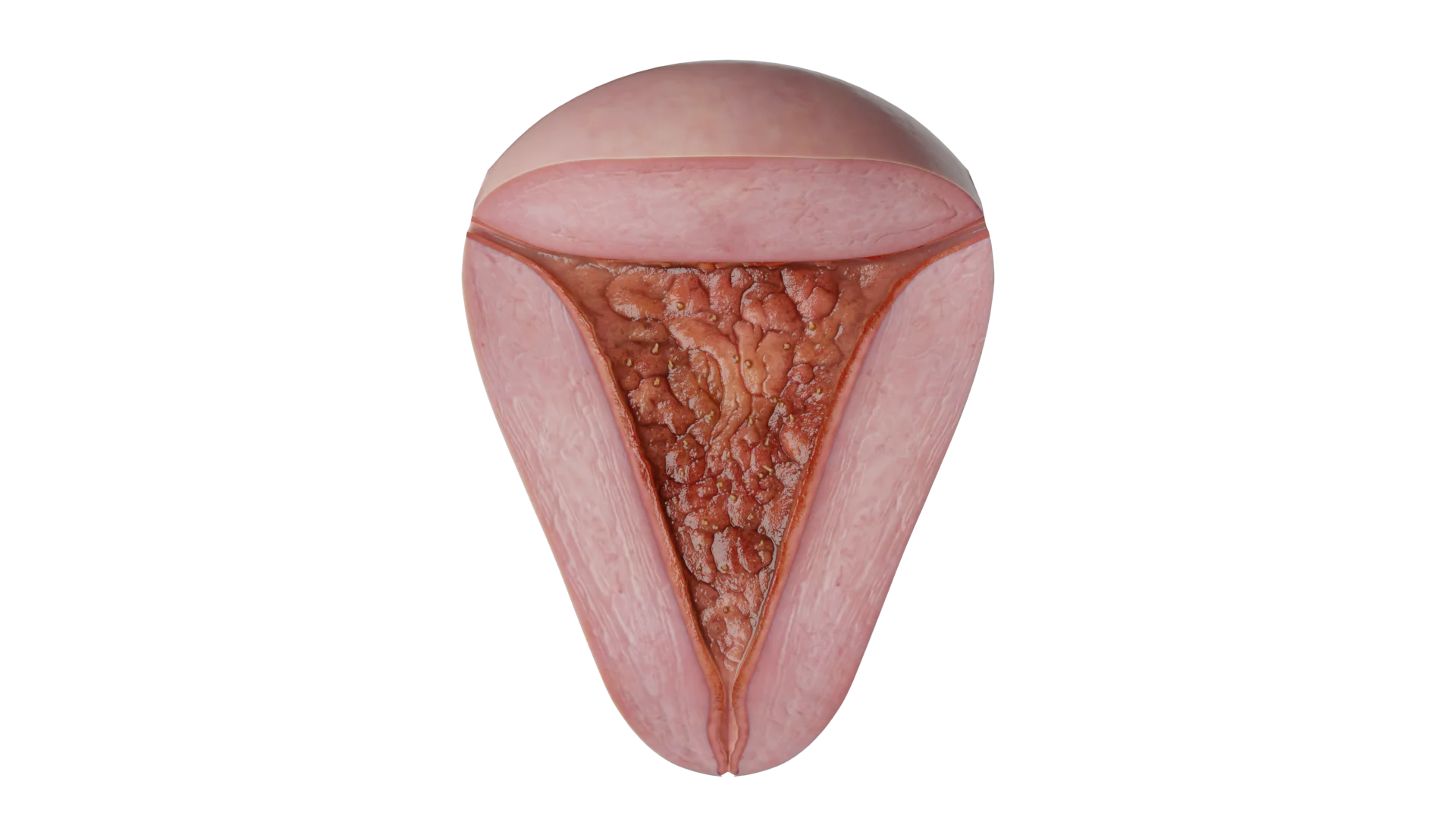
Vulvitis: Factors of Development, Clinical Manifestations, Diagnosis, Treatment
Vulvitis - inflammation of the vulva, manifested by lesions of the labia, clitoris, pubis and vaginal vestibule. Clinical manifestations, diagnosis and treatment.

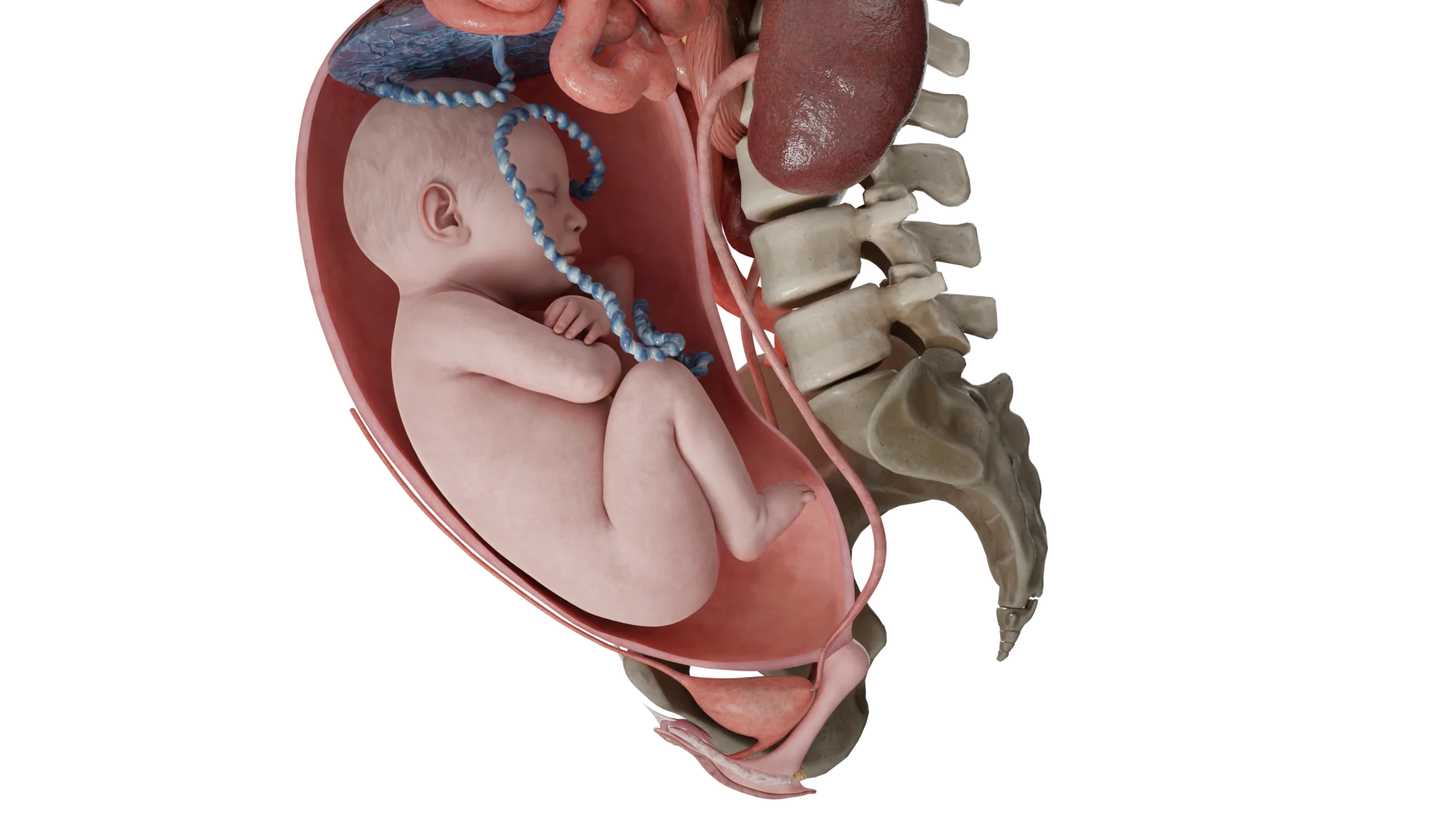
The longitudinal position of the fetus can be manifested by breech presentation, in which case the breech or legs of the fetus are the first to move through the birth canal.
The prevalence of breech presentation decreases from about 20% at 28 weeks of gestation to 3-4% by 38 weeks of gestation.
The incidence of recurrent breech presentation for repeat pregnancies is nearly 10% and 27% for third pregnancies.
There are different variations of fetal breech presentation:



The most common clinical conditions or processes that lead to breech presentation tend to affect fetal mobility or the vertical axis of the uterine cavity:
The risk of umbilical cord prolapse varies according to the type of breech presentation. The incomplete and full foot presentation has the highest risk of cord prolapse, ranging from 15% to 18%, while the breech presentation is rare, with a risk of only 0.5%.
The type of breech is clinically determined after 36 weeks of gestation. Using Leopold’s techniques during the external obstetric examination combined with cervical examination, breech presentation can be diagnosed.
During the vaginal examination, there is usually no fixation of the antecubital part, the soft tissues of the buttocks or foot may be identified. During labor, vaginal examination reveals a “soft mass” separated by a cleft between the buttocks, with possible palpation of a rigid structure, the sacrum.
After the rupture of the shells:
Clinical diagnosis can be difficult: the arm can be mistaken for a leg and the face for the buttocks. Ultrasound is the most accurate method to confirm the diagnosis. The following should be documented in the ultrasound report:
Women with confirmed breech presentation at 36 weeks or more should be reviewed to determine the method of delivery. The discussion should take into account:
The differential diagnosis includes:
Women should be informed of the fact that:
For natural childbirth, the following criteria must be met:
Three techniques for the management of vaginal delivery are described:
In the following conditions, it is customary to use the manual classic aid to facilitate the birth of the fetal head and shoulders:
An important requirement for the allowance is the delivery of the fetal body to the inferior angle of the scapulae.
The first step is the removal of the handles. The fetal legs are grasped with the opposite hand of the obstetrician, with the posterior fetal hand held at the ankles. The fetal body is tilted toward the anterior superior iliac spine of the mother, opposite the fetal back. With the second and third fingers of the same hand, the fetal pen is withdrawn with a washing motion and pressure on the ulnar crease. The other pen is manipulated in the same way.
The fetal head is withdrawn by the Morisot-Levré-Lachapelle technique. The fetal thorax is placed on the midwife’s palm. The midwife’s middle finger is inserted into the fetal mouth, and the index finger and ring finger are placed on the maxilla. The back, shoulders and occiput of the fetus are secured with the other hand, with the second finger and fourth finger placed on the shoulders and the third finger on the suboccipital fossa. Synchronously, both hands bend the head, with the fetal body directed upward. All manipulations are carried out simultaneously with pushing. Another method of withdrawal of the head according to Smelli-Fite differs in the location of the finger not in the oral cavity, but on the upper jaw.
The success rate of external obstetric fetal rotation ranges from 35% to 86%. Better success rates are associated with earlier gestational age and pure breech presentation. Opinions differ regarding the influence of maternal weight, placental position, and amniotic fluid volume. The majority of practitioners believe that in repeat mothers, patients with normal weight, posterior placental positioning, and sufficient amniotic fluid volume have an increased chance of successful turning.
The most common complication is a temporary slowing of the fetal heart rate (up to 40% of cases). This condition persists for several minutes after termination of the procedure and is not associated with adverse effects on the fetus.
Among the rare complications described are:
There is currently a paucity of studies that show whether the overall risk of perinatal mortality increases after external rotation. The 2015 Cochrane review identified the risk of perinatal death in patients who underwent external rotation as 2 out of 644 cases, compared to 6 out of 661 in the no manipulation group.
The day before, an ultrasound scan is performed to determine the fetal position, weight and volume of amniotic fluid, and to rule out placenta previa and fetal anomalies. A non-stress test (alternative: fetal biophysical profile) must be performed the day before the manipulation.
The procedure is performed in a deployed operating room with the mandatory presence of anesthesiologists-anesthesiologists-anesthesiologists. Routine tocolysis and routine use of spinal or epidural anesthesia are not recommended.
Outward turning is accomplished by gently moving the head end toward the woman’s pelvis while the pelvic end moves toward the uterine fundus. There is no consensus on how many attempts at turning can be made.
After a coup attempt, regardless of its success, a non-stress test should be repeated (biophysical profile if necessary). In addition, Rh immunoglobulin should be administered to women with Rh-negative blood.
After successful manipulation, labor should not be induced immediately. The patient is discharged home and is admitted to the maternity hospital at the onset of labor or for other indications.
Scheduled cesarean section is performed at ≥ 39 weeks’ gestation in order to facilitate optimal physiologic maturation of the fetus. Except in cases where there are indications for early delivery.
1. What is breech presentation?
2. What are the causes of fetal breech presentation?
3. What are the dangers of breech presentation?
4. How can breech presentation of the fetus be determined?
5. What are the indications for cesarean section for breech presentation?
6. How to deliver a breech baby?
7. Can the baby be turned over in a breech presentation?
8. At what term is a breech birth usually delivered?
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/2.
ACOG. Mode of term singleton breech delivery. Practice Bulletin No. 221. Obstet Gynecol. 2021;137(5):e77-e84. DOI: 10.1097/AOG.0000000000004395.
3.
RCOG. The management of breech presentation. Green-top Guideline No. 20b. 2017.
Available from: https://www.rcog.org.uk/media/4.
Cunningham FG, Leveno KJ, Bloom SL, et al. Williams obstetrics. 26th ed. New York: McGraw-Hill; 2022.
5.
Goffinet F, Schmitz T. Breech presentation: Clinical practice and evidence-based medicine. Cham: Springer; 2021.
6.
Hofmeyr GJ, Kulier R, West HM. External cephalic version for breech presentation at term. Cochrane Database Syst Rev. 2022;4:CD000083. DOI: 10.1002/14651858.CD000083.pub4.
7.
Toivonen E, Palomäki O, Huhtala H, Uotila J. Vaginal breech delivery: Is it still an option? Acta Obstet Gynecol Scand. 2022;101(3):369-376. DOI: 10.1111/aogs.14312.
8.
Ministry of Health of the Russian Federation. Clinical guidelines: Breech presentation. 2023.
Available from: https://minzdrav.gov.ru/9.
UpToDate. Breech presentation: Management. 2023.
Available from: https://www.uptodate.com/Link successfully copied to clipboard