Brain Tumors: Etiology, Classification, Symptoms, Diagnosis, and Treatment
Artemiy G.Neuro-oncological surgeon, MD
22 min read·December 23, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Brain tumors are a heterogeneous group of neoplasms that arise from various cell types within the central nervous system (CNS). They may also occur as metastases from other primary malignancies, most commonly cancers of the lung, breast, or kidney, as well as melanoma. Depending on their location and pattern of growth, brain tumors can cause both generalized (diffuse) brain symptoms and focal neurologic deficits. These manifestations result from compression and/or infiltration of brain tissue and from increased intracranial pressure (ICP).
In a minority of cases, they are associated with hereditary cancer syndromes, such as neurofibromatosis or Li–Fraumeni syndrome.
The only well-established environmental risk factor is exposure to ionizing radiation, especially at high doses.
Epidemiology
The incidence of primary brain and CNS tumors is approximately 25 cases per 100,000 population per year. When both primary and metastatic brain tumors are considered together, the annual incidence exceeds 45 cases per 100,000.
Around 30% of primary (non-metastatic) brain tumors are malignant; the remainder are benign or of low malignant potential.
In patients younger than 40 years, primary brain tumors predominate and are often low-grade.
The most common primary tumors in adults are meningiomas (more than 90% of which are benign) and glial tumors (over 80% of which are malignant).
After the age of 40, metastatic brain tumors (more than 50%) and glioblastoma become the most common brain tumors. Glioblastoma is the most aggressive primary brain tumor and accounts for roughly half of all glial tumors.
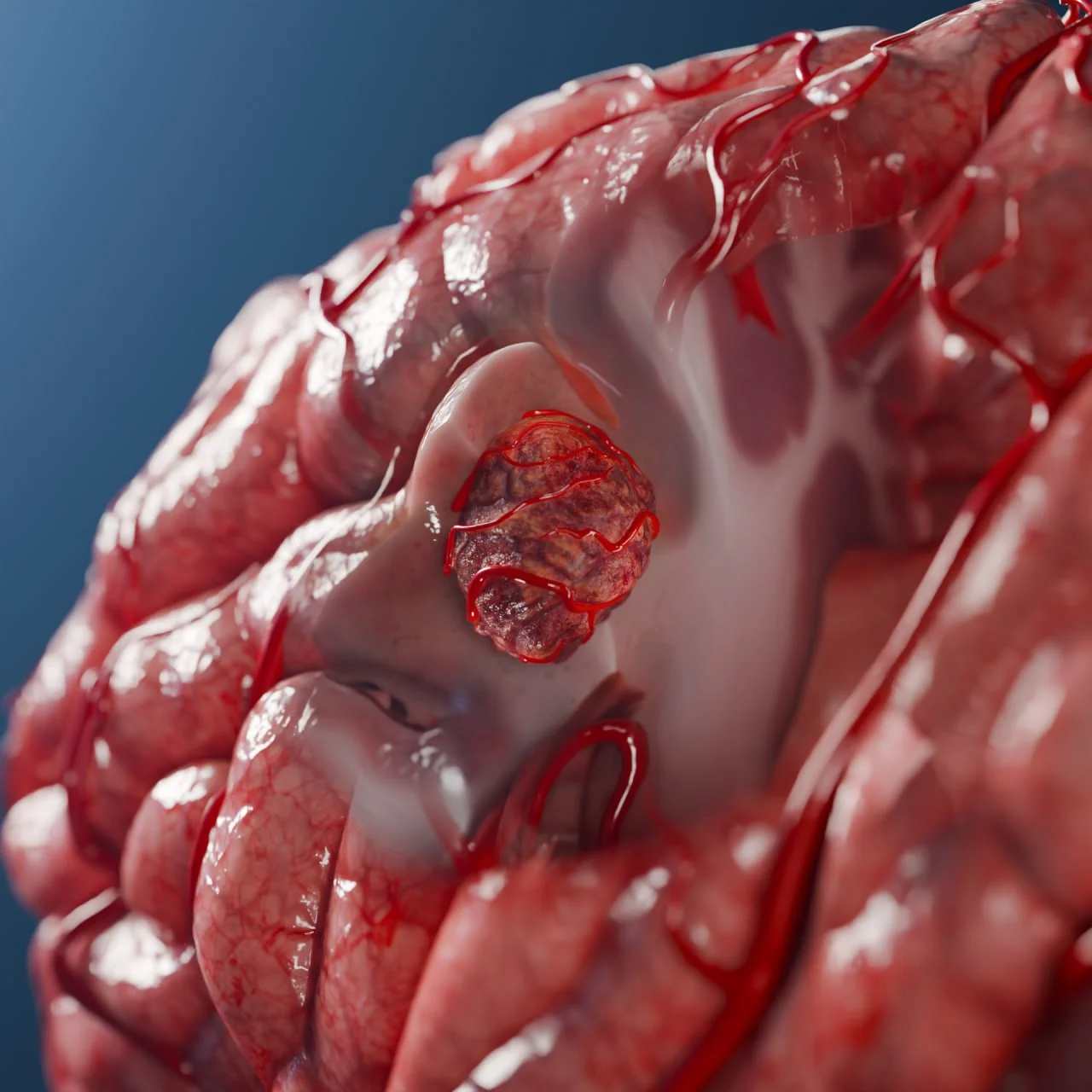
Kidney cancer metastasis in the left cerebral hemisphere: 3D model
In children,CNS tumors are one of the leading causes of cancer-related mortality. Gliomas are the most common histologic tumor group in the pediatric population. The most frequent subtype is benign pilocytic astrocytoma, with a 5-year survival rate >90%. They are followed in frequency by medulloblastomas, which are the most common malignant embryonal CNS tumors in children. In standard-risk cases, 5-year survival is approximately 60–80%. Other important pediatric brain tumors include ependymomas, glioblastomas, craniopharyngiomas, and intracranial germ cell tumors.
Anatomy
By Location Relative to the Tentorium Cerebelli
In relation to the tentorium cerebelli, brain tumors are classified into supratentorial and infratentorial types.
Supratentorial tumors
Supratentorial tumors(“above the tentorium”) are located superior to the tentorium cerebelli, in the cerebral hemispheres, basal ganglia, optic chiasm, and the lateral and third ventricles. They account for approximately 70–80%of tumors in adults.
Examples include:
Glioblastoma,
Astrocytoma,
Oligodendroglioma,
Pituitary adenoma,
Frontal or parietal meningioma, and others.
Infratentorial Tumors
Infratentorial tumors (“below the tentorium”) are located in the posterior cranial fossa: the cerebellum, brainstem, and the fourth ventricle. They predominate in children and account for up to 60–70% of pediatric brain tumors.
Examples include:
Cerebellar pilocytic astrocytoma,
Medulloblastoma,
Fourth ventricular ependymoma,
Vestibular schwannoma (acoustic neuroma),
Cerebellopontine angle meningioma,
Hemangioblastoma, and others.
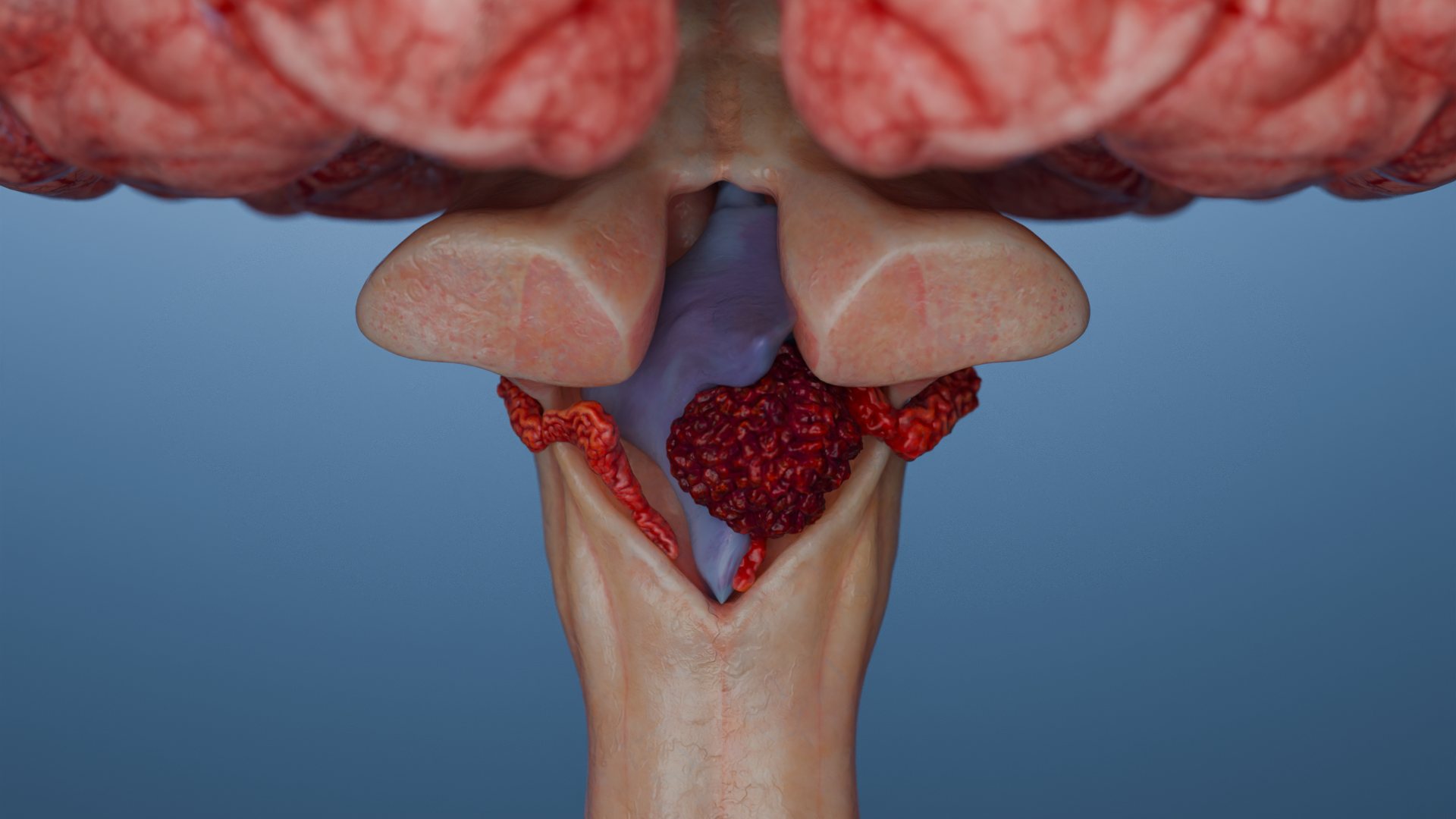
Infratentorial Ependymoma — 3D Model3D-Animation: Infratentorial Ependymoma
By Location Relative to the Brain Parenchyma
Based on their relationship to the brain parenchyma (the “axial” or central CNS tissue), tumors are classified as extra-axial or intra-axial.
These terms reflect not only anatomical location, but also characteristic growth patterns and usual treatment approaches. Extra-axial tumors are usually benign and compress the brain from outside, whereas intra-axial tumors tend to be infiltrative and malignant.
Extra-Axial Tumors
Extra-axial tumors arise outside the brain parenchyma but within the cranial cavity. They typically compress the brain rather than infiltrate it.
Examples include:
Tumors of the meninges (e.g., meningioma),
Tumors of the cranial nerves (e.g., schwannoma),
Tumors of the skull base (e.g., chordoma), and others.
Intra-Axial Tumors
Intra-axial tumors arise within the brain tissue itself, most commonly from glial cells (astrocytes, oligodendrocytes, ependymal cells). Examples include:
Glioblastoma,
Astrocytoma,
Ependymoma, and others.
Classification of Brain Tumors
The 2021 World Health Organization Classification of Tumors of the Central Nervous System (WHO CNS 2021) places major emphasis on molecular and genetic characteristics in addition to traditional histology.
The system uses a three-level approach:
Histology: cell morphology and overall tumor architecture.
Immunohistochemistry: expression of specific proteins (e.g., GFAP, p53, ATRX, Ki-67).
Molecular markers: genetic and chromosomal alterations such as IDH1/2, 1p/19q, TP53, ATRX, H3, BRAF, CDKN2A/B, EGFR, TERT, and others.
In gliomas, several key markers are routinely assessed to refine the diagnosis, estimate prognosis, and guide therapy:
IDH1/2 mutations: the presence of an IDH mutation is generally associated with a more favorable prognosis.
1p/19q codeletion: characteristic of oligodendroglioma and associated with better outcomes.
ATRX status: loss of ATRX expression supports a diagnosis of astrocytoma rather than oligodendroglioma.
TP53 mutations: often correlate with a less favorable prognosis.
MGMT promoter methylation: predicts a better response to temozolomide.
VEGF overexpression: may support the use of anti-angiogenic agents such as bevacizumab in selected cases.
The shift toward a molecularly based classification allows more precise tumor stratification and better prognostication. It also supports a more individualized treatment strategy, with tailored chemotherapy and radiotherapy and more rational decisions about surgery and adjuvant treatment.
Clinical Manifestations of Brain Tumors
General (diffuse) brain symptoms:
Headache: occurs in about 50–70% of patients. It is often bilateral and dull and tends to worsen with coughing, bending forward, or at night and in the early morning.
Seizures: seen in 50–80% of patients with primary brain tumors, especially slow-growing low-grade gliomas and metastases. Seizures are often focal in onset.
Cognitive and behavioral changes: apathy, memory impairment, and mood disturbances are common.
Signs of increased intracranial pressure (ICP): the classic triad consists of headache, nausea and vomiting, and papilledema (optic disc swelling).
Focal neurologic symptoms:
Weakness of the face or limbs: typically with involvement of the motor cortex; in some cases, deficits may improve temporarily with glucocorticoid therapy due to reduction of edema.
Sensory disturbances: sensory loss or abnormal sensations that do not follow dermatomal patterns.
Aphasia: difficulty producing or understanding speech, usually with tumors in the dominant hemisphere, particularly in Broca’s or Wernicke’s areas.
Visual disturbances: visual field defects (e.g., hemianopia) with involvement of the visual pathways, as well as diplopia or reduced visual acuity.
Personality and behavioral changes: especially with frontal lobe tumors.
In children, symptoms depend on age, tumor location, and tumor biology. Presentations are often nonspecific, which makes early diagnosis challenging.
Indications for neuroimaging (MRI/CT) in children with suspected CNS tumor:
Persistent headache lasting more than 4 weeks, especially if accompanied by morning vomiting, altered consciousness, or occurring in children younger than 4 years.
New or progressive neurologic symptoms (such as seizures, weakness, coordination difficulties, or visual disturbances).
Strabismus, reduced visual acuity, or papilledema.
Regression of motor milestones or gait disturbance.
Progressive macrocephaly (increasing head circumference), particularly when present together with other neurologic symptoms.
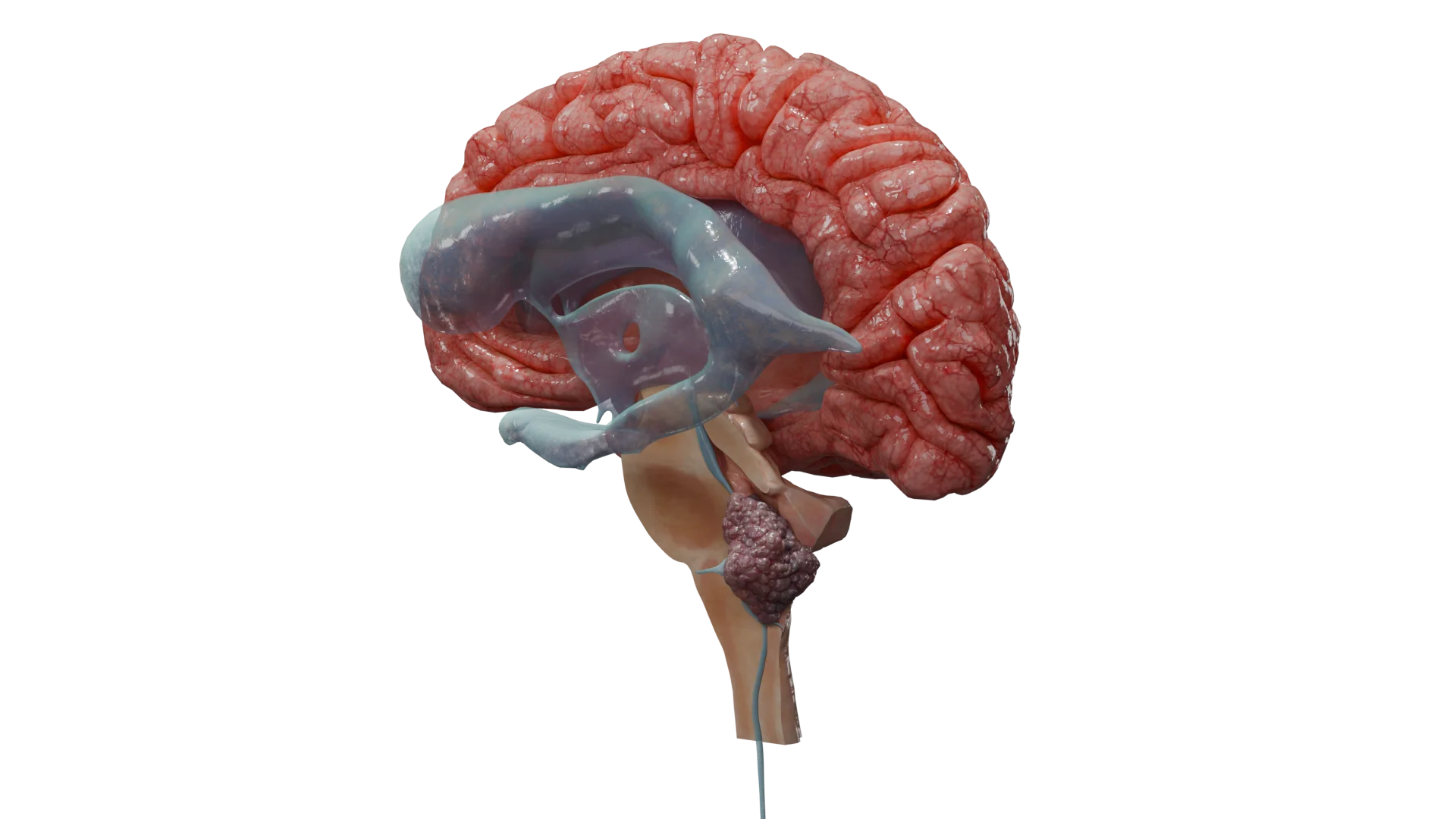
3D-Animation: Choroid Plexus Papilloma
Diagnosis of Brain Tumors
Diagnosis is based on a combination of modern neuroimaging techniques and histologic and molecular confirmation. Additional investigations are used when the etiology is unclear or the clinical course is atypical.
Neuroimaging
Contrast-enhanced MRI of the brain is the imaging modality of choice for detecting and characterizing brain tumors. It provides information on tumor size, location, intracranial spread, vascularity, necrosis, and the extent of infiltration.
CT of the head is used in emergency settings or when MRI is contraindicated.
Typical imaging patterns include:
Glioblastoma: heterogeneous contrast enhancement, central necrosis, surrounding edema, and irregular borders.
Low-grade gliomas: hyperintense lesions on T2/FLAIR, often without contrast enhancement, with an infiltrative growth pattern.
Metastases: usually round, well-demarcated lesions, often multiple, with marked peritumoral edema.
Meningioma: extra-axial mass attached to the meninges (skull base, convexity, falx, or tentorium), with homogeneous contrast enhancement.
Primary CNS lymphoma: strong homogeneous enhancement, often with restricted diffusion on DWI and a typical periventricular or deep location.
Biopsy
Stereotactic biopsy or open surgical biopsy is performed to confirm the diagnosis and obtain tissue for histologic and molecular profiling (e.g., IDH status, 1p/19q codeletion, MGMT, TP53, BRAF, H3K27, and others).
In suspected CNS lymphoma, glucocorticoids should be withheld before biopsy whenever clinically feasible. They can induce rapid, temporary tumor regression and thus obscure the diagnosis.
Additional diagnostic methods
PET-CT, MR spectroscopy, and MR perfusion: used when the nature of a lesion is uncertain, for example to distinguish tumor from abscess, demyelinating disease, or radiation necrosis.
Lumbar puncture: indicated in leptomeningeal involvement, suspected meningitis or encephalitis, progressive multifocal leukoencephalopathy, or CNS lymphoma. It is contraindicated in patients with marked intracranial hypertension or mass effect.
Differential diagnosis
The goals of differential diagnosis are:
To distinguish tumors from non-neoplastic processes (infection, demyelination, vascular lesions).
To determine whether a lesion is primary or metastatic.
To clarify histologic and molecular subtype and tumor grade.
To exclude treatment-related complications such as radiation necrosis or abscess.
Aneurysm
Sudden headache, on CT/MRI with contrast — vascular mass, on angiography — dilated artery, subarachnoid hemorrhage.
Stroke
Sudden onset, focal neurologic deficit, ischemic area visible on DWI/ADC MRI (diffusion restriction), more often localized across vascular basins.
Encephalitis
Subacute onset, fever, confusion, and seizures — no focal mass. On MRI, changes are usually diffuse, often in the temporal lobes (e.g., in herpetic encephalitis), with no mass effect.
Primary brain tumor
Gradual onset, focal neurologic symptoms, seizures, headache. MRI usually reveals an infiltrative or solid mass with surrounding edema, mass effect, and heterogeneous contrast enhancement.
Brain metastasis
Metastatic lesions are often multiple and located at the gray–white matter junction, surrounded by marked vasogenic edema and showing ring-like enhancement. In most patients, there is a known history of systemic malignancy.
CNS lymphoma
MRI typically shows a homogeneously enhancing lesion in deep, periventricular regions, particularly in immunosuppressed patients.
High diffusion restriction (DWI+), possible rapid regression after steroids, so it’s important to avoid them before biopsy.
Brain abscess
Often fever, leukocytosis, and a focus of infection (otitis media, sinusitis, bacteremia). On MRI, it can mimic a tumor, but typically shows a ring-enhancing lesion with restricted diffusion on DWI. MR spectroscopy reveals specific amino acids/metabolites.
Radiation necrosis
This complication occurs months to years after radiotherapy and can mimic tumor recurrence. Distinguished by MR perfusion and PET (necrosis means hypoperfusion, hypometabolism), may decrease on steroids.
Multiple sclerosis
Young age, multifocal lesions in the white matter, FLAIR-hyperintense without mass effect or contrast; clinical course is recurrent, with remissions, often in the young.
Cavernous sinus thrombosis
Acute onset with headache (often unilateral), eyelid swelling, ophthalmoplegia, and decreased vision. MRI/MR venography reveals thrombus in the venous sinuses. There is often infection of the facial, nasal, and sinus areas.
Cluster headache
Sharp pain around the eye, lacrimation, rhinorrhea, lasting minutes, recurring in series, not accompanied by neurologic deficit. No structural changes on the MRI.
Idiopathic hydrocephalus
Often in the elderly, a triad of symptoms (gait disturbance, dementia, urinary incontinence), there may be headache and nausea, on MRI ventricular dilation without focal masses.
Metabolic disorders
Causes diffuse rather than focal symptoms (confusion, seizures, tremors), with no focal mass on MRI. General tests (glucose, sodium, liver enzymes, creatinine, urea, etc.) help identify the cause.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Treatment of Brain Tumors
Glucocorticoids
Glucocorticoids are used to treat symptoms related to brain edema and increased intracranial pressure. A common regimen is dexamethasone 8–16 mg per day, often administered as 4 mg every 6 hours.
Prolonged use should be avoided because it increases the risk of complications such as infection, hyperglycemia or diabetes, and osteoporosis. In addition, long-term steroid therapy has been associated with reduced survival in patients with glioblastoma.
In suspected CNS lymphoma, glucocorticoids should ideally be withheld until after biopsy, as steroids can cause temporary tumor regression and interfere with histologic diagnosis.
Antiepileptic drugs
Antiepileptic drugs are indicated in patients who have experienced seizures. Levetiracetam is commonly used as first-line therapy.
Prophylactic treatment before surgery is considered on an individual basis.
Surgical therapy
Biopsy, subtotal resection, or gross-total resection is performed when the tumor is surgically accessible, causes significant symptoms, or when the diagnosis is uncertain. Surgery is also indicated in acute decompensation due to mass effect.
Modern tools such as preoperative MR tractography, neuronavigation, intraoperative MRI and ultrasound, operating microscopes, and fluorescence-guided surgery significantly improve the safety and completeness of tumor resection.
Radiotherapy and systemic antitumor therapy
Radiotherapy after surgery can approximately double survival in patients with malignant gliomas.
Stereotactic radiosurgery (SRS) or stereotactic radiotherapy is used for small, well-defined, deep-seated, or radioresistant tumors and often achieves durable local control.
Radiotherapy and systemic therapy are selected according to tumor type:
Glioblastoma: maximal safe resection followed by radiotherapy with concurrent and adjuvant temozolomide. Median survival is typically 12–18 months.
Primary CNS lymphoma: biopsy followed by high-dose methotrexate-based chemotherapy, with or without radiotherapy.
Brain metastases: SRS or open surgery (craniotomy) for solitary or limited lesions, sometimes combined with neoadjuvant or adjuvant SRS, plus targeted therapy or immunotherapy when appropriate. For multiple or inoperable metastases, SRS or whole-brain radiotherapy may be used.
Meningiomas: observation for small, asymptomatic tumors; surgery and/or radiotherapy (including SRS) for symptomatic or growing lesions.
Schwannomas and neurofibromas: observation, microsurgical removal, or SRS depending on size, growth, and symptoms.
Systemic treatment options, including targeted therapies and immuno-oncologic agents, are expanding for both benign and malignant CNS tumors. Nevertheless, surgical resection and radiotherapy remain the cornerstone of treatment for most brain tumors.
Special considerations in pediatric CNS tumors
Surgical resection is usually the first-line treatment, except in diffuse intrinsic brainstem gliomas and some optic pathway tumors. CSF shunting procedures are often required to control intracranial hypertension when hydrocephalus is present.
Radiotherapy is used according to tumor type and age. It is generally avoided or minimized in children younger than 3 years whenever possible because of the risk of long-term neurocognitive impairment.
Chemotherapy is combined with surgery and radiotherapy, especially in children older than 3 years with embryonal tumors (such as medulloblastoma), ependymoma, and certain gliomas. In infants and very young children, chemotherapy is often used to delay or replace radiotherapy in order to reduce late toxicity.
Modern management of CNS tumors relies on a multidisciplinary approach, molecular stratification, and individualized treatment planning.
Advances in radiotherapy and systemic therapy (including targeted agents and immunotherapy) offer hope for better long-term outcomes.
Early diagnosis, an optimal surgical strategy, appropriate adjuvant treatment, and comprehensive rehabilitation are all critical to improving prognosis and quality of life.
FAQ
1. What causes a brain tumor, and can it be inherited?
Most brain tumors arise sporadically, that is, without a clearly identifiable hereditary cause. In a minority of cases, they are associated with inherited genetic syndromes, such as neurofibromatosis. The main established environmental risk factor is exposure to ionizing radiation.
2. How do brain tumors usually present, and do the first symptoms differ between men and women?
Brain tumor symptoms do not differ between men and women. In both sexes, they may include headaches that are worse in the morning or with coughing, seizures, and cognitive or behavioral changes. In addition, depending on the tumor’s location, focal neurologic signs such as limb weakness, aphasia, or visual disturbances may occur.
3. What symptoms are typical of brain tumors in children?
In children, symptoms are often nonspecific, which makes early diagnosis difficult. Concerning features include persistent headache with morning vomiting, regression of motor skills, gait disturbance, and strabismus. In younger children, an increase in head size (macrocephaly) is also an important warning sign.
4. How does a brain tumor appear on MRI?
Contrast-enhanced MRI is the primary imaging method. The appearance depends on the tumor type. For example, glioblastoma often has irregular margins, heterogeneous contrast enhancement, and central necrosis. By contrast, metastases are usually round, well-demarcated lesions with marked surrounding edema.
5. Can a brain tumor be cured, and how is it removed?
Curability depends on the tumor’s type, size, location, and molecular characteristics. The main treatment is surgical resection, which may be partial (subtotal) or complete (gross-total). Modern technologies such as neuronavigation and intraoperative MRI help make surgery more radical while also improving safety.
6. How fast do brain tumors grow, and how long can a person live with them?
Growth rate and prognosis vary widely. Some low-grade gliomas may grow slowly over many years, whereas glioblastoma usually progresses rapidly. Without treatment, survival is often limited. However, modern multimodal therapy that combines surgery, radiotherapy, and systemic treatments can significantly prolong life.
7. Can a brain tumor resolve spontaneously, and why is it dangerous?
Brain tumors do not resolve spontaneously and require medical management or, at the very least, careful monitoring. They are dangerous because they compress and/or infiltrate surrounding brain tissue and increase intracranial pressure, which leads to both generalized and focal neurologic symptoms. Without timely treatment, the consequences can be life-threatening.
References
1.
VOKA Catalog. [Electronic resource].
https://catalog.voka.io/
2.
Louis, D. N., Perry, A., Wesseling, P., Brat, D. J., Cree, I. A., Figarella-Branger, D., Hawkins, C., Ng, H. K., Pfister, S. M., Reifenberger, G., Soffietti, R., von Deimling, A., & Ellison, D. W. (2021). The 2021 WHO classification of tumors of the central nervous system: A summary. Neuro Oncol. Neuro-Oncology, 23(8), 1231–1251. https://doi.org/10.1093/neuonc/noab106 PMID: 34185076; PMCID: PMC8328013.
3.
Ostrom, Q. T., Price, M., Neff, C., Cioffi, G., Waite, K. A., Kruchko, C., & Barnholtz-Sloan, J. S. (2023). CBTRUS statistical report: Primary brain and other central nervous system tumors diagnosed in the United States in 2016–2020. Neuro Oncol. Neuro-Oncology, 25(12, Suppl. 2), iv1–iv99. https://doi.org/10.1093/neuonc/noad149 PMID: 37793125; PMCID: PMC10550277.
4.
Price, M., Ballard, C., Benedetti, J., Kruchko, C., Barnholtz-Sloan, J. S., & Ostrom, Q. T. (2025). CBTRUS statistical report: Primary brain and other central nervous system tumors diagnosed in the United States in 2018–2022. Neuro-Oncology. Neuro Oncol. 2025. https://doi.org/10.1093/neuonc/noaf194
5.
Smith, H. L., Wadhwani, N., & Horbinski, C. (2022). Major features of the 2021 WHO classification of CNS tumors. Neurotherapeutics, 19(6), 1691–1704. 2022 Oct;19(6):1691-1704. https://doi.org/10.1007/s13311-022-01249-0 PMID: 35578106; PMCID: PMC9723092.
6.
Bonneville, F., Jäger, H. R., & Smirniotopoulos, J. G. (2024, February 11). Differential diagnosis 2024 Feb 11. In J. Hodler, R. A. Kubik-Huch, & J. E. Roos (Eds.), Diseases of the brain, head and neck, spine 2024–2027: Diagnostic imaging (Chap. 8). Springer. Chapter 8. https://doi.org/10.1007/978-3-031-50675-8_8
7.
Grand, S., Nedunchelian, M., Charara, S., Demaison, R., Jean, C., Galloux, A., Kastler, A., Attye, A., Berthet, C., & Krainik, A. (2023). Tumor or not a tumor: Pitfalls and differential diagnosis in neuro-oncology. Revue Neurologique, 179(5), 378–393. doi: 10.1016/j.neurol.2023.03.011. https://doi.org/10.1016/j.neurol.2023.03.011 PMID: 37030987.
8.
Chinthala, A. S., Obeng-Gyasi, B., Virgin, K. L., Deckert, M., & Mao, G. (2025). Brain metastasis mimicking brain abscess: Illustrative case and systematic review. Journal of Neurosurgery: Case Lessons, 10(16), CASE25528. https://doi.org/10.3171/CASE25528 PMID: 41115317; PMCID: PMC12548541.
9.
Englot, D. J., Chang, E. F., & Vecht, C. J. (2016). Epilepsy and brain tumors. Handbook of Clinical Neurology, 134, 267–285. https://doi.org/10.1016/B978-0-12-802997-8.00016-5 PMID: 26948360; PMCID: PMC4803433.