Gastric Polyps: Etiology, Classification, Diagnosis, and Treatment Methods
Aleksandr F.Abdominal surgeon, MD
21 min read·January 29, 2026
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
In general, polyps are formations arising from the mucous membrane and protruding above it into the lumen of the organ (in this case, the stomach). This pathology requires a differentiated approach, as different types of polyps have varying potential for malignancy.
Epidemiology
Most gastric polyps are incidental findings in approximately 2% of gastroscopic studies conducted for other reasons (screenings, diagnosis of related organ diseases).
According to autopsies followed by pathological studies, gastric polyps are found in 0.3–1.1% of cases. Hyperplastic gastric polyps account for 70–90%. The disease most commonly develops between the ages of 40 and 50 but can even occur in children. Men are 2–4 times more likely to be affected than women.
Classification of gastric polyps
This pathology is typically classified based on various criteria, depending on the number of polyps, their form, morphology, location, and malignant potential.
By number
Single;
Multiple;
Polyposis (diagnosed when 20 or more neoplasms are detected in an individual).
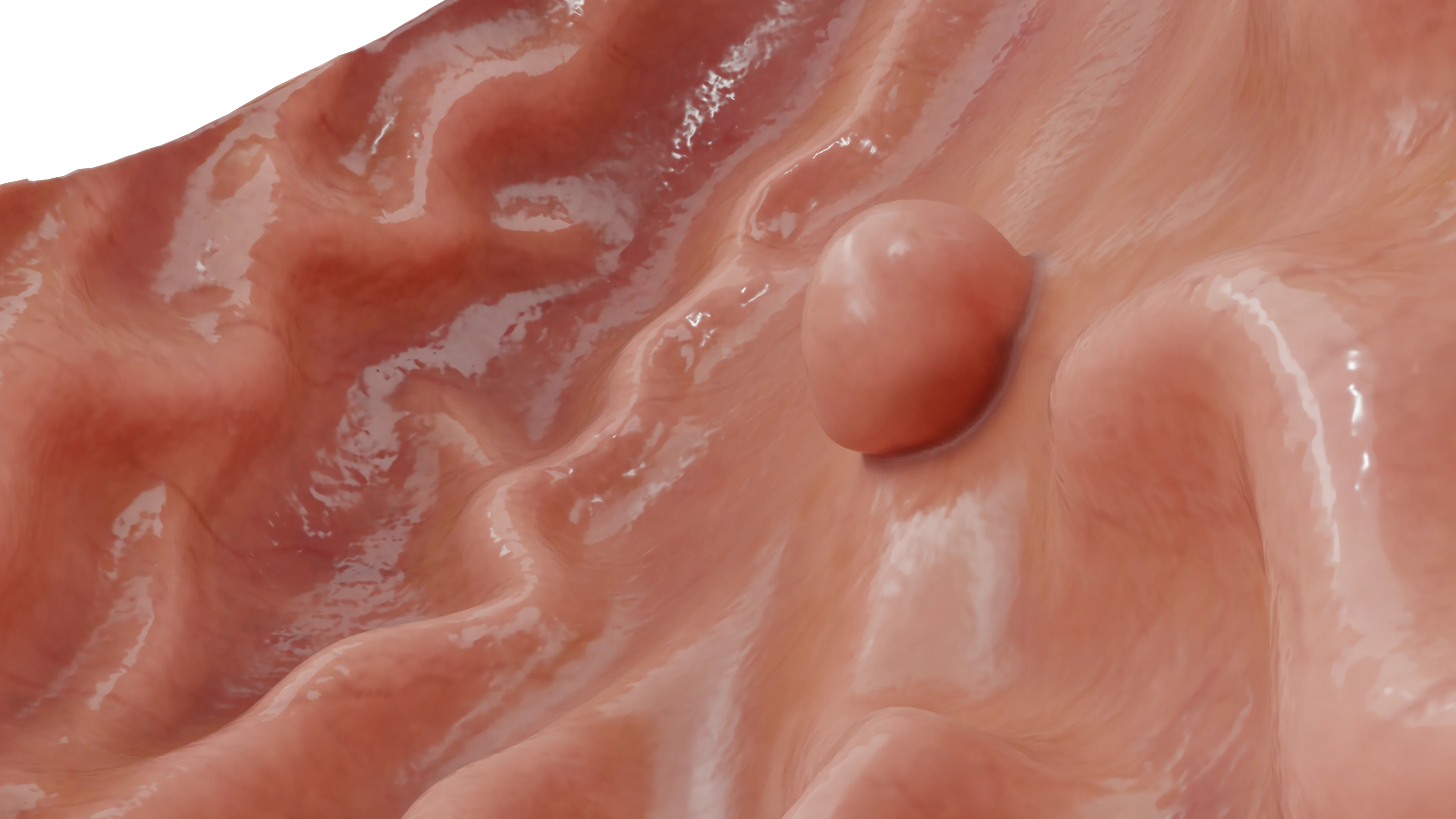
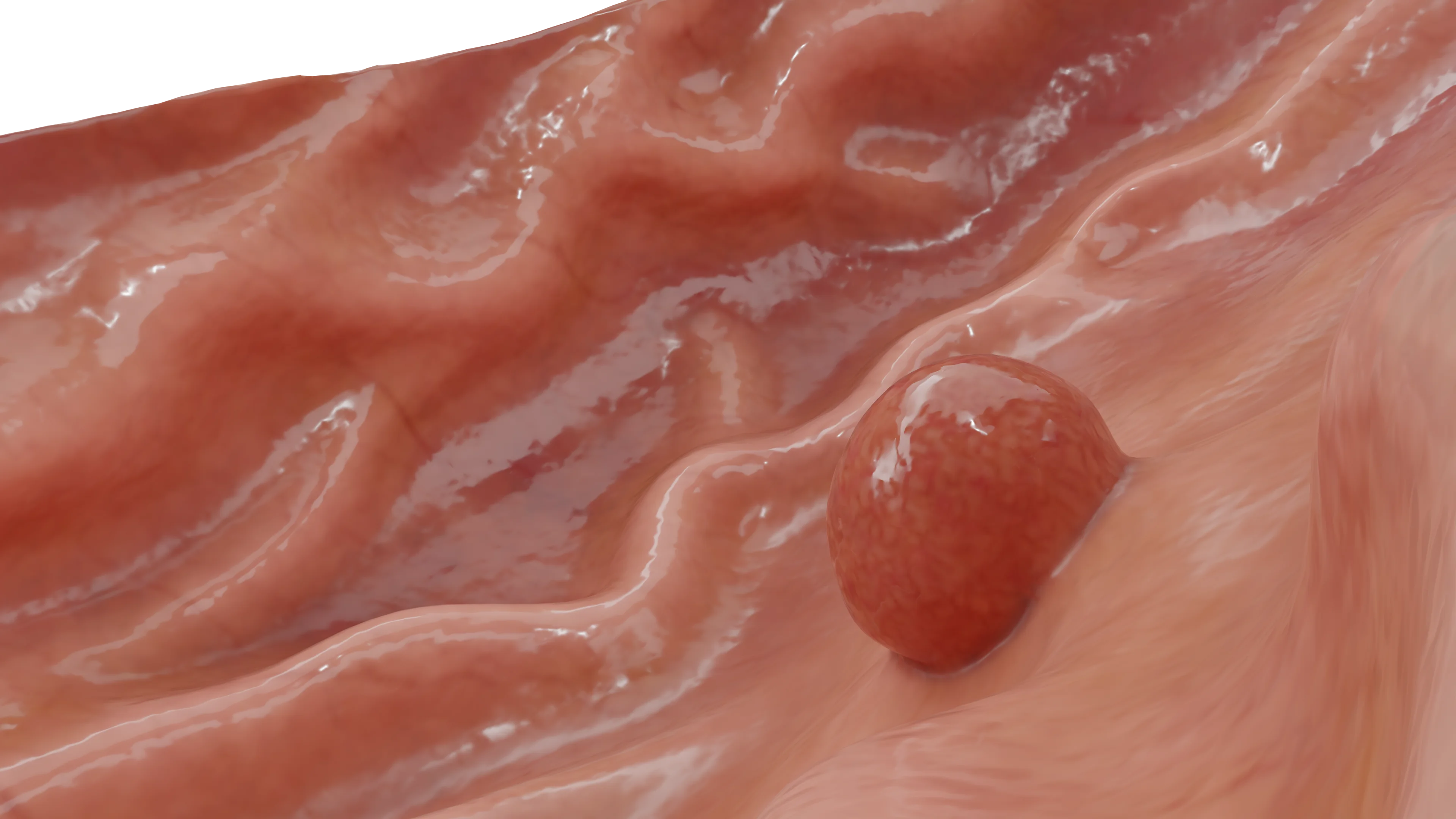
Solitary polyp in the body of the stomach: 3D modelMultiple polyps in the body and antral region of the stomach: 3D model
By macroscopic form
Type I: flat, elevated above the mucosa structures not exceeding 2.5 mm with indistinct borders;
Type II: protruding above the mucosa more than 2.5 mm, dome-shaped with clear contours;
Type III: elevated above the surface with a retracted base;
Ectopia and atypical tumors with polypoid growth (pancreatic ectopia, xanthelasmas, GISTs, lymphomas, etc.).
Etiology
The exact mechanism of polyp formation is unknown. Most likely, several mechanisms play a significant role in their formation. Three main theories of polyp development are mentioned in the literature:
Inflammatory theory: the presence of chronic inflammation in the mucous membrane (chronic gastritis, periodic ulcer exacerbations). In the context of the inflammatory process, an excessive proliferation of cells occurs to heal mucosal defects, which can form polyps.
Dysregenerative theory: this theory suggests an abnormal (distorted, with pathological composition of cellular elements) cellular response to mucosal damage, leading to the formation of excessive local cell accumulation (polyps).
Embryonic theory: according to this theory, the appearance of polyps is genetically predetermined at the embryonic development stage. During body development and throughout life, polyps appear under the influence of adverse factors.
According to a number of sources, the appearance of polyps may also be influenced by several factors with mixed or undefined etiopathogenesis:
Helicobacter pylori infection;
Long-term use of proton pump inhibitors;
Familial adenomatous polyposis;
Dietary habits;
Age (epidemiologically, it has been established that the incidence of gastric polyps tends to increase with age).
Clinical presentation
Gastric polyps usually progress without symptoms and are found incidentally during routine gastric examinations. Symptoms of an existing polyp often appear when the size of the polyp increases.
The following are among the most characteristic manifestations of a polyp:
Nonspecific discomfort in the upper abdomen (unrelated to food intake);
Feeling of heaviness or fullness in the stomach;
Anemia (up to severe anemia causing the patient to visit a physician) as a result of ulceration of the polyp and prolonged chronic blood loss may develop;
Hematemesis or melena (when the polyp is destroyed with damage to its feeding vessels, causing acute massive bleeding);
High intestinal obstruction (paroxysmal epigastric pain spreading across the abdomen, vomiting of eaten food, etc.) when especially large polyps on a narrow base penetrate the duodenum and disrupt the pyloric channel’s patency;
Secondary pancreatitis (rare reports in the literature of prolapse of large hyperplastic polyps into the duodenum, obstructing the papilla of Vater [major duodenal papilla]);
Anorexia or loss of appetite;
Nausea;
Vomiting;
Reflux esophagitis or heartburn;
Dysphagia or difficulty swallowing.
Diagnosis
As described above, polyps in the stomach are most commonly detected during an esophagogastroduodenoscopy (EGD), although diagnostic potential exists with gastric radiography (disturbance in the contour of the gastric mucosa is identified).
Ultrasound provides diagnostic value, though the sensitivity of this study is not high. It is also possible to identify this disease when performing computed tomography (CT) or magnetic resonance imaging (MRI) of the abdominal cavity (with good preparation and contrast imaging of the gastrointestinal tract).
Treatment of gastric polyps
The choice of treatment method depends on the size of the neoplasm, its histological structure, and the presence of clinical complications.
Observation strategy and conservative therapy
Small polyps (up to 5 mm) should be monitored dynamically every six months. The same strategy is applied if the patient categorically refuses polypectomy.
Some authors recommend initiating conservative treatment (eradication of Helicobacter infection, proton pump inhibitors) with a follow-up examination, since some polyps tend to decrease and disappear over time (hyperplastic polyps, fibromatous inflammatory polyps).
Endoscopic surgery
Polyps larger than 5 mm and complicated cases (erosion, gastrointestinal obstruction, or rapid polyp growth during surveillance) are indications for surgery.
When selecting a surgery method, it is essential to determine the histological structure of the polyp. Currently, the optimal and most applicable method is endoscopic polypectomy. There are several methods of such polypectomy:
Electroexcision with a loop;
Removal in the submucosal layer;
Direct coagulation of small polyps.
The choice of removal method is determined by the endoscopist, based on a combination of factors (size and location of the polyp, biopsy results, availability of equipment, and physician’s qualifications).
Patients who have undergone polyp electroexcision should perform follow-up EGDs at 3, 6, and 12 months, and thereafter it is desirable to perform endoscopy once a year.
Open surgery
Large polyps that cannot be removed endoscopically are subject to open surgery. Such cases include:
Polyps on a wide base;
Polyps with a high risk of bleeding;
In cases of malignant results from histological examination.
It is possible to perform a wedge excision of the gastric wall with the polyp, or a gastric resection to a greater or lesser extent depending on the histological conclusion and the extent of gastric involvement.
Specific types of gastric polyps and their management characteristics
Polyps with minimal risk of malignant transformation (Non-neoplastic)
They can be either on the narrow base (pedunculated) or wide base. They may be randomly distributed in any part of the stomach (24% to 60% of hyperplastic polyps are located in the antral portion of the stomach, 29% to 56.3% are in the stomach body, and only about 2.5% are in the cardia). They are more commonly found in the older age group (average age 65.5–75 years). There is a slight predisposition in females, who make up 58% to 70.5% of patients.
Hyperplastic polyps are solitary in about two-thirds of cases. Most of them measure less than 1 cm, and polyps larger than 2 cm are found in not more than 10% of cases. They are considered to result from excessive regeneration during chronic mucosal injury and, therefore, are often observed in chronic gastritis associated with Helicobacter pylori (25% of cases), pernicious anemia, adjacent to ulcers and erosions, or at gastroenterostomy sites, also in the gastroesophageal junction (in patients with gastroesophageal reflux disease, GERD).
Histologically, hyperplastic polyps exhibit significant foveolar elongation with branching formation, excessive development of the lamina propria with infiltration by plasma cells, lymphocytes, eosinophils, mast cells, macrophages, and varying amounts of neutrophils. Gastric glands are usually not involved in the formation of polyps. Over time, hyperplastic polyps can either increase or regress (spontaneously or after eradication of Helicobacter pylori). Malignant transformation is extremely rare (1.5%–3% of cases, typically when larger than 2 cm). Therefore, larger polyps should be completely resected endoscopically.
These polyps are characterized by an increase in the number of spindle-shaped cells, inflammatory cells, and small vessels, often with a predominance of eosinophils. Such polyps occur throughout the gastrointestinal tract but are most frequently localized in the antropyloric region (80%).
Etiology suggests an allergic cause, and there is also noted an association with hypochlorhydria or achlorhydria (with atrophic gastritis). They are diagnosed in both men and women of any age equally. Inflammatory fibrous polyps are usually located in the submucosa, although cases of involvement only of the mucosa have been described. They consist of small blood vessels, surrounded by short spindle-shaped cells, which may be arranged like “onion peel” around larger vessels.
Multinucleated giant cells, resembling “flowers,” with hyperchromatic nuclei, are sometimes observed. All described structures are surrounded by a chronic inflammatory cell infiltrate with a predominance of eosinophils. Such polyps are accidentally diagnosed and have no distinctive symptomatology, usually not recurring after resection (therefore, endoscopic removal is considered adequate treatment).
Xanthoma/Xanthelasma
These clinically insignificant lesions are detected more often in men with age than in women and are associated with chronic gastritis, gastropathy, and duodenogastric bile reflux. Macroscopically, they appear as single or multiple lesions 1 to 2 mm in diameter, round or oval, clearly defined, yellow, spotted, or nodular lesions.
They most commonly occur along the lesser curvature. Histologically, they consist of aggregates of mature macrophages loaded with lipids, occupying the lamina propria, and containing cholesterol and neutral fat.
Hamartomatous polyp of Peutz-Jeghers type
The gastric mucosa may be involved in Peutz-Jeghers polyposis (although involvement of the small and large intestines is more characteristic). This type of polyp consists of hyperplastic glands lined with foveolar-type epithelium and separated by smooth muscle cells with atrophy of deep glandular components.
Juvenile polyp
Juvenile gastric polyps are rare and often arise in the context of juvenile polyposis of either just the stomach or the entire gastrointestinal tract (with or without a family history). They may occur at any age, usually presenting with anemia or hypoproteinemia, and are most commonly found in the antrum. They consist of edematous mucosa with inflammatory changes, marked elongation, tortuosity, and cystic dilatation of foveolar zones (thus they may be mistakenly identified as hyperplastic polyps).
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Neoplastic polyps (having a risk of malignant transformation)
Fundic gland polyps
Fundic gland polyps (FGPs) are small sessile lesions that occur exclusively in the fundus and upper part of the body of the stomach. FGPs occur sporadically, although they are found in patients with familial adenomatous polyposis.
Endoscopically, they appear as translucent, sessile polyps less than 1 cm in diameter, usually multiple. They can be detected in men and women of any age in equal proportions of cases. There is a documented association of FGPs with proton pump inhibitor therapy (for more than 36 months), which, according to some authors, is a subject of debate.
In most cases, activating somatic mutations are identified (in phosphorylation sites of GSK-3β) of exon 3 of the gene β-catenin in the foveolar and glandular epithelium. FGPs are composed of cystically dilated glands lined with fundic epithelium, mixed with normal glands, and may include smooth muscle cells distributed diffusely and chaotically around the cystic glands.
Adenoma (adenomatous polyp)
The World Health Organization (WHO) defines gastric adenomas as circumscribed polypoid lesions composed of tubular and/or villous structures lined by dysplastic epithelium. The prevalence of gastric adenoma ranges from 0.5% to 3.75% in countries of the Western Hemisphere, whereas in countries with a high risk of gastric cancer, it ranges from 9% to 20%.
Their frequency increases with age, and there is also an increased occurrence in individuals with familial adenomatous polyposis. They usually arise in the context of atrophic gastritis with intestinal metaplasia, and most of them are identified in the antral region, with the gastric angle and fundus being the second most common sites.
Most of them are single, exophytic lesions (either sessile or on a narrow base). They rarely may be “flat” or even depressed below the contour of the surrounding mucosa. Most commonly, they are 3 to 4 cm in size. Gastric adenomas usually have a velvety, lobulated surface contrasting with the smooth and atrophic adjacent mucosa.
Gastric adenomas can be graded according to the degree of dysplasia (low or high grade) based on nuclear crowding, hyperchromasia, mitotic activity, cytoplasmic differentiation, and degree of disrupted architectural pattern. Small pedunculated adenomas less than 1 cm usually consist of poorly differentiated tubular dysplastic epithelium.
Larger adenomas are more often villous with a high degree of dysplasia, and a significant proportion carry a carcinomatous transformation. Malignancy in lesions larger than 2 cm reaches 40–50%. As they are pre-invasive neoplasms with a potential to progress to adenocarcinoma, gastric adenomas should be treated by local removal, typically endoscopic polypectomy or endoscopic mucosal resection.
The WHO defines gastric carcinoids as well-differentiated endocrine neoplasms consisting of non-functioning enterochromaffin-like cells arising in the acid-producing mucosa of the body or fundus of the stomach.
Gastric carcinoids are rare, accounting for less than 0.5% of all stomach neoplasms (more common in patients with autoimmune atrophic gastritis with associated Zollinger-Ellison syndrome, sometimes sporadically). Tumors are solitary and may have features similar to those of carcinoma (such as gastrointestinal bleeding, obstruction, or metastases). Gastric carcinoids show characteristic ribbon or trabecular patterns with island-style organization. Large carcinoid tumors can metastasize to the lymph nodes and liver, as well as more distant organs. However, their growth is usually slow.
Size and invasiveness correlate best with the likelihood of metastasis. Carcinoids smaller than 2 cm and multiple have a very low risk of metastasis, whereas tumors less than 1 cm in diameter may remain stable for many years, often without growth.
It is recommended to resect tumors larger than 2 cm in diameter, as they have a significant risk of lymphatic invasion and metastasis. The treatment of multiple small surface carcinoids is more challenging; meticulous endoscopic removal is possible, but some authors recommend gastric resection or antrectomy (this eliminates hypergastrinemia and induces regression of hyperplastic lesions and possibly carcinoid involvement).
FAQ
1. What are gastric polyps?
They are formations originating from the mucosa and protruding above its surface into the organ’s lumen. Essentially, they are benign tumors that require medical monitoring due to the risk of potential malignancy.
2. What causes polyps in the stomach?
The primary factor is considered to be chronic inflammation of the mucosa with gastritis or peptic ulcer disease, during which cells begin to proliferate excessively in the process of tissue healing. Their development is also influenced by genetic predisposition, infection with the bacterium Helicobacter pylori, and long-term use of proton pump inhibitors.
3. What symptoms may indicate the presence of polyps?
Usually, such formations are asymptomatic and are detected accidentally. However, with an increase in size or the development of complications, symptoms such as a feeling of heaviness or dull pain in the abdomen, symptoms of gastrointestinal bleeding and anemia, nausea, vomiting, heartburn, and dysphagia may appear.
4. Do gastric polyps always progress to cancer?
The risk of malignancy directly depends on the histological type. Hyperplastic and inflammatory types very rarely undergo malignant transformation. The greatest danger is posed by adenomatous polyps, the risk of transformation into cancer of which with a size greater than 2 cm reaches 40–50%.
5. Can polyps be cured without surgery, and can they disappear on their own?
Certain types, such as hyperplastic or inflammatory polyps, can decrease or completely disappear with conservative therapy. Physicians often recommend a course of Helicobacter pylori eradication followed by endoscopic monitoring of dynamics.
6. In what cases is polyp removal necessary?
Surgery is indicated for a size greater than 5 mm, rapid growth, development of complications (bleeding, erosion), or poor biopsy results. Adenomatous polyps require removal regardless of size due to the high risk of transformation into adenocarcinoma.
7. How is the procedure for removing polyps carried out?
The main method is endoscopic polypectomy during gastroscopy using electrosurgery or coagulation methods. In cases where endoscopic access is impossible due to a large size or a wide base of the polyp, open surgeries are performed, such as resection or wedge excision of the stomach wall (quite rarely).
8. What diet is necessary for gastric polyps?
There is no specific diet against the polyps themselves. It is recommended to adhere to a gentle diet excluding spicy and fried foods and alcohol, to reduce mucosal irritation and manage accompanying chronic gastritis.
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Abraham SC, Park SJ, Lee JH, Mugartegui L, Wu TT. Genetic alterations in gastric adenomas of intestinal and foveolar phenotypes. Mod Pathol. 2003;16: 786–795.
3.
Bosman FT, Carneiro F, Hruban R, Theise N (2010) WHO Classification of Tumours of the Digestive System, (4th edn), International Agency for Research on Cancer (IARC), Lyon, 2010.
4.
Delle Fave G, Kwekkeboom DJ, Van Cutsem E, Rindi G, Kos-Kudla B, et al. (2012) ENETS Consensus Guidelines for the Management of Patients with Gastroduodenal Neoplasms. Neuroendocrinology 95: 74–87.
5.
Lim SA, Yun JW, Yoon D, Choi W, Kim SH, et al. (2011) Regression of hyperplastic gastric polyp after Helicobacter pylori eradication. Korean J Gastrointest Endosc 42: 74-82.
6.
Pantanowitz L, Antonioli DA, Pinkus GS, Shahsafaei A, Odze RD. Inflammatory fibroid polyps of the gastrointestinal tract: evidence for a dendritic cell origin. Am J Surg Pathol. 2004;28:107–114.
7.
Park DY, Lauwers GY (2008) Gastric polyps: classification and management. Arch Pathol Lab Med 132: 633-640.
8.
Ramage JK, Ahmed A, Ardill J, Bax N, Breen DJ, et al. (2012) Guidelines for the Management of Gastroenteropancreatic Neuroendocrine (Including Carcinoid) Tumours (NETs). Gut 61: 6–32.
9.
Torbenson M, Lee JH, Cruz-Correa M, et al. Sporadic fundic gland polyposis: a clinical, histological, and molecular analysis. Mod Pathol. 2002;15:718– 723.
10.
Belonogov A.V., Zhitov D.I. “Endoscopic and endosurgical methods of treating stomach polyps” (in Russian), Bulletin of Siberian Branch, Russian Academy of Medical Sciences, vol. 2, No. 5, pp. 76–79, 2002.
11.
Blok B., Schakhmal G., Shmidt G. Gastroscopy. (In Russian) Moscow: MED press-inform, 2007, 216 p. (Trans. from Ger. under general editorship of I. V. Maev, S. I. Emelyanov).
12.
Tereshchenko S.G. Optimization of intra-organ interventions for the prevention of bleeding in operative endoscopy for digestive tract diseases (in Russian). Moscow: Moscow Regional Research and Clinical Institute, 2015. — 23 с.
13.
Khomyakov V.M., Ermoshina A.D., Pirogov S.S., Ryabov A.B. “Modern views on risk factors for gastric cancer” (in Russian), Russian Journal of Gastroenterology, Hepatology and Coloproctology, vol. 27, no. 6, pp. 78–86, 2017.