Fetal Positions in the Womb: Types, Diagnosis, Risks, Labor Management Techniques
Daria G.Gynecologist, fertility specialist, MD
17 min read·August 05, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Fetal position is defined as the relationship between the axis of the fetal body and the longitudinal axis of the uterus.
Fetal position is defined as:
Longitudinal: in the case of parallel axes (optimal);
Transverse: when perpendicularly located (pathologic);
Oblique: in case of an acute angle with the uterine axis (pathologic).
The optimal fetal position is cephalic occipital presentation with the head well bent anteriorly, with the fetal body positioned longitudinally in relation to the uterine axis.
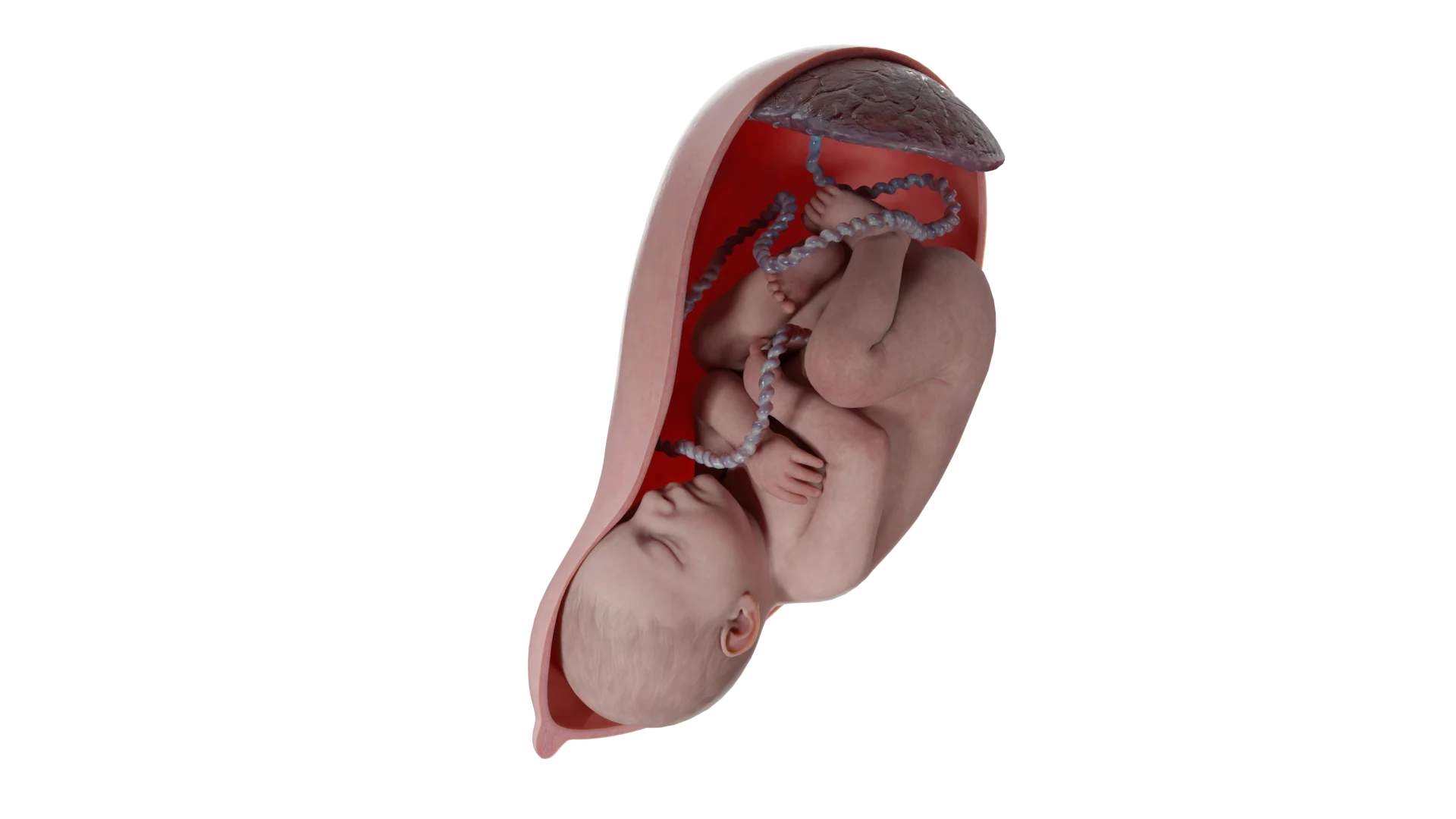
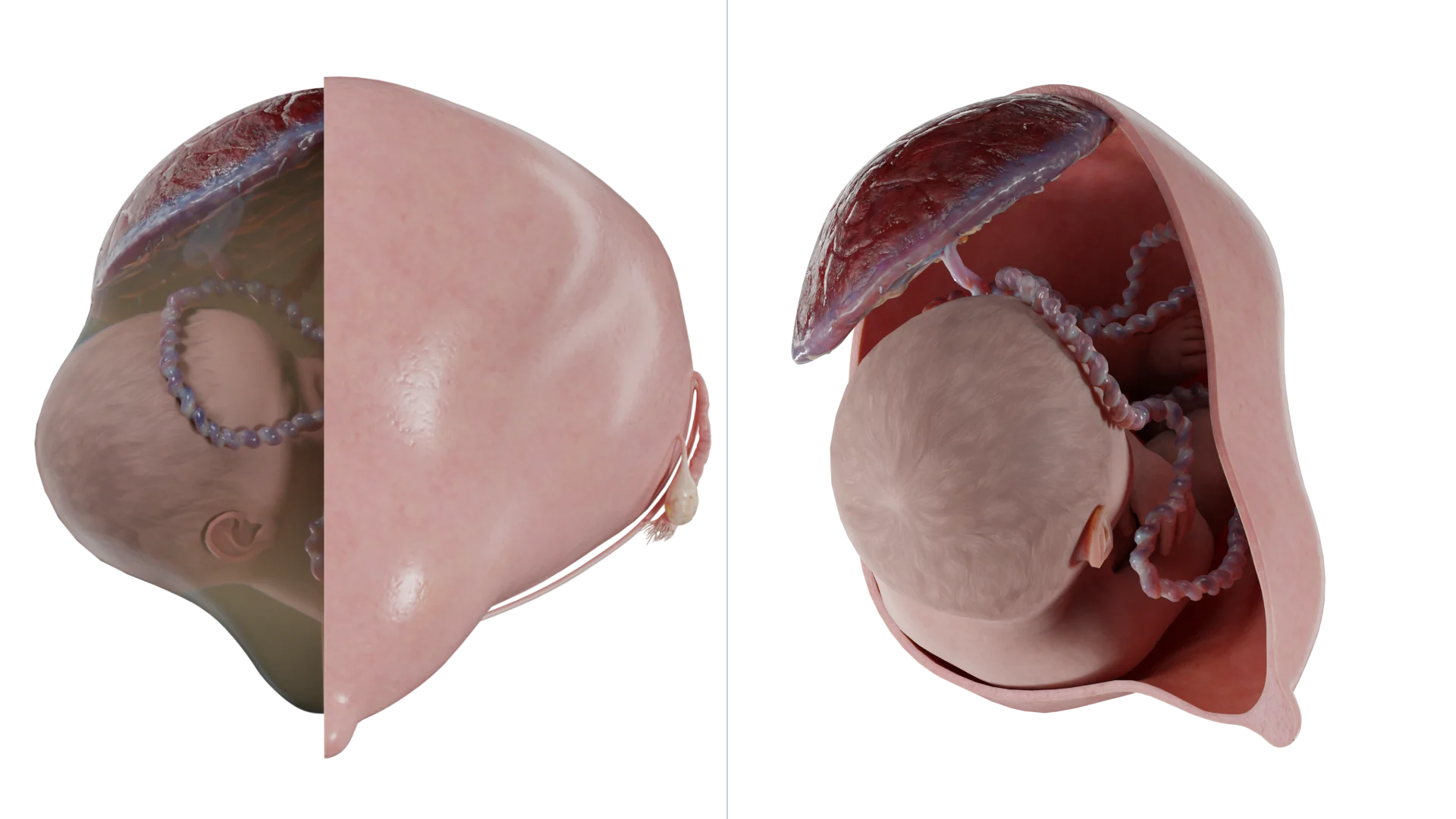
3D Animation: Transverse Position of the Fetus in the Womb
Transverse fetal position is diagnosed when the fetus is perpendicular to the longitudinal axis of the uterus. There are two configurations:
The curvature of the fetal spine is oriented downward (also called dorsoinferior), and the fetal shoulder is adjacent to the cervix.
The curvature of the fetal spine is oriented upward (also called dorso-superior), with small fetal parts and the umbilical cord adjacent to the cervix.
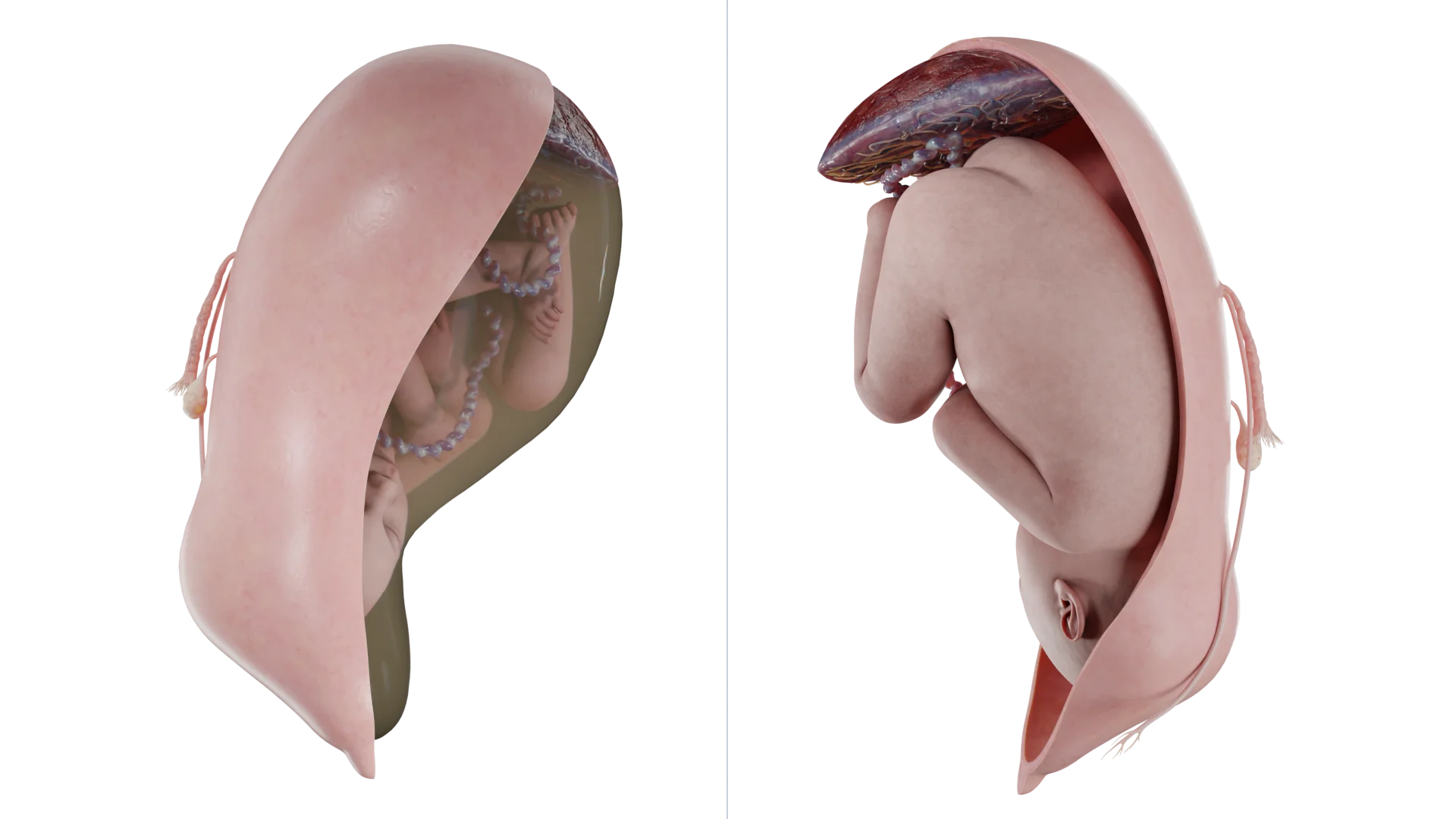
3D Animation: Oblique Position of the Fetus in the Womb
In the oblique position, the fetal body is at an acute angle with the uterine axis, with the pelvic or cephalic end below the iliac crest. On palpation and application of Leopold’s maneuvers, the fetal antrum is not identified above the symphysis. Auscultation of the fetal heartbeat is performed at the umbilicus. The oblique position of the fetus is extremely unstable and often changes to a longitudinal or transverse position during labor.
In transverse and oblique positions, the first position is defined when the fetal head is on the left side and the second when the fetal head is on the right side. The anterior view is defined when the dorsum is against the anterior uterine wall, and the posterior view is defined when the dorsum is against the posterior uterine wall.
Prevalence
Transverse and oblique fetal position at delivery are diagnosed in about 1 in 300 cases. Most often, malposition is diagnosed early in pregnancy. It is worth noting that transverse fetal positioning is unstable: according to literature data, in 85% of cases of transverse fetal positioning diagnosed at 24-28 weeks of pregnancy, it changes to longitudinal positioning by the end of pregnancy.
Pathogenesis and risk factors
In early pregnancy, when the volume of amniotic fluid is large in relation to fetal weight, the fetus is not limited by the size of the uterine cavity and is often in an abnormal position. As the pregnancy progresses, the volume of amniotic fluid decreases relative to fetal size, and the fetus more often assumes a longitudinal position oriented parallel to the uterine axis along the line of gravity.
Preterm labor is the most common risk factor for transverse fetal positioning in labor. Other risk factors include multiple pregnancies, placenta previa, anatomic pelvic narrowing, uterine anomalies or tumors, polyuria, and fetal anomalies. Placenta implantation site, uterine deformity, anatomical factors, and uterine distension alter the space in the uterine cavity and are likely to affect fetal position.
Diagnosis
On initial examination, an abdominal irregular configuration with an increase in transverse uterine size and abdominal circumference is noted.
Clinically, the diagnosis can be made by abdominal palpation using Leopold’s maneuvers. There is no possibility of palpating the head above the symphysis. Additional palpation allows detection of the fetal head along the right or left uterine margin. The upward or downward direction of the fetal buttocks is more difficult to detect, especially if the patient is obese. The sensitivity of abdominal palpation for detecting malposition at 35-37 weeks of gestation is approximately 70%󠄵󠄵󠄵󠄵󠄵.
Ultrasound
Ultrasound (USG) is used to confirm the diagnosis and determine the exact position and presentation of the fetus.
In addition, if an abnormal fetal position is detected, the uterine and fetal anatomy should be examined to look for anomalies or conditions associated with this unstable position. Placenta previa should be ruled out in the first instance. Importantly, in cases of suspected transverse fetal positioning by palpation with impossibility of ultrasound, it is recommended that a finger vaginal examination be abandoned.
Complications
Despite the significant reduction in morbidity and mortality associated with transverse fetal positioning due to modern perinatal care, this category of pregnant women still has an increased risk of maternal and perinatal morbidity compared to women with a longitudinally positioned fetus.
The development of complications largely depends on the availability and quality of medical care in the country. For example, in developed countries with unimpeded access to ultrasound diagnosis and skilled care, the main complications are:
Placenta previa;
Umbilical cord loop prolapse;
Fetal trauma;
Fetal anomalies;
Premature labor.
In resource-limited countries where ultrasound imaging, emergency caesarean section and neonatal intensive care are not available, maternal and perinatal mortality and morbidity remain high. Uterine rupture from prolonged labor in the transverse position is the leading cause of maternal and perinatal mortality.
In labor, the transverse fetal position can become complicated:
Fetal parts falling out;
Umbilical cord prolapse;
Development of a neglected transverse fetal position.
An advanced transverse fetal position is formed due to the increasing force of uterine contractions, with the fetus losing mobility, its handle or umbilical cord may fall out, and in severe cases, shoulder impaction is formed.
Management of labor
The oblique position is often transitional to transverse, and transverse fetal position is an indication for cesarean delivery. The mode of delivery also depends on the clinical circumstances at the time of diagnosis. Important factors to consider include:
The position of the placenta and umbilical cord;
Gestational age and fetal viability;
The onset of labor or rupture of the fetal membranes;
Presence of multiple pregnancies.
External obstetric turn for transverse fetal positioning
When the diagnosis of transverse fetal positioning is established before labor begins and there are no contraindications to vaginal delivery, an external obstetric rotation should be attempted at 37-37.6 weeks’ gestation.
Since the volume of amniotic fluid in this period is the largest, and the uterine tone and fetal weight is less than in later terms, performing the manipulation at 37-37.6 weeks of pregnancy increases the likelihood of success.
Experts disagree on the influence of maternal weight, placental position and amniotic fluid volume on the success of the manipulation. The majority of practitioners believe that the chance of successful turning is increased in repeat mothers, patients with normal weight, posterior placenta position and sufficient volume of amniotic fluid. In addition, if complications arise during the turn attempt, the manipulation can be completed by emergency cesarean section. If the turn attempt is unsuccessful, a second attempt is made at 38-39 weeks of gestation.
An alternative approach is to perform an external obstetric rotation at 39 weeks’ gestation, followed by amniotomy and induction of labor. The rationale for induction of labor is that the transverse position is a highly unstable position that can change spontaneously after turning, unlike the breech position where reversal is rare.
Risks associated with the manipulation
The most common complication is a temporary slowing of the fetal heart rate (up to 40% of cases). This condition persists for several minutes after termination of the procedure and is not associated with adverse effects on the fetus. Rare complications include fetal bone fractures, premature rupture of the fetal membranes, premature detachment of the normally located placenta, hemorrhage and uterine rupture. To date, there is a paucity of studies that show whether the overall risk of perinatal mortality increases after an external rotation. A 2015 Cochrane review identified the risk of perinatal death in patients who underwent external rotation as 2 out of 644 cases versus 6 out of 661 cases in the no-manipulation group.
Methodology
The day before, an ultrasound scan is performed to determine the fetal position, weight and volume of amniotic fluid, and to rule out placenta previa and fetal anomalies. A non-stress test (alternative: fetal biophysical profile) should be performed the day before the procedure. The procedure is performed in a deployed operating room with the mandatory presence of anesthesiologists-anesthesiologists. Routine tocolysis and routine use of spinal or epidural anesthesia are not recommended.
An external turn is accomplished by moving the head end smoothly toward the woman’s pelvis while the pelvic end moves toward the uterine fundus. There is no consensus on how many attempts at turning can be made. After an attempted inversion, regardless of success, a non-stress test (biophysical profile if necessary) should be repeated. In addition, Rh immunoglobulin should be administered to Rh negative women.
Tactics in different clinical situations
Preterm labor
Preterm labor in transverse fetal position requires a cesarean section.
Premature rupture of the fetal membranes
If the gestational age exceeds 34 weeks, the patient should be delivered by caesarean section. If the gestational age is less than 34 weeks, it is recommended to adopt a wait-and-see approach to prevent fetal respiratory distress syndrome. It should be noted that a wait-and-see approach is only possible in the absence of infection, bleeding and labor.
Transverse position of the second fetus after the birth of the first fetus
After the birth of the first fetus, the second fetus may assume a transverse position, regardless of its original position in the uterus.
In such cases, an internal rotation of the fetus can be performed under anesthesia. This procedure is performed immediately after the birth of the first fetus, when the cervix is fully opened and the fetal membranes are intact. The manipulation can only be performed by an experienced doctor, as there is a risk of injury to the fetus in complicated cases. The external obstetric turn is an alternative approach that is simpler to perform. It is mandatory to perform ultrasound monitoring of the fetus during any of the manipulations.
There are no studies described in the literature that provide high quality comparative data demonstrating the relative merits of internal versus external rotation. It is important to note here that the clinician should proceed based on his or her level of training and experience.
Antenatal death
In case of antenatal fetal death in the transverse position, an external obstetric turn is recommended, regardless of the integrity of the fetal membranes, followed by induction of labor.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Peculiarities of cesarean section surgery
In patients with a well-developed lower uterine segment, a low transverse hysterotomy is performed. Some experts recommend a vertical uterine incision, which is also a reasonable approach if the lower uterine segment is not well developed. However, a vertical hysterotomy, even if limited to the lower segment, is less desirable because making a vertical incision increases the risk of uterine rupture in repeat pregnancies. On the eve of surgery, an external obstetric rotation is recommended to facilitate retrieval. The end of the fetus, which will become the antecubital part, is rotated towards the entrance of the woman’s pelvis, while the other end is directed in the opposite direction. It is possible to turn the fetus into either a cephalic or breech presentation, but most physicians favor a breech presentation because it is technically easier to perform. Once the turn is complete, the physician assistant holds the fetus in a longitudinal position so that it does not return to its original position. A hysterotomy is then performed and the fetus is extracted.
FAQ
1. How do I determine the position of the fetus?
The fetal position is determined by clinical examination and instrumental methods. By palpation of the abdomen (Leopold maneuvers), the doctor assesses the position of the head, back and buttocks of the fetus. Ultrasound is the most accurate method to confirm the position, presentation and exclude associated pathologies. In oblique or transverse positions, the fetal heartbeat is usually heard at the navel.
2. What is the difference between transverse fetal position and oblique fetal position?
In the transverse position, the fetal axis is strictly perpendicular to the uterine axis, with the fetus lying horizontally and its head and pelvic end at the sides of the uterus. The oblique position is characterized by an acute angle between the fetal and uterine axes, with one end of the fetus (head or pelvis) below the iliac crest. The oblique position is less stable and often changes to a longitudinal or transverse position during labor.
3. What are the causes of abnormal fetal position?
The main causes include preterm labor, when the fetus does not have time to get into the correct position. Other factors include multiple pregnancies, placenta previa, uterine abnormalities, multiple uteri and narrow pelvis. The risk increases with uterine tumors or fetal abnormalities that limit fetal movement.
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
American College of Obstetricians and Gynecologists. (2023). Mode of term singleton breech delivery (Practice Bulletin No. 221). Obstetrics & Gynecology, 141(5), e156–e171.
3.
Hankins, G. D. V., et al. (2020). Transverse fetal lie: Diagnosis, risks, and management. American Journal of Obstetrics and Gynecology, 222(3), S1–S8.
4.
Royal College of Obstetricians and Gynaecologists. (2023). External cephalic version and reducing the incidence of term breech presentation(Green-top Guideline No. 20a).
5.
Hofmeyr, G. J., et al. (2023). External cephalic version for breech presentation at term. Cochrane Database of Systematic Reviews, 2023(4), CD000083.
6.
Ultrasound-guided management of transverse lie in late pregnancy. (2023). Ultrasound in Obstetrics & Gynecology, 61(2), 210–215.
7.
Bianco, A., et al. (2024). Management of transverse fetal lie in the third trimester: A systematic review and meta-analysis. American Journal of Obstetrics & Gynecology MFM, 6(1), 101012.
https://doi.org/10.1016/j.ajogmf.2024.101012
8.
Zafarmand, M. H., et al. (2023). Ultrasound-guided management of unstable lie in late pregnancy: A multicenter randomized trial. Ultrasound in Obstetrics & Gynecology, 61(3), 345-351.
https://doi.org/10.1002/uog.26145
9.
Palacios-Jaraquemada, J. M., et al. (2023). Placental location and transverse fetal lie: MRI-based classification system. Journal of Maternal-Fetal Medicine, 36(4), 789-795.
https://doi.org/10.1080/14767058.2023.2184256
10.
Lees, C. C., et al. (2024). Transverse lie in late pregnancy: Modern management approaches. BJOG: An International Journal of Obstetrics & Gynaecology, 131(2), 145-152.
https://doi.org/10.1111/1471-0528.17654
11.
D’Souza, R., et al. (2023). Maternal and neonatal outcomes in pregnancies complicated by transverse lie: Systematic review. European Journal of Obstetrics & Gynecology, 287, 56-62.