysts are:
Early onset and late termination of the menstrual cycle;
Nulligravida and late (after the age of 30) pregnancy;
Non-breastfeeding;
Endocrine disorders;
Ovarian inflammatory diseases;
A history of abortions.
Morphological presentation
Breast cysts have the following morphological features:
Enlarged glands lined with squamous epithelium consisting of cubic or columnar cells;
Epithelial layer may be thin or absent;
Moderate fibrosis and isolated inflammatory cells may be observed in the cyst wall;
Damage to the cyst causes an inflammatory reaction accompanied by the formation of foamy macrophages, cholesterol deposition and fibrosis.
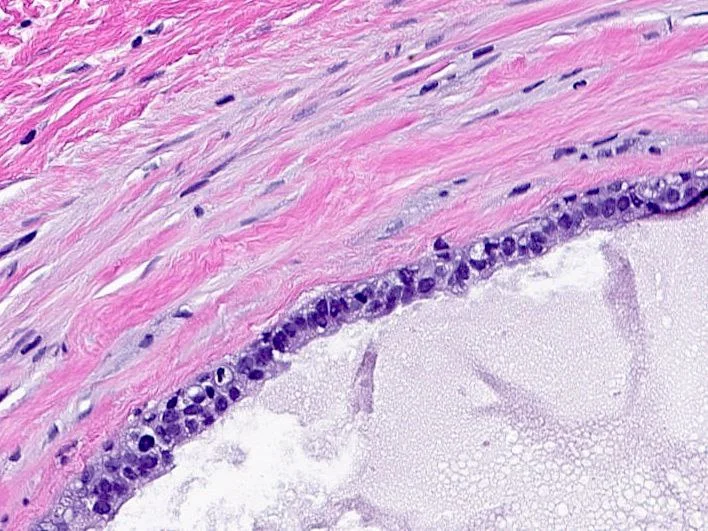
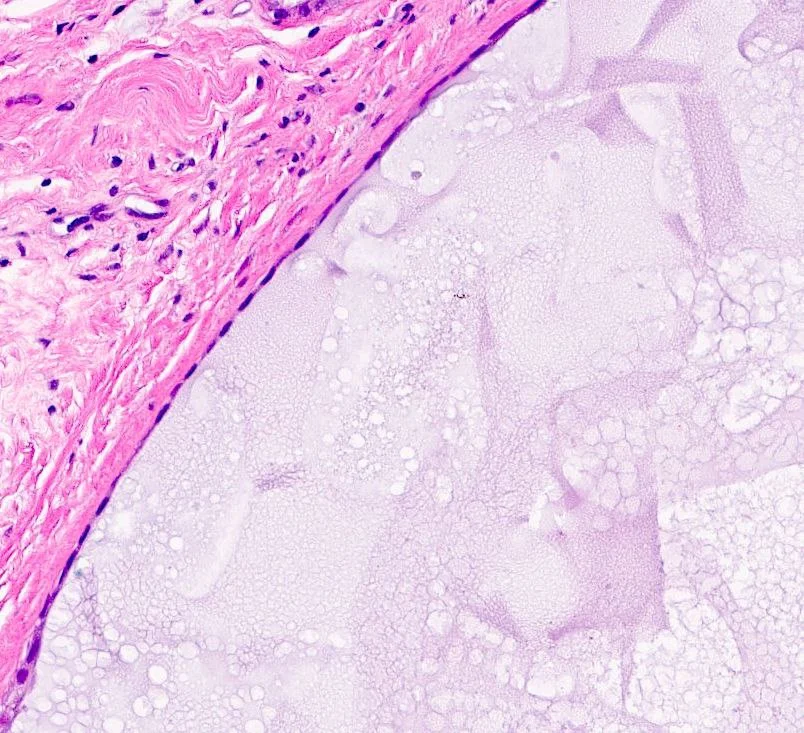
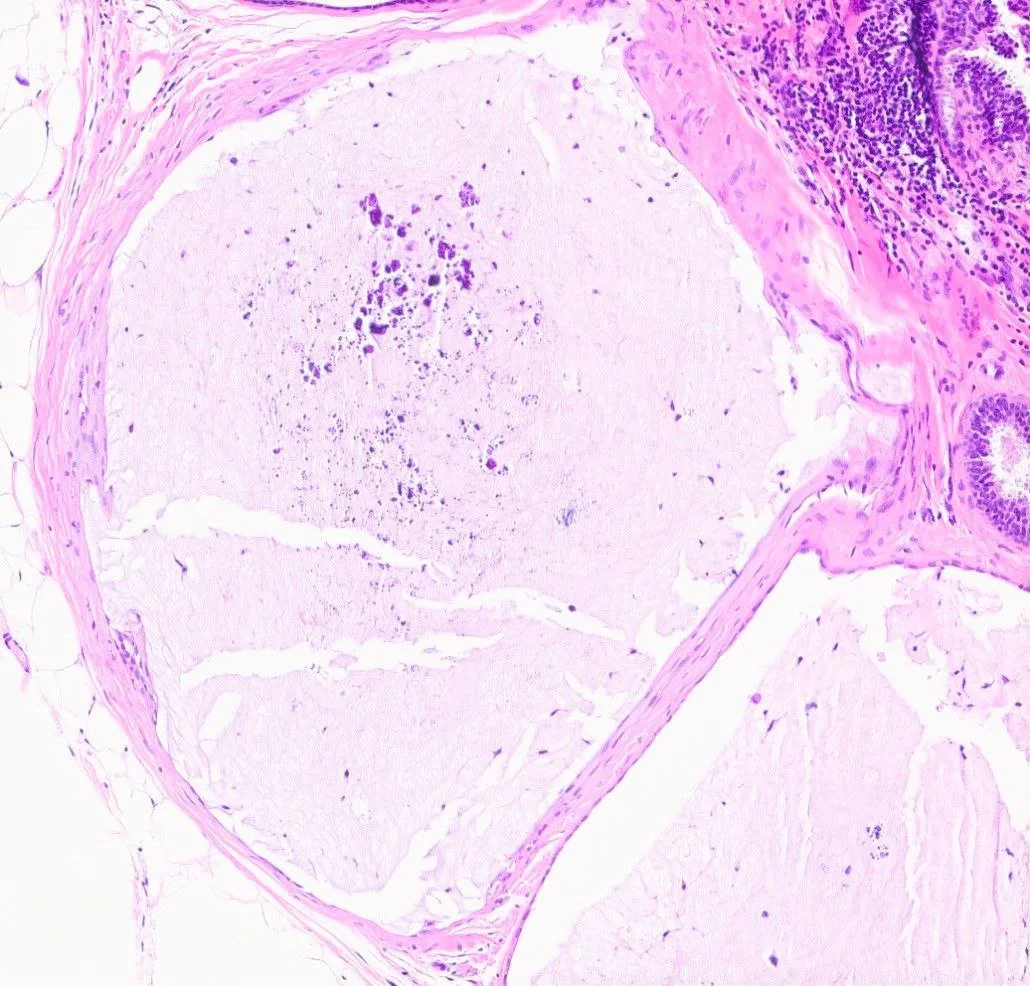
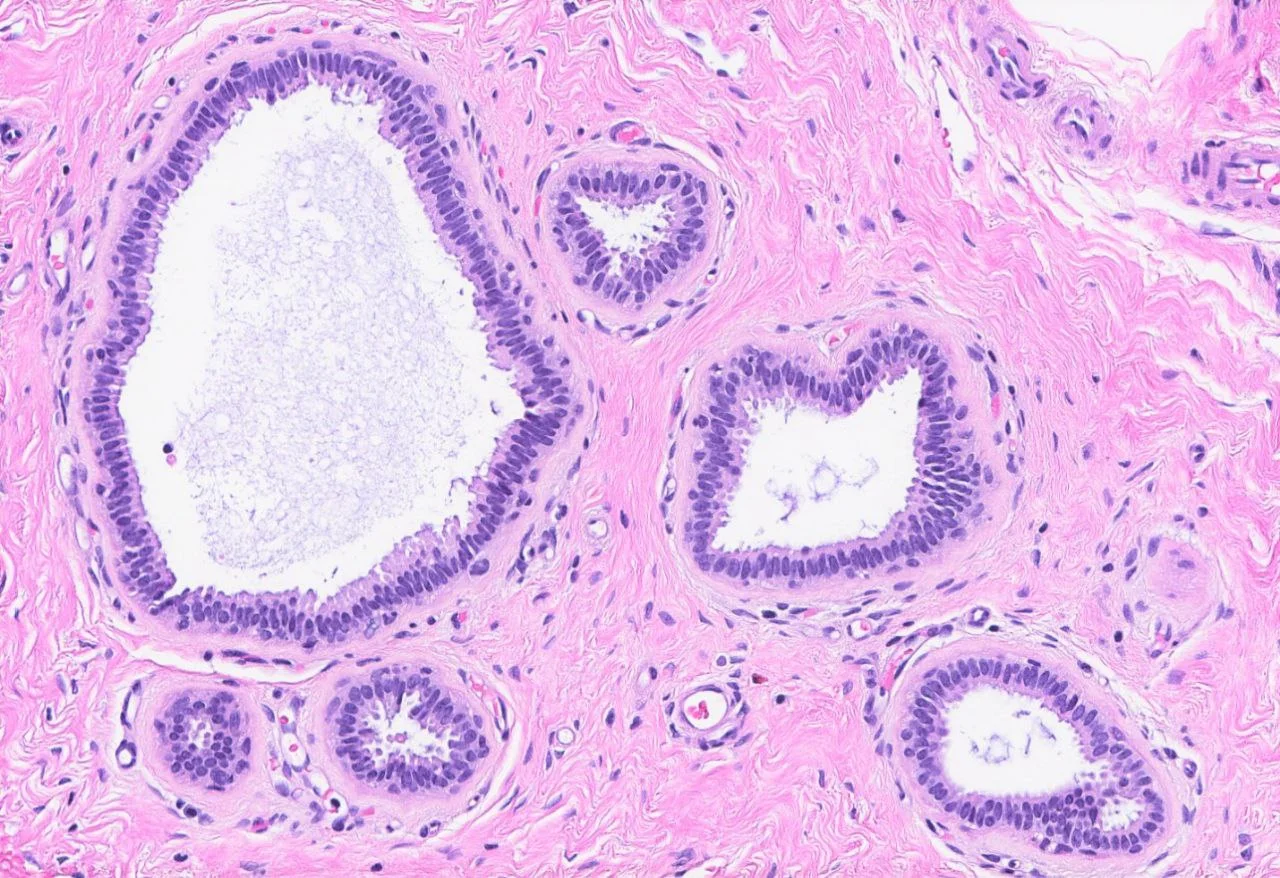
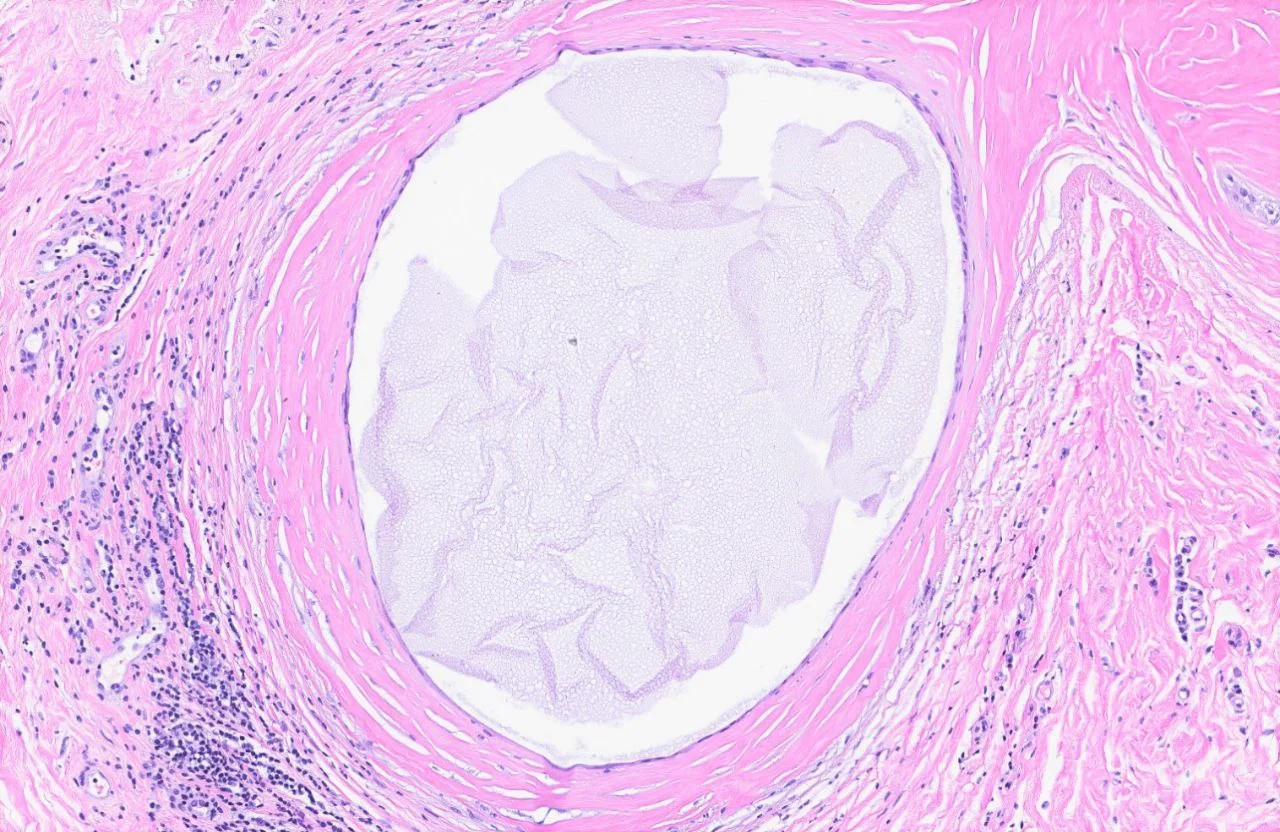
Below are images demonstrating the morphological presentation of a breast cyst. Author: Kristen E. Muller, D.O. Source: Pathology Outlines [9]:
Simple epithelial lining
Thickened epithelial lining
Absence of epithelial lining
A group of cysts lined by columnar epithelium
Fibrosis with surrounding inflammation
Classification of breast cysts
Three types of breast cysts are distinguished:
Simple cysts are characterized by a smooth-walled structure; they are completely filled with fluid, have no solid structures, and no Doppler signal is detected on US. Simple cysts account for about 90% of all cystic breast masses.
Complex cysts have a mixed structure (fluid and solid) and thick walls (more than 0.5 mm) in which blood flow signals can be detected. Frequently, such cysts contain septa in their structure. If such a mass is detected by ultrasound, a puncture (aspiration) biopsy is required to rule out breast cancer.
Complicated cysts are completely fluid-filled with suspended fluid or indistinct borders. They reveal no septa, no solid component and no blood supply on ultrasound but are often accompanied by inflammation. The probability of breast cancer is less than 2%; a puncture (aspiration) biopsy is performed for individualized indications.
Clinical presentation
The clinical presentation depends on the size of the mass. Cysts of small size, as a rule, have an asymptomatic course and are detected only by ultrasound. Larger cysts can lead to breast enlargement and deformity.
The main symptoms of breast cysts:
Palpable mass. The most common symptom is the presence of a round or oval mass in the breast, painless, easily displaced under the skin, and of dense elastic consistency. The cyst can increase and decrease in size depending on the phase of the menstrual cycle and hormone levels.
Soreness. The second most common symptom is localized (in the area of the cyst) or diffuse soreness in the breast before menstruation. The pain is aching, of insignificant or moderate intensity, and analgesic therapy is not required in most cases.
Nipple discharge. In rare cases, the presence of discharge from the nipple is noted, from light yellow to brown in color, with no distinct odor.
Diagnosis of breast cysts
Physical examination alone does not reliably distinguish cysts from other benign and malignant breast tumors.
1. Visual inspection
The visual inspection evaluates:
Symmetry, size and shape of breasts.
Skin color.
The presence of deformities in the contour of breasts or areolae.
Changes in the position of the nipples, nipple discharge.
Cysts of small sizes do not change the contour of the breast, whereas cysts of large sizes may deform the contours and lead to breast enlargement or asymmetry of breasts.
2. Palpation
Palpation of the breast is performed in standing and supine positions. Consecutively all quadrants of the gland are examined, starting from the upper-outer clockwise, then palpate axillary, supraclavicular and cervical lymph nodes on both sides. The areolae area is palpated separately.
On palpation:
Microcysts are usually not identified.
Larger cysts are defined as a round or oval mass, freely displaced relative to the skin, and painless or almost painless.
The skin over the mass is usually not hyperemic; there is no edema of the skin and subcutaneous tissue.
The consistency of the mass is most often described as dense elastic (“grape-like”), but can vary from soft elastic (“like a water balloon”) to dense (woody density).
Peripheral lymph nodes are not enlarged, are painless and may not be detectable by palpation.
Nipple discharge is infrequent, can be light yellow to brown in color, is not opalescent and has no distinct odor.
3. Ultrasound
Ultrasound is the main method of diagnosing breast masses due to its high efficiency, safety and accessibility.
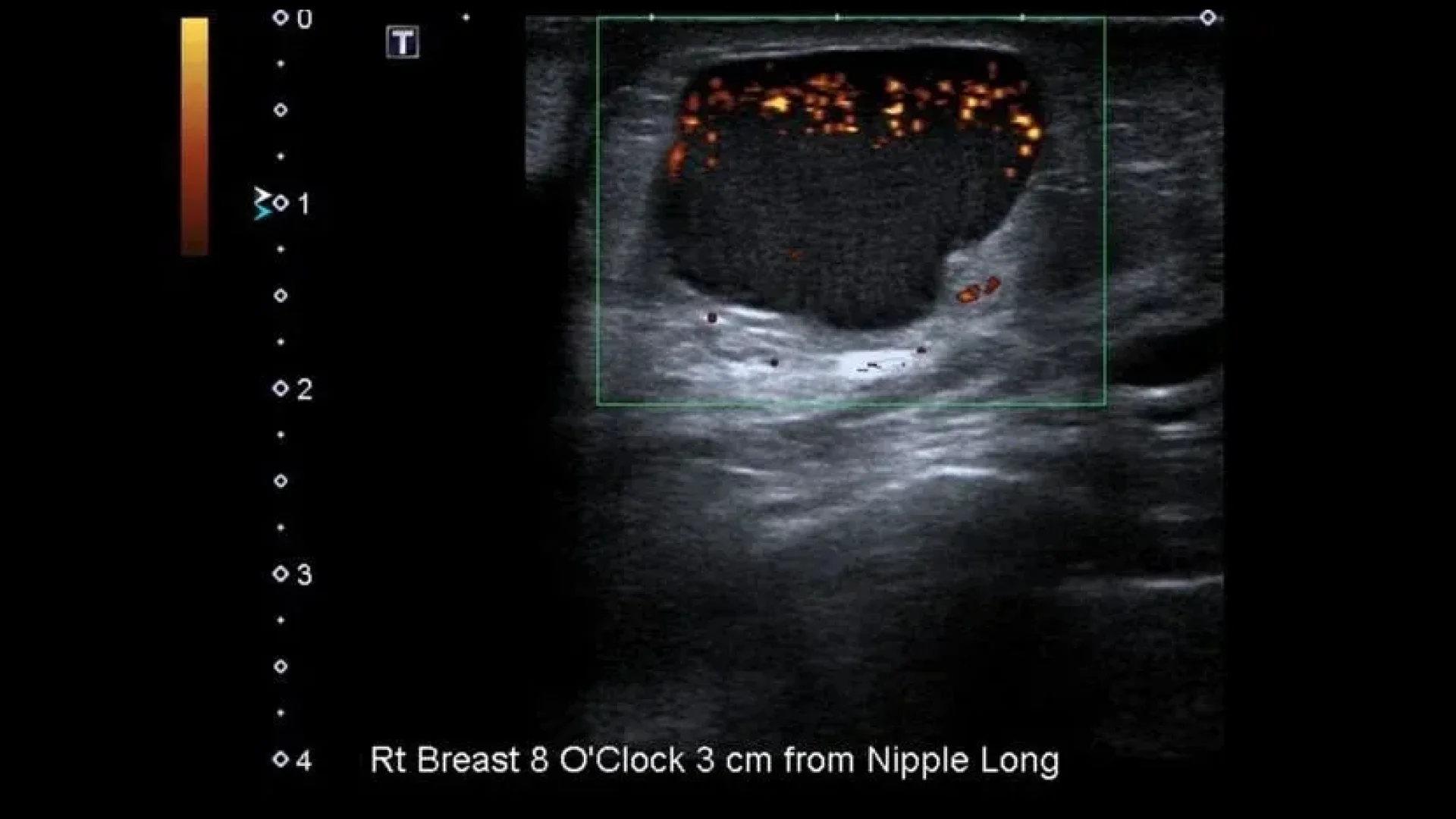
Simple breast cysts are characterized by the following ultrasound signs:
The horizontal dimension is larger than the vertical dimension;
The mass is non-echoic and homogeneous;
The walls are hyperechoic, thin and smooth;
Dorsal signal amplification;
Lack of blood flow within the mass.
Ultrasound with Doppler ultrasonography of a simple large breast cyst. Author: Henry Knipe. Source: Radiopaedia. Simple Breast Cyst [12]
Complex cysts are characterised by:
The horizontal dimension is larger than the vertical dimension;
The mass is non-echoic, with the presence of solid-walled structures, possibly the presence of septa;
Dorsal signal amplification;
Possible blood flow signals.
Complicated cysts are characterised by:
The horizontal dimension is larger than the vertical dimension;
The mass is non-echoic with the presence of finely dispersed suspension in the cavity;
The walls are hyperechoic, irregular and thickened;
Dorsal signal amplification.
Breast ultrasound: complex cyst (left) and complicated cyst (right). Source: ScienceDirect. Complex cystic breast masses in ultrasound examination [13]
In order to standardise the diagnostic description, the BI-RADS system is currently used. Each focal mass is described with regard to shape, orientation, contours and echo structure; it should be further categorised into a category ranging from BI-RADS 0 (study is uninformative, requires follow-up examination using other diagnostic methods) to BI-RADS 6 (morphologically confirmed cancer). Breast cysts correspond to BI-RADS 2 (benign mass) and BI-RADS 3 (probably benign mass) categories.
4. Mammography
Mammography is uninformative in the diagnosis of cystic breast masses. In the presence of complex and complicated breast cysts, according to ultrasound, mammography may be prescribed as a clarifying method for differential diagnosis with breast cancer.
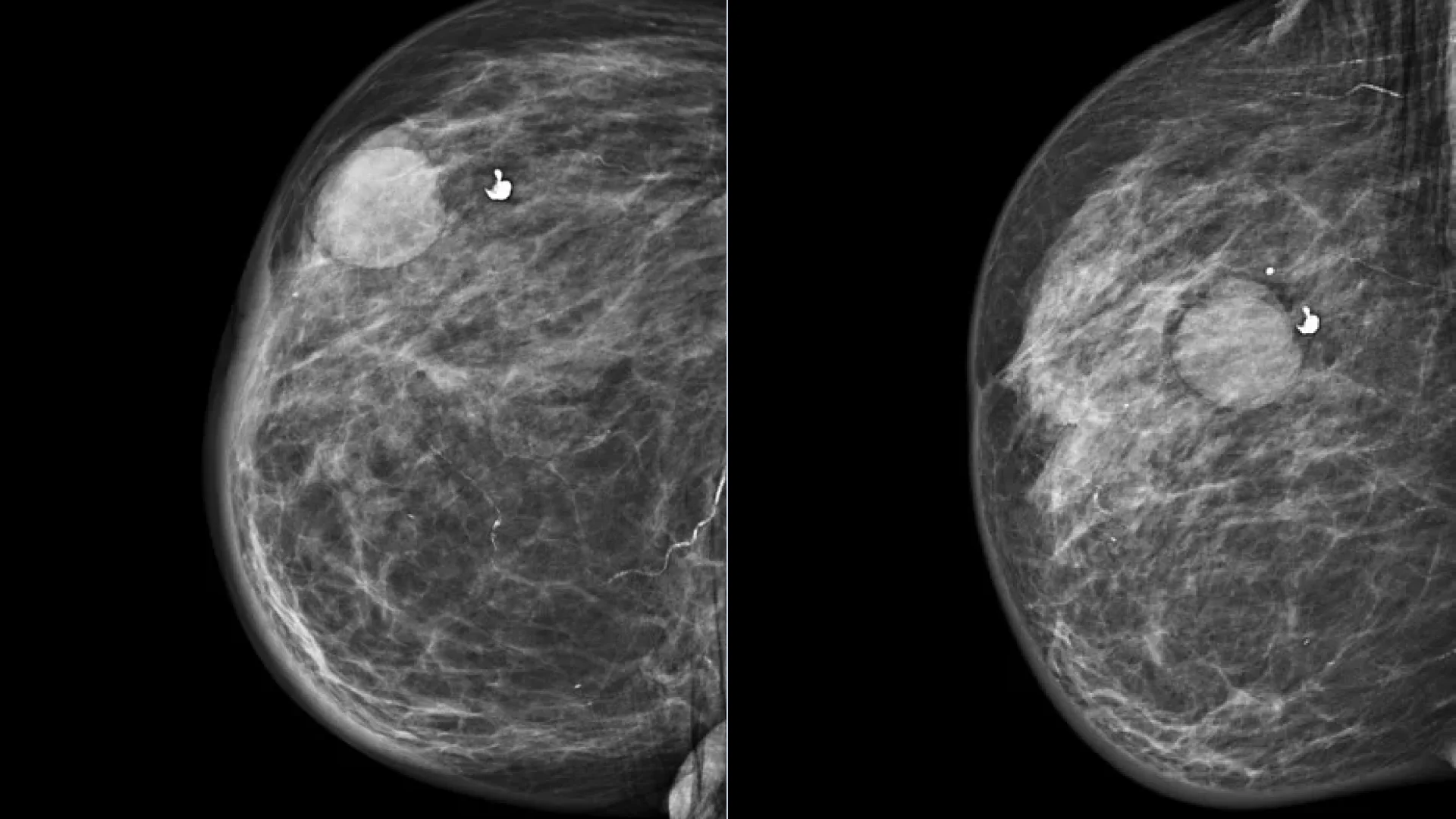
Radiologically, large cysts are defined as round or oval masses of homogeneous structure with smooth, clear contours; small cysts are not radiologically defined. In patients of reproductive age, mammography is uninformative due to an evident glandular component in the structure of breast; therefore, this diagnostic method is more often used in postmenopausal patients.
Mammography of the right breast in two projections: breast cyst. Author: Henry Knipe. Source: Radiopaedia. Simple Breast Cyst [12]
5. Magnetic resonance imaging (MRI)
Magnetic resonance imaging in the diagnosis of breast cysts is not the method of choice and is of a clarifying nature when malignant neoplasms are suspected. The cyst on tomograms is visualised as a round or oval mass with clear contours, iso- or hypointense with respect to the breast parenchyma on T1-weighted images and hyperintense on T2-weighted images. When contrast agent is injected, the cyst appears as a filling defect, sometimes with widening of the margins.
MRI of a breast cyst: T1-weighted image (left) and T2-weighted image (right). Source: Аmerican journal of roentgenology [8]
6. Fine-needle aspiration biopsy (FAB)
Fine-needle aspiration biopsy (FAB) is a diagnostic procedure that is performed to obtain the contents of a cyst for subsequent cytological examination. The procedure does not require special preparation, is performed on an outpatient basis and does not require anesthesia. Relative contraindications to performing FAB are infectious and inflammatory diseases, as well as blood coagulation disorders.
Technique: after skin preparation with antiseptic, under ultrasound control, a biopsy of the mass with a fine needle with aspiration of the contents is performed. After the procedure is completed, the skin is retreated with an antiseptic solution, and an aseptic dressing/patch is applied for 30–40 minutes.
Complications of the procedure:
Subcutaneous hematoma at the injection site;
Localized breast soreness in the area of the injection;
Local inflammation of soft tissues in the area of injection.
Complications after FAB are rare, usually do not require treatment and resolve on their own within a few days.
7. Core needle biopsy
Core needle biopsy is an invasive diagnostic procedure aimed at tissue sampling followed by histological examination. It is used to exclude malignant breast tumors in cases when non-invasive diagnostic methods and FAB are uninformative. Unlike fine-needle aspiration biopsy, this procedure is painful and requires the use of local anesthesia.
Technique: after skin preparation with antiseptic solution, infiltration anesthesia of the skin and soft tissues is performed. Under ultrasound control, several columns of tissue are taken with a special instrument — trephine. After the procedure is completed, the wound is treated with an antiseptic solution, then an aseptic dressing is applied.
Complications after core needle biopsy are similar to those after FAB but are more common due to the more traumatic procedure. In addition, there may be allergic reactions to the anesthetic injection.
8. Excisional biopsy
Excisional biopsy is the surgical removal of a breast mass. It is used very rarely if all other diagnostic methods are uninformative and do not allow the exclusion of breast cancer. It is performed in hospital conditions under local or general anaesthesia (the type of anaesthesia is determined individually depending on the complexity of the manipulation and the patient’s contraindications to any type of anaesthesia). In aseptic conditions, a complete removal of the mass is performed within healthy tissues with subsequent histological examination of the removed material.
Complications:
Bleeding from the postoperative wound;
Inflammation of the postoperative wound;
Allergic reactions to anesthetics.
The diagnosis of a simple breast cyst is usually not difficult with ultrasound. In doubtful cases, aspiration biopsy is indicated to clarify the diagnosis.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Treatment of breast cysts
Breast cysts usually do not require treatment. Both non-surgical and surgical treatments are possible if symptoms are severe.
Aspiration of cyst contents during aspiration biopsy can reduce the size of the mass and symptoms of the disease. In some cases, it is possible for the cyst to disappear completely after aspiration of its contents.
Non-surgical treatment
Medical therapy consists of prescribing combined oral contraceptives or anti-estrogenic agents (tamoxifen). However, given the high risk of side effects, such a therapy is recommended only in case of a severe course of the disease. If cysts appear on hormone replacement therapy in the menopausal period, it is recommended to withdraw such a therapy.
Surgical therapy
Surgical treatment is used when the risk of breast cancer is high. Usually a sectoral resection of the breast is performed, followed by histological examination of the removed material.
FAQ
1. Why do breast cysts appear, and what are their causes?
The main cause is hormonal imbalance (increased estrogen and decreased progesterone), which leads to tissue overgrowth and blockage of the mammary duct. Factors that trigger this process include the individual pattern of the menstrual cycle, past nulligravida and non-breastfeeding, endocrine and inflammatory gynecological diseases, as well as a history of abortions.
2. What are the signs and symptoms of a breast cyst?
Most often cysts are asymptomatic. If signs are present, the main one is a palpable round or oval mass that is painless and easily displaced. An aching pain in the area of the cyst or in the whole breast before menstruation is also a characteristic symptom. In rare cases, there may be a light yellow to brown colored discharge from the nipple.
3. Is a breast cyst dangerous, and can it progress to cancer?
A simple cyst is a non-tumour, benign mass that does not progress to cancer. Complex cysts with a solid component are dangerous, as they require a biopsy to rule out a malignant process. Complicated cysts have a very low risk of malignisation (less than 2%).
4. Can a breast cyst go away on its own?
Yes, cysts can shrink in size on their own depending on the phase of the menstrual cycle and sometimes disappear completely. This process is associated with hormonal fluctuations. Complete disappearance is also possible after aspiration (emptying) of the cyst contents.
5. How to know that a breast cyst ruptured?
Cyst rupture, although infrequent, manifests as acute localized inflammation. The main symptoms are sudden and often intense pain in the area where the cyst was located, the appearance of a lump, swelling and possible redness of the skin. The clinical presentation may resemble mastitis.
6. What are the contraindications for breast cysts?
There are no direct absolute contraindications, but there are recommendations. The main thing is caution with hormonal treatment; if cysts appear on hormone replacement therapy (HRT), it is recommended to withdraw it. It is also advised to avoid trauma to the breast and intense heat procedures (hot compresses) on the breast area, as this can lead to inflammation.
7. What is the difference between a cyst and a breast fibroadenoma?
These are two different masses, benign in nature. A cyst is a fluid-filled cavity within a process called fibrocystic breast. A fibroadenoma is a solid (tissue) tumor composed of glandular and connective tissue. They differ on palpation (cysts can be soft or elastic; fibroadenoma is dense and “rubber-like”), the age of patients (cysts are more common after 35; fibroadenomas — in young women aged 15–35) and, most importantly, the ultrasound pattern, which clearly shows the difference in their structure.
8. How fast does a breast cyst grow?
The rate of cyst growth is not constant. Its size is directly related to the hormonal profile and can increase and decrease cyclically during one menstrual cycle (e.g., increase before and decrease after menstruation). Some cysts can remain stable for years, while others can quickly fill with fluid in a couple of weeks. It is not growth in the sense of cell division but the accumulation of secretion.
A. V. Anisimov (А. В. Анисимов). BI-RADS system for ultrasound: description, classification, illustrations (Система BI-RADS для УЗИ: описание, классификация, иллюстрации). \[Article in Russian] SonoAce Ultrasound Journal No. 29, 2016. (Журнал SonoAce Ultrasound № 29, 2016 г.) \[In Russian] [Electronic resource].
https://www.medison.ru/si/art434.htm
5.
A. N. Sencha. Breast ultrasound. Step by step. From simple to complex. (А. Н. Сенча. Ультразвуковое исследование молочных желез. Шаг за шагом. От простого к сложному.) \[Book in Russian] 2nd edition.
6.
A. N. Sencha, Yu. V. Bikeev. Ultrasound examination of mammary glands. Atlas. (Сенча А. Н., Бикеев Ю. В. Ультразвуковое исследование молочных желез. Атлас.) \[Book in Russian]
7.
S. K. Ternovoy, A. B. Abduraimov. Radiation mammology. (С. К. Терновой, А. Б. Абдураимов. Лучевая маммология.) \[Book in Russian]
8.
American journal of roentgenology. [Electronic resource].
Clinical role of breast MRI now and going forward (D. Leithner, G.J. Wengert, T.H. Helbich, S. Thakur, R.E. Ochoa-Albiztegui, E.A. Morris, K. Pinker). [Electronic resource].