Brain Tumors: Etiology, Classification, Symptoms, Diagnosis, and Treatment
Brain tumors: early symptoms in adults and children, causes, modern diagnostic methods, and comprehensive treatment, including surgery, radiotherapy, and systemic therapy.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Metastases are the most common intracranial tumors in adults, occurring more frequently than primary brain tumors. In most cases, metastatic lesions of the brain are diagnosed following an already established systemic malignant process, but in some patients it may be the first manifestation of the tumor.

5 primary tumors are responsible for ~80% of all brain metastases:
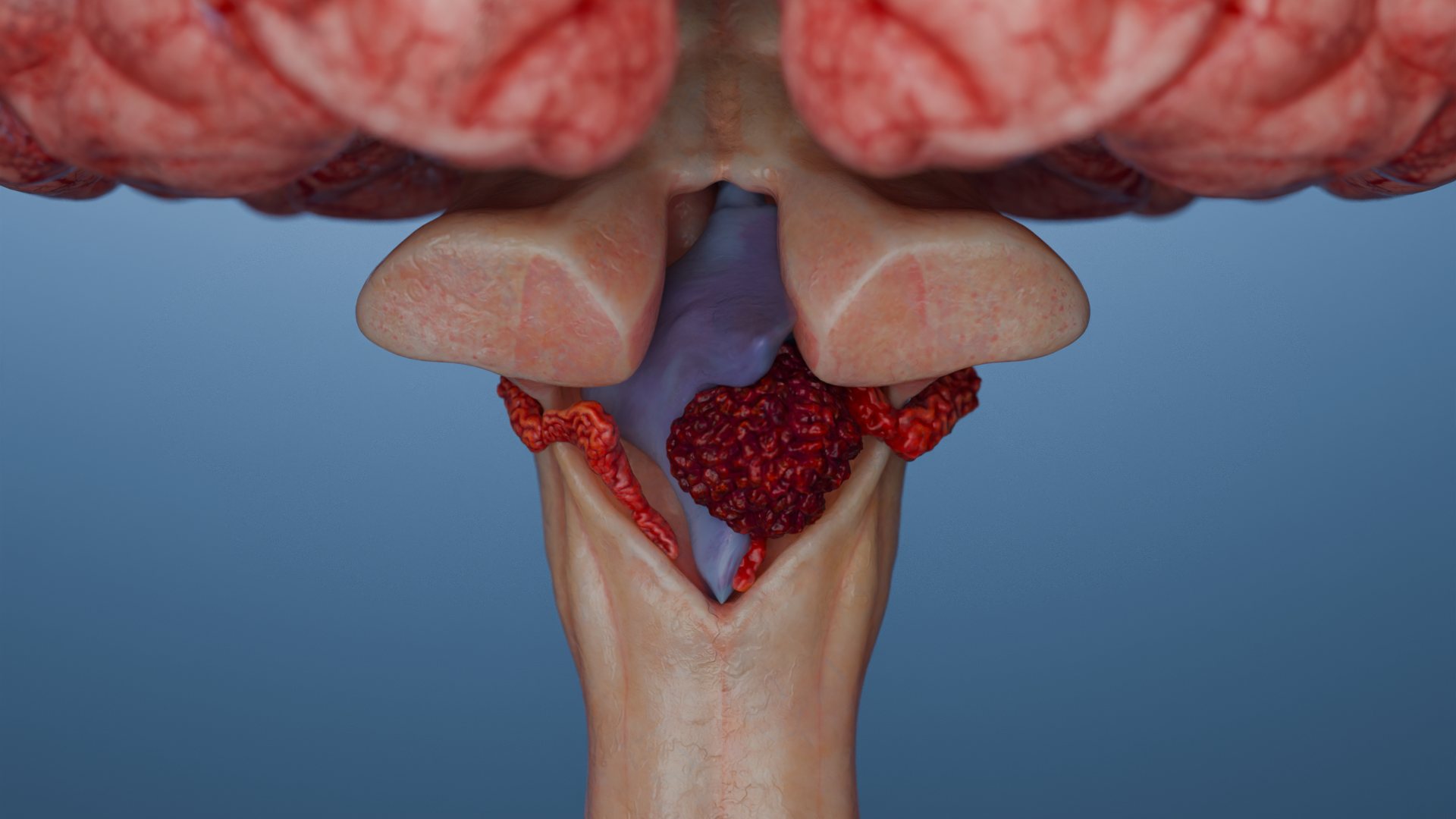
Metastases in the brain are predominantly formed hematogenously; the cells penetrate the blood-brain barrier and linger at the gray-white matter interface due to the vascular features of this area.
.webp)
At the time of initial diagnosis, brain metastases are found in approximately 2% of all patients with all tumor types and 12–15% of patients with already advanced (metastatic) disease.
During the course of the disease, brain metastases develop in 10–30% of patients with solid malignancies. For some types of neoplasms, the incidence can be as high as 40–50% in high-risk groups (HER2+ and triple-negative breast tumors, melanoma, non-small cell lung cancer).
Autopsy studies show that brain metastases are found in about 25% of patients with cancer, even if they were not detected during life.
Leptomeningeal metastases (along meninges) are more common in breast cancer, melanoma, lymphoma, and non-small cell lung cancer.
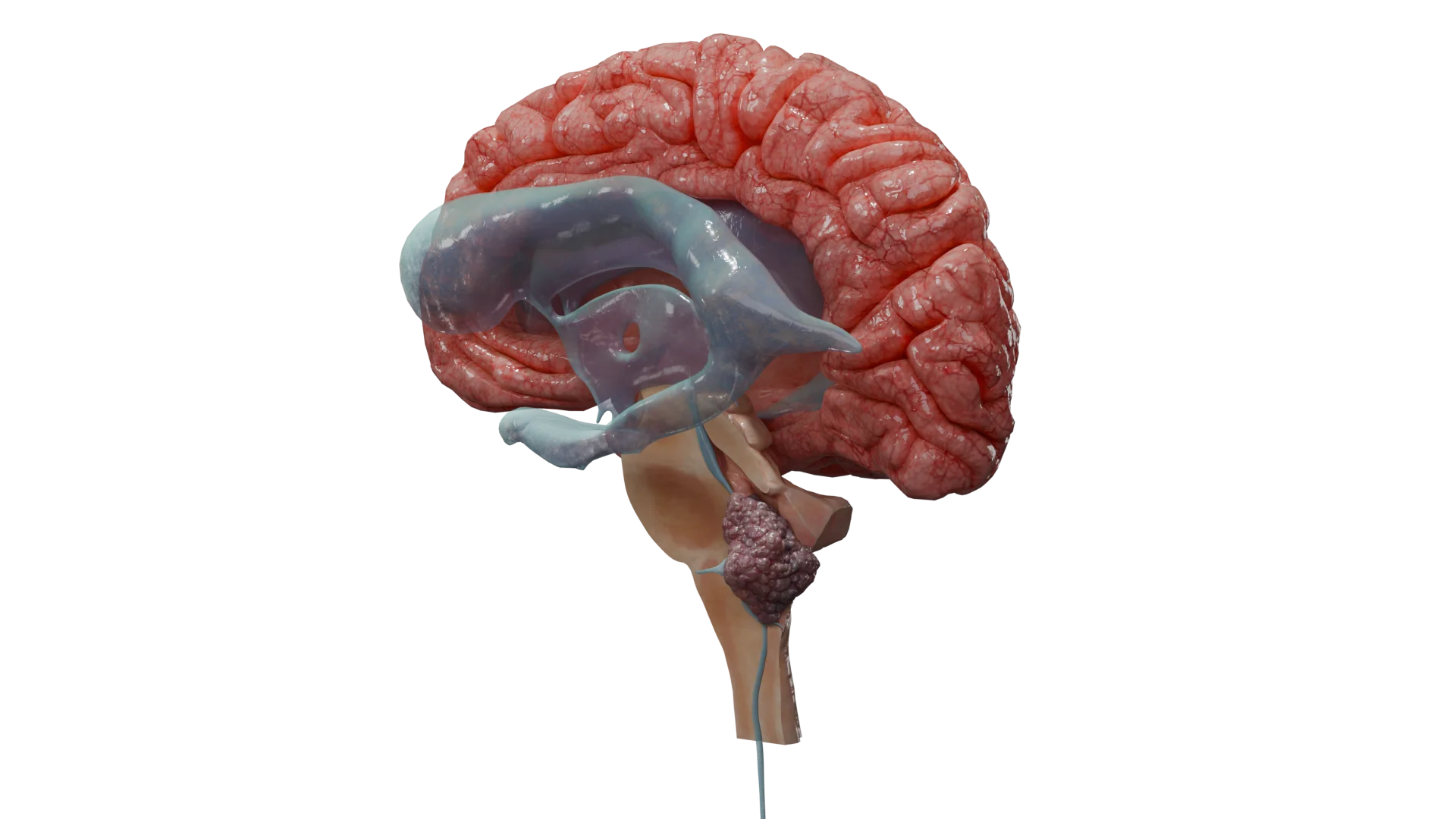
The majority (80%) of CNS metastases are located supratentorially, i.e. affect the hemispheres of the brain.
Up to 20% are located infratentorially (cerebellum, brainstem). Meninges are involved in up to 8% of cases.
The most common localization of metastases is the gray-white matter interface.
This assessment is used when choosing between radiosurgery (SRS), whole brain radiation therapy (WBRT), and surgery.
Small foci are available for stereotactic radiosurgery (SRS). Medium-sized foci (10–30 mm) usually imply dose constraints for single stereotactic radiosurgery (or require fractionation), and foci >30 mm are often considered for surgical removal or fractionated radiosurgery (large total dose is broken down and delivered in multiple steps), as single-fraction SRS in such cases carries a high risk of radionecrosis and edema.
Symptoms depend on the size, localization, growth rate and number of foci, as well as the involvement of liquor spaces and brain edema. The debut is usually acute or subacute.
Up to 20–30% of metastases are asymptomatic and are detected by imaging to clarify the diagnosis.
Acute impairment of consciousness / seizure status / severe vomiting + headache may indicate the following:
These conditions require emergency measures (seizure control, anti-edema therapy, emergency imaging [CT/MRI with contrast] and probably emergency neurosurgical intervention).
Differential diagnosis is performed with other focal lesions of the brain. The key features suggestive of metastases are the presence of a known primary cancer history, multiple foci, their typical localization at the gray-white matter interface (corticosubcortical), severe perifocal edema, and clear annular enhancement on MRI with contrast.
The main conditions the metastases should be differentiated with:
Gradual onset, focal neurologic symptoms, seizures, headache. On MRI, there is usually an infiltrative or solid mass (often solitary, as opposed to metastasis), edema, mass effect, and heterogeneous contrast accumulation.
Often fever, leukocytosis, and a focus of infection (otitis media, sinusitis, bacteremia). Mimics the tumor on MRI (also has annular enhancement) but has clear diffusion restriction (DWI+) in the center. MR spectroscopy reveals specific amino acids/metabolites.
On MRI, homogeneous enhancement and location in deep brain structures, especially in immunosuppressed patients. High diffusion restriction (DWI+), possible rapid regression after steroids, so it’s important to avoid them before biopsy.
It occurs months to years after radiation therapy, may mimic a recurrence or new metastasis. Distinguished by MR perfusion and PET (necrosis means hypoperfusion, hypometabolism), may decrease on steroids.
(especially the tumor-like form). Young age, multifocal lesions in the white matter, FLAIR-hyperintense without mass effect or contrast; clinical course is recurrent, with remissions, often in the young.
(especially in the subacute phase when there may be ring-shaped enhancement). Sudden onset, focal neurologic deficit, ischemic area visible on DWI/ADC MRI (diffusion restriction), more often localized across vascular basins.
Sudden headache, on CT/MRI with contrast — vascular mass, on angiography — dilated artery, subarachnoid hemorrhage.
Subacute onset, fever, confusion, and seizures — no focal mass. On MRI, changes are usually diffuse, often in the temporal lobes (e.g., in herpetic encephalitis), with no mass effect.
Acute onset with headache (often unilateral), eyelid swelling, ophthalmoplegia, and decreased vision. MRI/MR venography reveals thrombus in the venous sinuses. There is often infection of the facial, nasal, and sinus areas.
Sharp pain around the eye, lacrimation, rhinorrhea, lasting minutes, recurring in series, not accompanied by neurologic deficit. No structural changes on the MRI.
Often in the elderly, a triad of symptoms (gait disturbance, dementia, urinary incontinence), there may be headache and nausea, on MRI ventricular dilation without focal masses.
Causes diffuse rather than focal symptoms (confusion, seizures, tremors), with no focal mass on MRI. General tests (glucose, sodium, liver enzymes, creatinine, urea, etc.) help identify the cause.
The effect of whole brain radiation therapy (WBRT) is to control (stabilize) intracranial foci and reduce the incidence of intracranial recurrences.
It is used in multiple (>10) metastases and when SRS is not possible, and in leptomeningeal lesions.
Side effects:
Modern approaches: use of memantine (NDMA antagonist) and Intensity-Modulated Radiation Therapy (IMRT) with hippocampal exclusion reduce the risk of cognitive impairment.
Challenges of drug treatment of brain metastases:
1. Hematoencephalicbarrier (BBB):
2. Heterogeneity of the tumor.
3. The immunoprivileged environment of the brain.
Targeted therapy shows encouraging results (intracranial control can reach more than 50–80%). It is used for tumors with potential sensitivity to therapy (e.g., lung cancer with EGFR/ALK, melanoma with BRAF, HER2+ breast cancer). The use of targeted therapies or immunotherapy may delay or replace radiation therapy.
Immunotherapy (PD-1/PD-L1 inhibitors) may be effective in metastatic non-small cell lung cancer, melanoma and HER2+ breast cancer.
CAR-T therapy targets tumors expressing certain antigens different from normal brain tissue and has shown encouraging results in clinical trials, but is not yet routinely used (the method is undergoing clinical trials and is currently experimental in CNS oncology; studies are limited due to the risk of systemic toxicity and unpredictable effects in the CNS).
Find more scientifically accurate content on our social media








The Disease-Specific Graded Prognostic Assessment (ds-GPA) scale is the most accurate prognostic tool for metastatic brain lesions. It considers biological and molecular characteristics of primary tumors (in addition to age, KPS functional status, number of brain metastases, and extracerebral metastases that are standard for GPA).
The scale is used for metastatic brain lesions in lung cancer, melanoma, breast cancer, kidney cancer, and colorectal cancer.
In practice, rigid and universal prognostic schemes should be avoided in metastatic brain lesions, preferring an individualized approach based on the type of primary tumor, molecular profile, functional status of the patient, and available treatments.
Modern treatment of metastatic brain lesions requires a multidisciplinary approach based on the type of primary tumor and molecular characteristics of the metastasis, the number and localization of foci, and the general condition of the patient. SRS and targeted therapies are becoming the treatment of choice in most patients with limited metastases and sensitive tumors.
1. Which type of cancer most often metastasizes to the brain?
2. What do metastases look like on a brain MRI?
3. How fast do metastases in the head grow?
4. Can cancer be cured if it has metastasized to the brain?
5. What is the life expectancy for brain metastases?
References:
1.
VOKA Catalog. [Electronic resource].
https://catalog.voka.io/
2.
Vogelbaum MA, Brown PD, Messersmith H, Brastianos PK, Burri S, Cahill D, Dunn IF, Gaspar LE, Gatson NTN, Gondi V, Jordan JT, Lassman AB, Maues J, Mohile N, Redjal N, Stevens G, Sulman E, van den Bent M, Wallace HJ, Weinberg JS, Zadeh G, Schiff D. Treatment for Brain Metastases: ASCO-SNO-ASTRO Guideline. J Clin Oncol. 2022 Feb 10;40(5):492-516. doi: 10.1200/JCO.21.02314. Epub 2021 Dec 21. Erratum in: J Clin Oncol. 2022 Apr 20;40(12):1392. doi: 10.1200/JCO.22.00593. PMID: 34932393.
3.
Brenner AW, Patel AJ. Review of Current Principles of the Diagnosis and Management of Brain Metastases. Front Oncol. 2022 May 24;12:857622. doi: 10.3389/fonc.2022.857622. PMID: 35686091; PMCID: PMC9171239.
4.
Aizer AA, Lamba N, Ahluwalia MS, Aldape K, Boire A, Brastianos PK, Brown PD, Camidge DR, Chiang VL, Davies MA, Hu LS, Huang RY, Kaufmann T, Kumthekar P, Lam K, Lee EQ, Lin NU, Mehta M, Parsons M, Reardon DA, Sheehan J, Soffietti R, Tawbi H, Weller M, Wen PY. Brain metastases: A Society for Neuro-Oncology (SNO) consensus review on current management and future directions. Neuro Oncol. 2022 Oct 3;24(10):1613-1646. doi: 10.1093/neuonc/noac118. PMID: 35762249; PMCID: PMC9527527.
5.
Habbous S, Forster K, Darling G, Jerzak K, Holloway CMB, Sahgal A, Das S. Incidence and real-world burden of brain metastases from solid tumors and hematologic malignancies in Ontario: a population-based study. Neurooncol Adv. 2020 Dec 22;3(1):vdaa178. doi: 10.1093/noajnl/vdaa178. PMID: 33585818; PMCID: PMC7872008.
6.
Sener U, Wilcox JA, Boire AA. Leptomeningeal Disease: Current Approaches and Future Directions. Curr Neurol Neurosci Rep. 2025 Mar 18;25(1):25. doi: 10.1007/s11910-025-01412-y. PMID: 40100294; PMCID: PMC11920312.
7.
Sperduto PW, Kased N, Roberge D, Xu Z, Shanley R, Luo X, Sneed PK, Chao ST, Weil RJ, Suh J, Bhatt A, Jensen AW, Brown PD, Shih HA, Kirkpatrick J, Gaspar LE, Fiveash JB, Chiang V, Knisely JP, Sperduto CM, Lin N, Mehta M. Summary report on the graded prognostic assessment: an accurate and facile diagnosis-specific tool to estimate survival for patients with brain metastases. J Clin Oncol. 2012 Feb 1;30(4):419-25. doi: 10.1200/JCO.2011.38.0527. Epub 2011 Dec 27. PMID: 22203767; PMCID: PMC3269967.
8.
Huntoon K, Elder JB, Finger G, Ormond DR, Redjal N, Linskey ME, Olson JJ. Congress of Neurological Surgeons Systematic Review and Evidence-Based Guidelines Update for the Role of Emerging Therapies in the Management of Patients With Metastatic Brain Tumors. Neurosurgery. 2025 Jun 1;96(6):1172-1177. doi: 10.1227/neu.0000000000003383. Epub 2025 Mar 17. PMID: 40094364.
9.
Jacob Sperber, Seeley Yoo, Edwin Owolo, Tara Dalton, Tanner J Zachem, Eli Johnson, James E Herndon, Annee D Nguyen, Harrison Hockenberry, Brandon Bishop, Nancy Abu-Bonsrah, Steven H Cook, Peter E Fecci, Paul W Sperduto, Margaret O Johnson, Melissa M Erickson, C Rory Goodwin, Validation of the graded prognostic assessment and recursive partitioning analysis as prognostic tools using a modern cohort of patients with brain metastases, Neuro-Oncology Practice, Volume 11, Issue 6, December 2024, Pages 763–771.
10.
Brozos-Vázquez EM, Rodríguez-López C, Cortegoso-Mosquera A, López-Landrove S, Muinelo-Romay L, García-González J, López-López R, León-Mateos L. Immunotherapy in patients with brain metastasis: advances and challenges for the treatment and the application of circulating biomarkers. Front Immunol. 2023 Nov 3;14:1221113. doi: 10.3389/fimmu.2023.1221113. PMID: 38022574; PMCID: PMC10654987.
Loading test 6 questions
Table of Contents




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io