The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
C-section is one of the oldest operations in medicine, but only in recent decades has a system of evidence-based standards guiding indications, technique, and postoperative management emerged.
According to WHO (2021), the optimal frequency of C-section in the population is 10–15%, but in some countries this figure exceeds 30–40%. Overuse of surgery without strict indications increases the risk of maternal and fetal complications and increases the incidence of placental abnormalities and uterine rupture in subsequent pregnancies.
3D animation: C-section
Indications for C-section
Maternal indications
Absolute indications
Complete placenta previa with hemorrhage or occlusion of the internal orifice of the uterus;
Rupture or threatened rupture of the uterus;
Severe eclampsia, HELLP syndrome, in which delivery is necessary as soon as possible;
Severe pelvic deformities that prevent fetal movement;
Active genital herpes infection at delivery (risk of neonatal infection).
Refusal of vaginal delivery when there are justified medical risks (individual decision).
Fetal indications
Acute fetal hypoxia confirmed by electronic fetal monitoring (EFM), biophysical profile or fetal blood pH;
Abnormal presentation: transverse, oblique or breech presentation in the absence of conditions for safe vaginal delivery;
Multiple pregnancies if the first fetus is not in a cephalic presentation;
Vasa praevia and other vascular abnormalities of the umbilical cord;
Large fetus with clinically narrow pelvis.
Indications for combined conditions
A combination of moderate risk factors (e.g., breech presentation + uterine scar + fetal hypoxia) may also be grounds for elective C-section.
Importantly, elective surgery should not be performed before 39 weeks of gestation to reduce the incidence of respiratory complications in the newborn (NICE NG192, 2021).
Preoperative preparation for a C-section
1. Clinical evaluation and informed consent
Medical and obstetric history, laboratory parameters (Hb, Ht, coagulation profile, blood group, Rh factor) are analyzed. The purpose, risks, and alternatives to surgery are explained to the woman in detail, and informed consent is documented.
For elective C-section, consultation with an anesthesiologist is recommended, discussing the type of anesthesia and the possibility of early mother-baby contact.
2. Antibiotic prophylaxis
According to ACOG (2023) and RCOG (2022):
Cefazolin 2 g IV 30 minutes before incision; if mother’s weight is >120 kg / 265 lbs, administer 3 g;
For allergies, clindamycin + gentamicin;
Additional dose in case of surgery duration >2 h or massive blood loss > 1500 ml.
3. Prevention of thromboembolic complications
Elastic compression of the lower extremities to all laboring women;
Low molecular weight heparins (enoxaparin 40 mg/day): in case of VTE risk factors (obesity, varicose veins, age >35 years);
Administration of LMWH 6–12 h after surgery if there are no signs of bleeding.
4. Anesthesia care
Regional anesthesia is the method of choice for routine C-section (spinal or combined spinal-epidural). Benefits:
Patient is alert;
Risk of aspiration is minimal;
Early interaction with the newborn is possible.
General anesthesia is indicated for contraindications (coagulopathy, severe hypovolemia, urgency <5 minutes).
5. Psycho-emotional preparation and partner involvement
Current protocols (NICE, WHO) allow for the presence of a partner during elective C-section while maintaining sterility, which reduces anxiety and improves maternal adjustment.
Modern surgical techniques for C-section
General principles of surgical access
The aim of surgical technique in C-section is to ensure safe, non-traumatic and rapid delivery with minimal blood loss and preservation of anatomical tissue integrity for the subsequent reproductive function of the woman.
Current international recommendations (NICE NG192, WHO 2021, ACOG 2023, RCOG 2022) emphasize the need for gentle, standardized methods, minimizing the use of sharp instruments and electrosurgery, as well as the rejection of routine manipulations that have not proven effective (suturing of the peritoneum, drainage).
Types of skin and fascial incisions
Pfannenstiel incision
The most commonly used access for elective C-section. The incision is made 2–3 cm above the symphysis, arched, 12–15 cm long.
Layer-by-layer dissection: skin, subcutaneous tissue, anterior fascia of abdominal rectus muscles, blunt muscle stripping, peritoneal dissection.
Benefits: good cosmetic result, reduced risk of postoperative hernias, adequate visibility with a developed lower segment.
Disadvantages: limited view in severe adhesions, may be technically more difficult in emergency situations.
Skin incisionSubcutaneous fatty tissue incision
Joel-Cohen incision
Developed in the 1970s as an alternative to Pfannenstiel. It is performed rectilinearly 3 cm above the projection of classic Pfannenstiel incision, 15 cm long.
Main features:
Only the skin and fascia are transected, the muscles and peritoneum are pulled apart bluntly.
The peritoneum is opened transversely without dilation with scissors.
Routine suturing of the parietal and visceral peritoneum is not performed.
Advantages include: reduced surgery time by 6–10 min, reduced postoperative pain, less blood loss and incidence of fever (Cochrane, 2022).
Disadvantages: less aesthetically pleasing incision than Pfannenstiel, but it has no clinical significance.
Misgav-Ladach technique (Joel-Cohen variant)
An evolutionary development of the Joel-Cohen method proposed by Stark (1995).
Reduced incidence of postpartum infections and pain syndrome;
Earlier mobilization and discharge.
Use: it is the “gold standard” in most clinics in Europe for elective C-section.
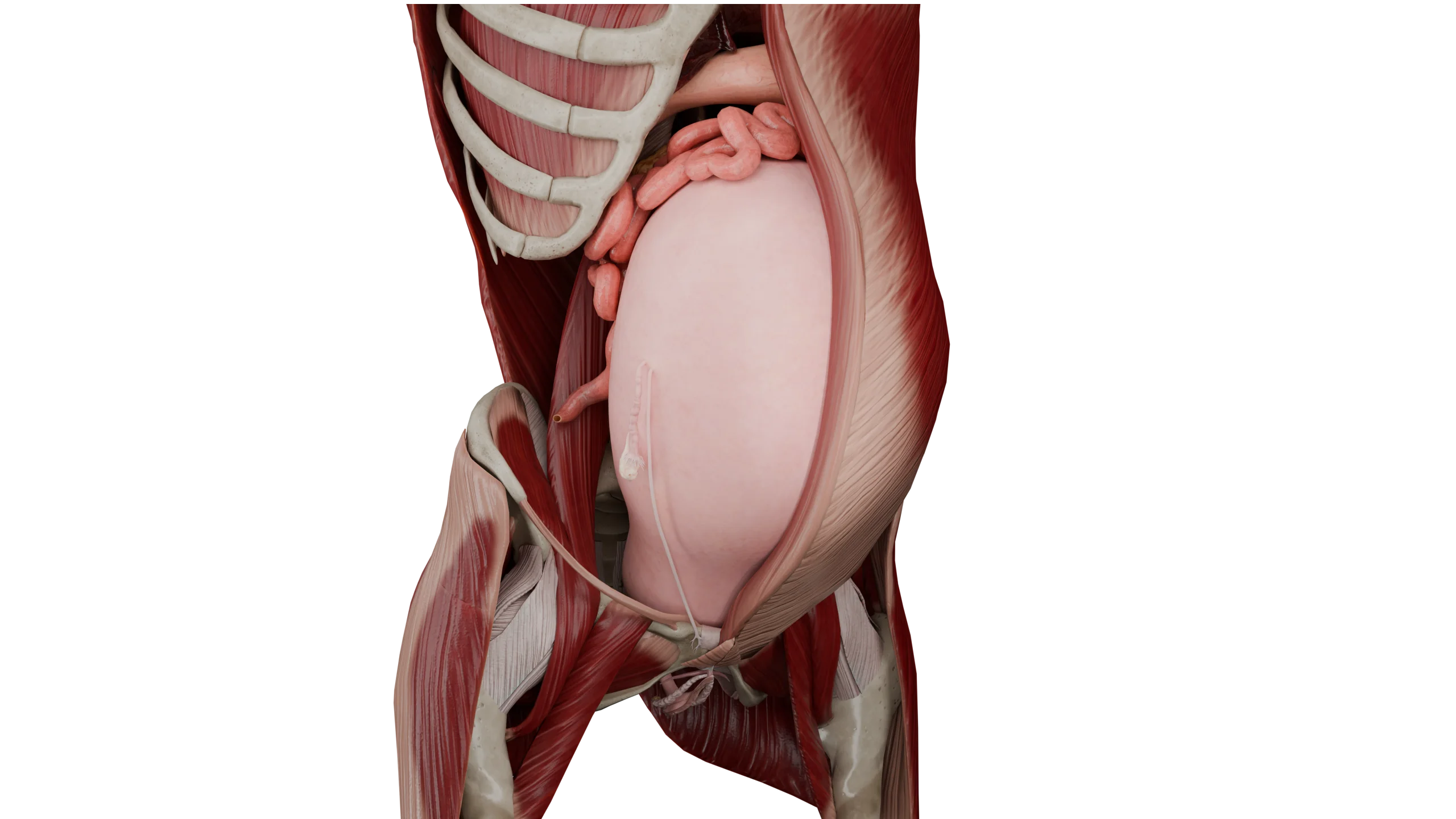
Uterine incision (hysterotomy)
Lower segmental transverse incision
The safest and most common access. It is performed in the lower segment of the uterus, 1–2 cm above the uterovesical fold.
The incision is 2–3 cm long, which is then extended with the fingers (bluntly).
After extracting the fetus, suturing with absorbable suture material is performed.
Benefits:
Minimal blood loss;
Robust scar;
Low risk of rupture in subsequent births (up to 0.5%);
Technical simplicity.
Disadvantages: difficult in severe adhesions or undeveloped lower segment (before 30 weeks of gestation).
Uterine incision
Vertical (classic) incision
It runs from the lower segment up the body of the uterus for 8–10 cm. Indications:
Placenta previa;
Premature pregnancy (≤28 weeks);
Pronounced adhesions;
Fetal position abnormalities.
Disadvantages:
High risk of bleeding;
Failed scar (risk of rupture in subsequent pregnancy up to 4–9%);
Increased incidence of infectious complications;
It is used only in the event of life-threatening conditions.
T- and J-incisions
Used in cases of difficult extraction (e.g., large heads or abnormal presentations).
Performed as an upward (T) or lateral (J) extension of the transverse incision.
It should be kept in mind that such incisions increase the risk of scar failure in subsequent pregnancies, and the patient should be advised to undergo elective C-section in subsequent deliveries.
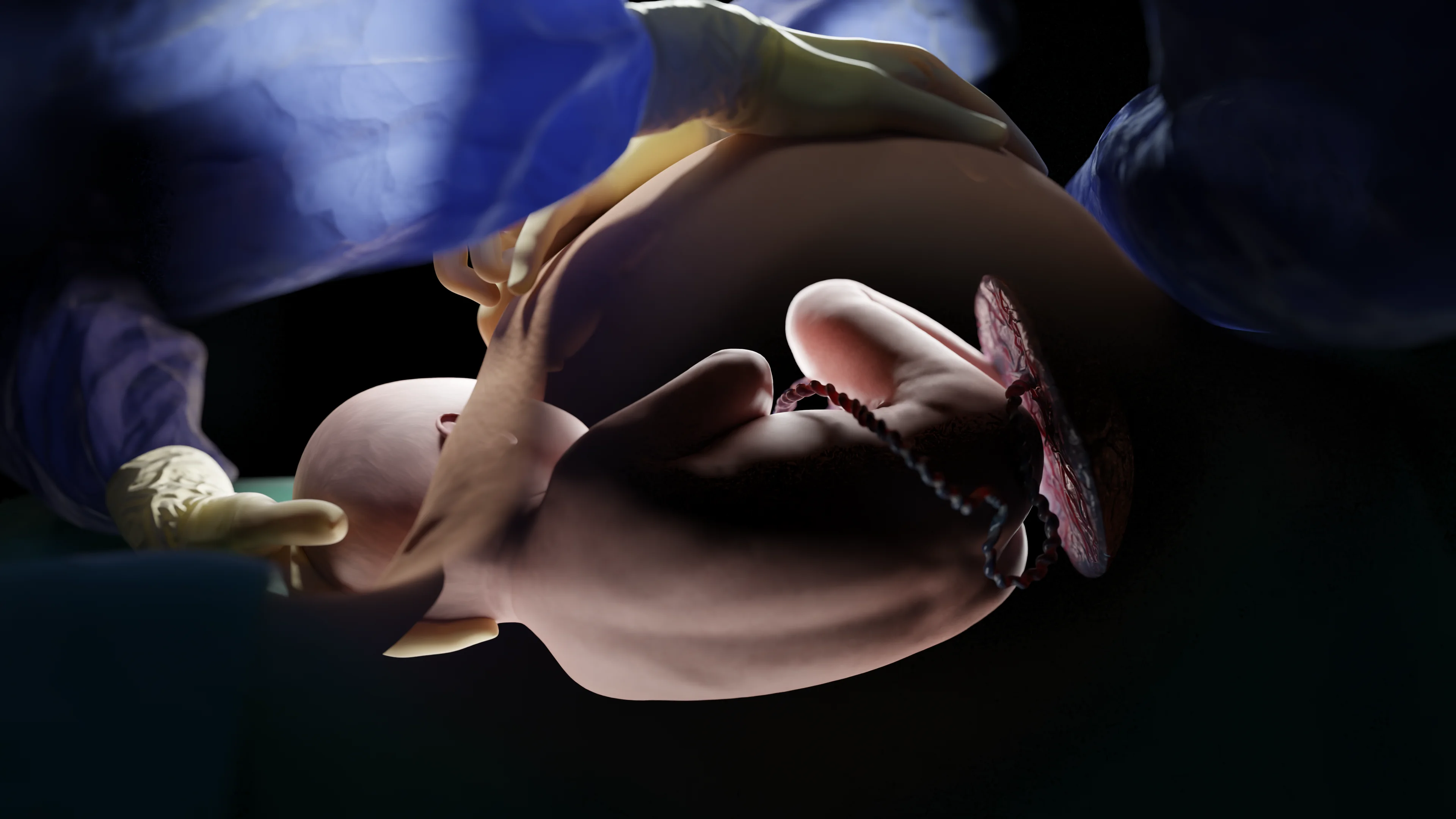
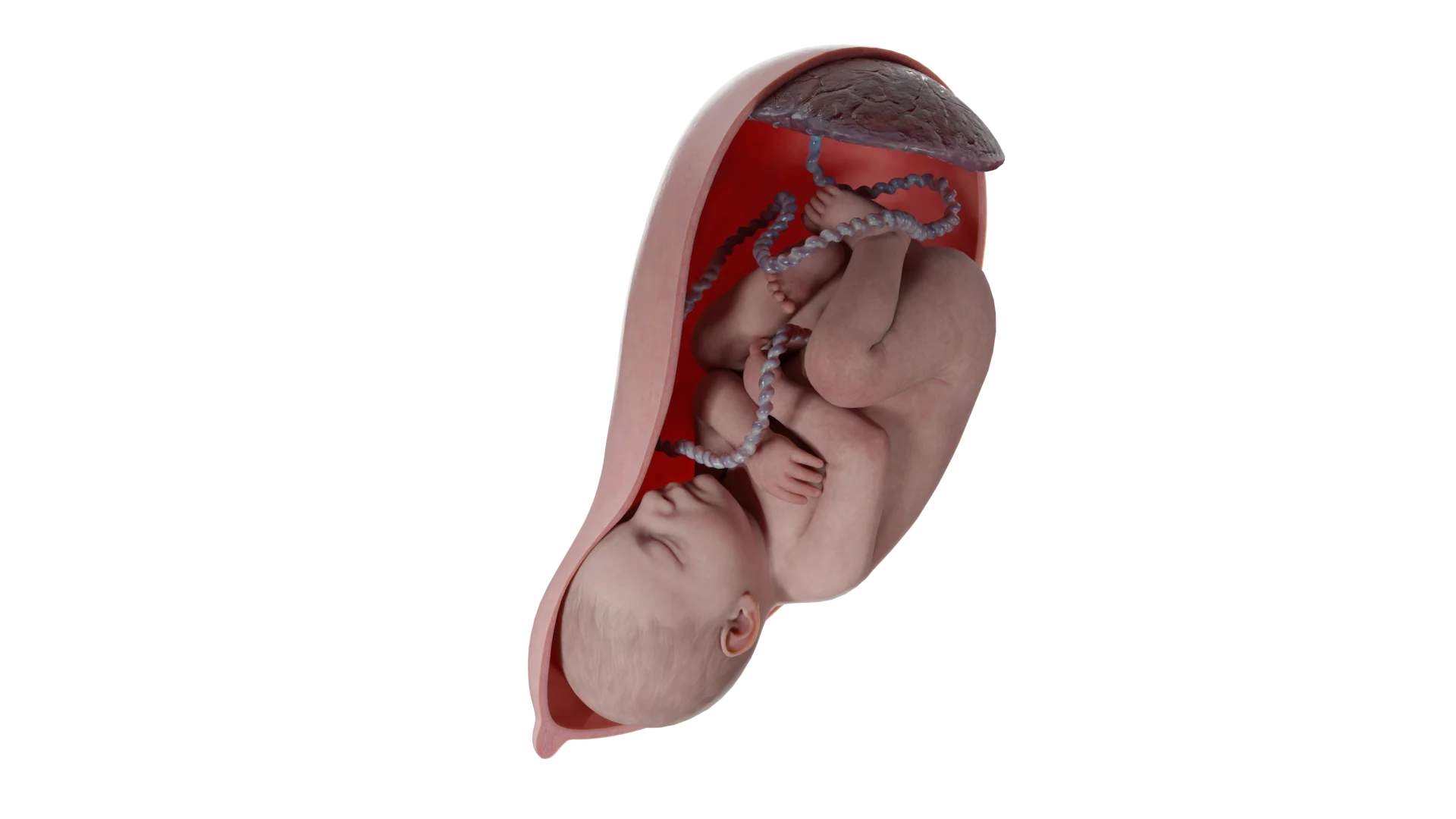
Fetal extraction
After opening the amniotic fluid sac and removing a small amount of amniotic fluid, the fetus is extracted by the following methods:
Cephalic presentation: a hand is inserted under the head through the incision and withdrawn with minimal tissue tension.
Breech presentation: retrieval by the buttocks, then shoulders and head (Tsovianov method or classic Bracht technique).
Transverse presentation: internal fetal leg turn technique and subsequent retrieval is possible.
Key point: avoid excessive traction pressure to minimize uterine and fetal injury.
Fetal extraction
Placenta separation and prevention of hemorrhage
Spontaneous separation of the placenta is the safest. After its exit, the uterine cavity is inspected and the remains of fetal membranes are removed.
Blood loss prevention:
Administration of oxytocin 10 U intravenous bolus, followed by infusion of 20–40 U in 1000 mL of solution at a rate of 60–80 mL/h;
At risk of hypotension, carbetocin 100 mcg intravenously slowly;
Uterus massage to a firm tone.
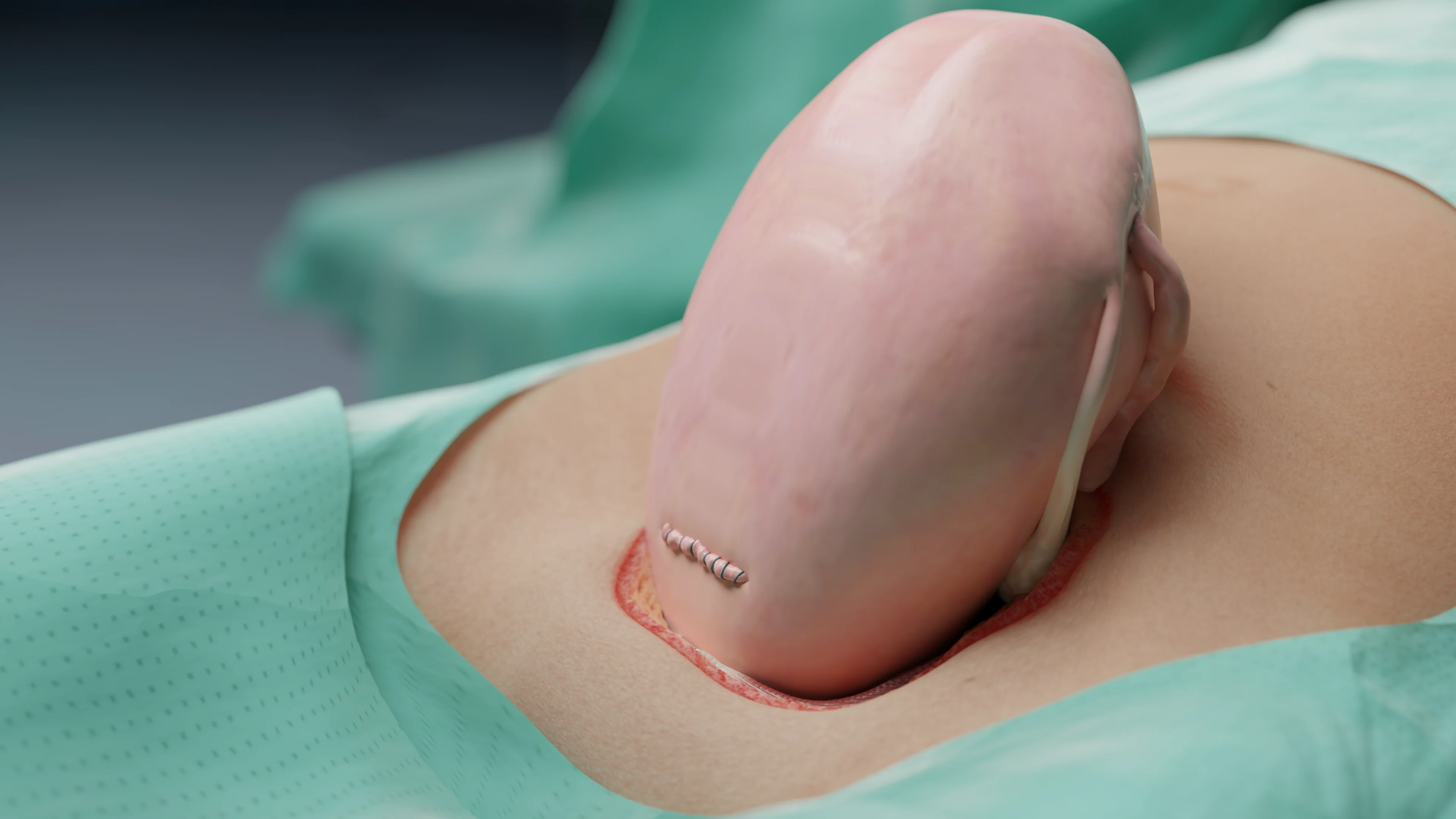
Uterine suturing technique
Single suture
It is performed with continuous absorbable material (Vicryl 1–0).
Simplicity, shorter surgery time, less blood loss.
It is used in the Misgav-Ladach technique.
Meta-analyses (Bujold et al., 2021) show scar strength comparable to the double sutures.
Uterine suturing
Double suture
The first line is a continuous suture of the mucosal and muscular layer; the second line is a serosal-muscular inverting line.
The advantage is a formation of potentially more reliable scar.
Disadvantage is longer surgery time, slightly increased blood loss.
Nuances
Use of synthetic absorbable materials (vicryl, polyglycolide).
Areas of ischemia or excessive tissue tension should not be left.
In case of bleeding surgical edges, separate Z- or octagonal sutures are used.
Suturing and closing the layers of the abdominal wall
Peritoneum is not sutured, as proven not to increase the risk of infections and reduce surgery time.
Fascia is sutured with continuous sutures with absorbable material (Vicryl 1–0).
Subcutaneous tissue is sutured at >2 cm thickness for prevention of seroma.
Dermal suture is intradermal cosmetic (monofilament 3–0) or metal staples if quick closure is needed.
End with aseptic dressing, hemostasis control and surgical count.
Alternative and modified techniques
“Modified Stark”
Combines Joel-Cohen incision with adapted double-row uterine suturing and use of a single dose of antibiotic prior to incision. Widely used in Germany and Scandinavia.
“Modified Misgav-Ladach”
It is used in emergency situations: minimal dissection, rapid fetal retrieval, single suture closure of the uterus, and temporary hemostatic B-Lynch suture if necessary.
Mini-laparotomy C-section
Used for small fetuses or antenatal death; skin incision ≤10 cm, minimal injury, used mainly in developing countries.
Uterine Exteriorization vs In situ suturing
Exteriorization
The uterus is removed from the abdominal cavity for visualization and convenient suturing.
Benefits: better visibility, hemorrhage control.
Disadvantages: increased pain and transient hypotension due to ligament traction.
In situ suturing
Suturing the uterus in place without taking it out.
Less significant hemodynamic responses.
Equivalent scar and blood loss outcomes.
The choice of method is determined by the surgeon’s experience and the patient’s condition.
Drainage and hemostasis control
Routine abdominal drainage is not recommended (NICE, 2021). Indications:
Massive blood loss;
Bladder damage;
Fused placenta.
Control of hemostasis is performed before suturing the fascia — careful inspection of the peritoneum and corners of the uterine incision.
Duration and quality of the surgery
Average time of standard C-section (Misgav-Ladach): 25–35 minutes.
Average blood loss: 400–800 ml.
Key quality indicators:
Time from skin incision to fetal birth <5 min;
Absence of additional hemostatic sutures;
Reliable hemostasis and a smooth scar.
Current trends and innovations
ERAS approaches in the surgery room: minimizing infusions, warming the patient, and multimodal anesthesia.
Use of ultrasonic scalpels to reduce blood loss (studies limited).
Photo documentation and digital recording of C-section steps — implemented for quality control.
Gentle cesarean technology: delayed fetal extraction, maintaining skin-to-skin contact right in the surgery room, psychological support — encouraged by NICE and RCOG for elective surgery cases.
Intraoperative prevention measures
Bleeding prevention:
Oxytocin 10 units IV; at risk — carbetocin 100 mcg IV;
Hemostasis control and temporary vascular compression;
In placenta percreta, multidisciplinary preparation, embolization or hysterectomy is possible.
Thermal control: maintaining a temperature ≥36°C (≥97°F) reduces the risk of blood loss and infection.
Rational infusion therapy: crystalloid restriction < 2 liters, colloids/transfusions according to hemodynamics if necessary.
Postoperative management after C-section
Monitoring and observation
The first 2 hours — in the intensive care ward: control of BP, pulse, diuresis, uterine condition and blood loss. If there are signs of hypotony or bleeding, immediate wound inspection and hemostatic therapy are required.
Anesthesia
Multimodal approach (per ERAS-ACOG 2022):
NSAIDs (ketorolac, ibuprofen) + paracetamol at regular intervals;
Local blocks (TAP block, QL block) or prolonged epidural analgesics;
Minimizing opioids, using them only for severe pain.
Early mobilization and nutrition
It is allowed to get up after 6 h, fluids after 2 h, food after 6 h in the absence of nausea. Eating early improves peristalsis and reduces the risk of intestinal paresis.
Prevention of thrombosis
Mechanical compression immediately after surgery, LMWH — after 6–12 h. Duration — up to 7 days or longer if high risk.
Infection control
Temperature of >38°C (100°F) in the first 48 hours is a reason to rule out endometritis or wound infection. Treatment is empirical (II–III generation cephalosporin + metronidazole).
Rehabilitation and discharge
Discharge home on the 3rd to 5th day, if condition is satisfactory. Recommendations after the procedure:
Follow-up at OB-GYN in 10–14 days;
Avoiding from intensive exercise for 4–6 weeks;
Optimal inter-pregnancy interval is ≥18 months.
Breastfeeding support
In regional anesthesia, early skin-to-skin contact and breastfeeding in the first 30 minutes, which reduces the risk of lactational problems and postnatal depression.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Principles of modern approaches to C-section performance
Modern approaches to C-section are based on four key principles:
Optimization of indications: striving to reduce the incidence of primary C-sections is one of WHO’s global goals. The use of scales (e.g., Robson classification) allows standardization of indications and analysis of the quality of obstetric care.
Gentle surgical techniques: Misgav-Ladach technique has proven benefits in shorter surgery duration, less blood loss and pain without increasing complication rates.
Comprehensive prevention of complications: single antibiotic prophylaxis before incision and VTE prophylaxis are mandatory quality of care standards.
ERAS programs: early mobilization, infusion restriction, multimodal pain management, and early nutrition shorten hospital stays and speed recovery.
Despite standardization, controversial issues remain: the optimal method of uterine suturing, the need to suture the peritoneum, the choice of drugs to prevent bleeding. These topics require further multicenter studies.
C-section is a highly effective method of delivery for strict medical indications. Current international guidelines aim to improve safety, reduce complications and preserve a woman’s reproductive health.
Optimal C-section performance includes:
Strict adherence to indications;
Antibiotic prophylaxis prior to incision;
Using of gentle techniques (Joel-Cohen/Misgav-Ladach);
Multimodal pain management and early mobilization;
Interdisciplinary approach in high-risk situations.
FAQ
1. In what cases is a C-section performed?
C-sections are performed for strict medical indications. Maternal indications may include complete placenta previa, threat of uterine rupture or severe eclampsia. Fetal indications are acute hypoxia, abnormal presentation (e.g., transverse) or in cases of high fetal weight combined with a narrow maternal pelvis.
2. At what term is elective C-section performed?
Elective C-section is recommended no earlier than the 39th week of pregnancy. Performing surgery at this term, rather than at 38 weeks or earlier, is necessary to significantly reduce the risk of respiratory (breathing) complications in the newborn.
3. Do you have to wait for labor when having an elective C-section?
Elective surgery is usually performed before labor (contractions) begins on a predetermined date based on medical indications.
4. How is a C-section done and how many layers are cut?
The course of C-section surgery is a layer-by-layer dissection of tissue. The surgeon makes types of incisions in the skin (usually transverse above the pubis) and in the uterus. They sequentially dissect several layers: skin, subcutaneous tissue, fascia, peritoneum and uterine wall, amniotic membrane.
5. How long does a C-section last?
A standard C-section, performed using modern gentle techniques, lasts an average of 25–35 minutes.
6. Is C-section surgery painful and which anesthesia is better?
The surgery itself is painless as it is performed under anesthesia. In elective surgeries, regional (spinal or epidural) anesthesia is considered the method of choice. It allows the patient to be alert. General anesthesia is used less frequently, mostly in emergency cases.
7. Can I have a C-section as desired?
“C-section as desired” (surgery without indication) is not recommended. Such surgery increases the risks of complications for the mother, such as infections and blood loss, and increases the risk of uterine rupture in future pregnancies.
8. Which is better: C-section or natural childbirth?
Natural childbirth is a physiologic process. C-section is a surgery performed for strict medical indications when a natural delivery is not safe for the mother or baby. Therefore, the choice (cesarean or natural childbirth) is not determined by what is better overall, but by which method is safest in a particular clinical situation. Each method has its pros and cons, which the doctor evaluates when determining the type of delivery.
9. What is the preparation for C-section and how many days in advance do you have to be hospitalized?
Preparation for C-section includes mandatory consultation with an anesthesiologist, clinical evaluation of the condition and necessary laboratory tests. The timing of hospitalization is determined by the protocols of the medical facility. This can be either 1–2 days before surgery for a full examination or on the morning of the day of intervention, if the patient’s condition allows.
10. How does recovery go and when are you discharged after a C-section?
Recovery from cesarean surgery according to modern protocols involves early mobilization (getting up after 6 hours). Regarding food in the first few days: liquids and light foods are allowed for the first 6 hours after C-section. Timing of discharge after C-section depends on the condition, but with uncomplicated course, discharge usually occurs on 3rd to 5th day.
11. How long does a scar heal after a C-section?
Primary healing of the skin scar takes 10–14 days. Full scar formation takes several months.
12. How long after a C-section is the bloody discharge?
Bloody discharge (lochia) is a normal process of cleansing the uterus and after a C-section. They can last an average of 4 to 6 weeks, gradually becoming lighter.
13. When can I have sex and exercise after a C-section?
Intense exercise is excluded for 4–6 weeks. Sexual activity after a C-section is usually recommended in 6–8 weeks after surgery, but after a gynecologist’s examination.
14. When does lactation begin after C-section?
Beginning of lactation process after C-section depends on individual factors. Early latching of the baby to the breast, possible with maternal regional anesthesia, helps stimulate lactation.
15. How many times can I have a C-section and when can I get pregnant after a C-section?
The optimal interval for getting pregnant after a C-section is at least after 18 months. There is no strict limit on how many times you can have a C-section, but multiple uterine scars increase the risks of complications in subsequent pregnancies.
References
1.
VOKA Catalogue. [Electronic resource].
https://catalog.voka.io/
2.
World Health Organization. WHO Recommendations: Non-Clinical Interventions to Reduce Unnecessary Caesarean Sections. Geneva: WHO; 2021.
3.
NICE. Caesarean Birth (NG192). National Institute for Health and Care Excellence; 2021.
4.
ACOG Practice Bulletin No. 205. Vaginal Birth After Cesarean Delivery. Obstet Gynecol. 2023.
5.
RCOG. Birth After Previous Caesarean Birth (Green-top Guideline 45). 2022.