Goiter: Classification, Etiology and Methods of Treatment
Svetlana D.Surgical oncologist, MD
11 min read·December 11, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Goiter is a general term that is used to describe abnormalities of the thyroid gland, manifested by an increase in its size and volume. The volume of the thyroid gland normally does not exceed 18 cm³ in women and 25 cm³ in men. Goiter is 4–5 times more common in women than in men.
Goiter can be physiological (in puberty, pregnancy, and lactation periods) or pathological. Physiological enlargement of the thyroid gland is due to an increase in the body’s need for thyroid hormones, is temporary and, as a rule, does not require treatment.
There are several classifications of goiter depending on etiology, epidemiology, anatomy, as well as functional or morphological features.
By etiology and epidemiology
Physiologic enlargement is due to the body’s increased need for thyroid hormones (puberty, pregnancy, lactation).
Pathologic goiter occurs as a consequence of thyroid disease.
Endemic goiter, revealed in a large population, is caused by iodine deficiency.
Sporadic goiter occurs in non-endemic regions.
Familial (hereditary) goiter is caused by the presence of a genetic defect in thyroid hormone synthesis.
By structure and function
Morphological structure:
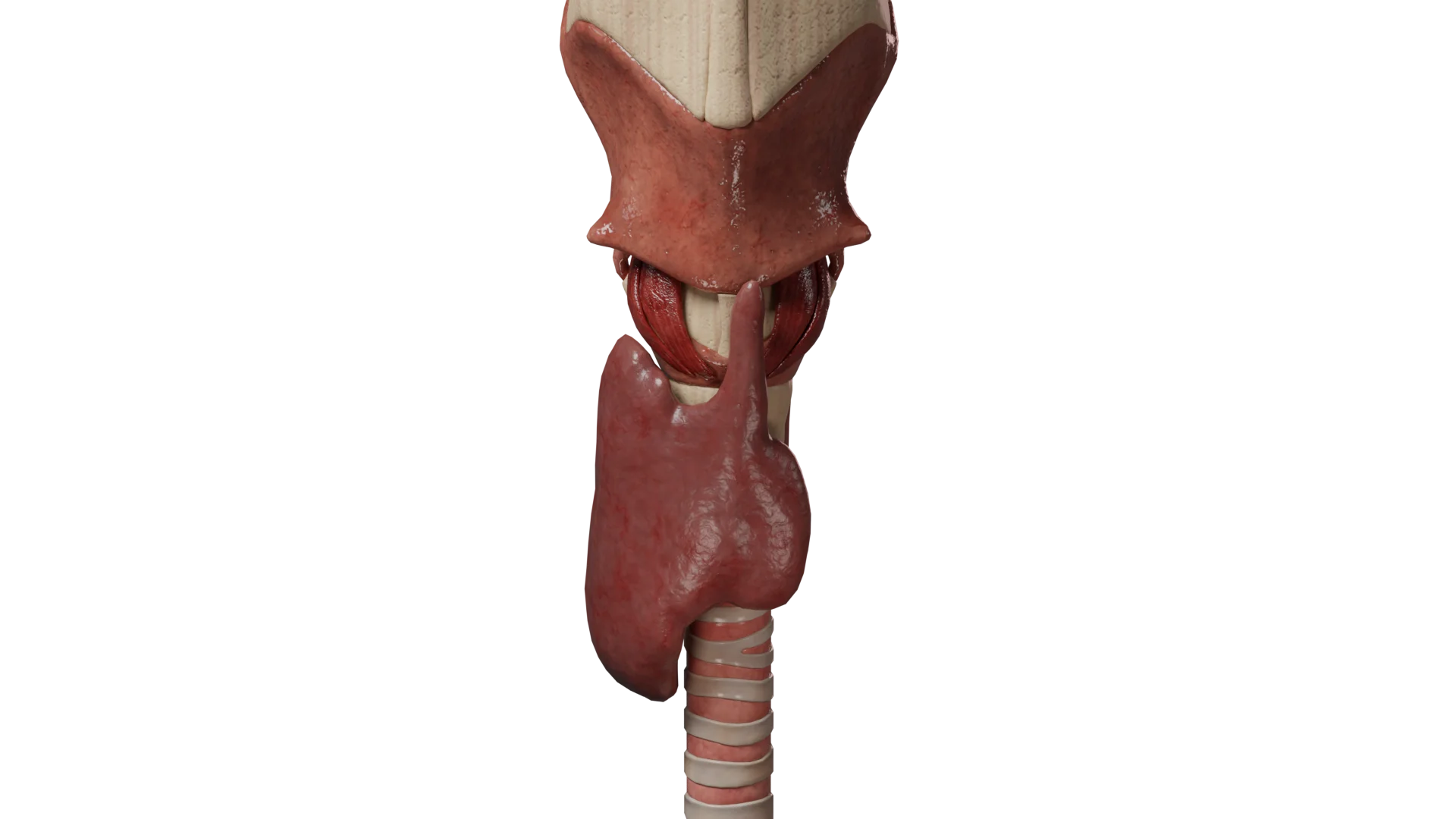
Diffuse goiter: thyroid gland is uniformly enlarged.
3D animation: diffuse goiter
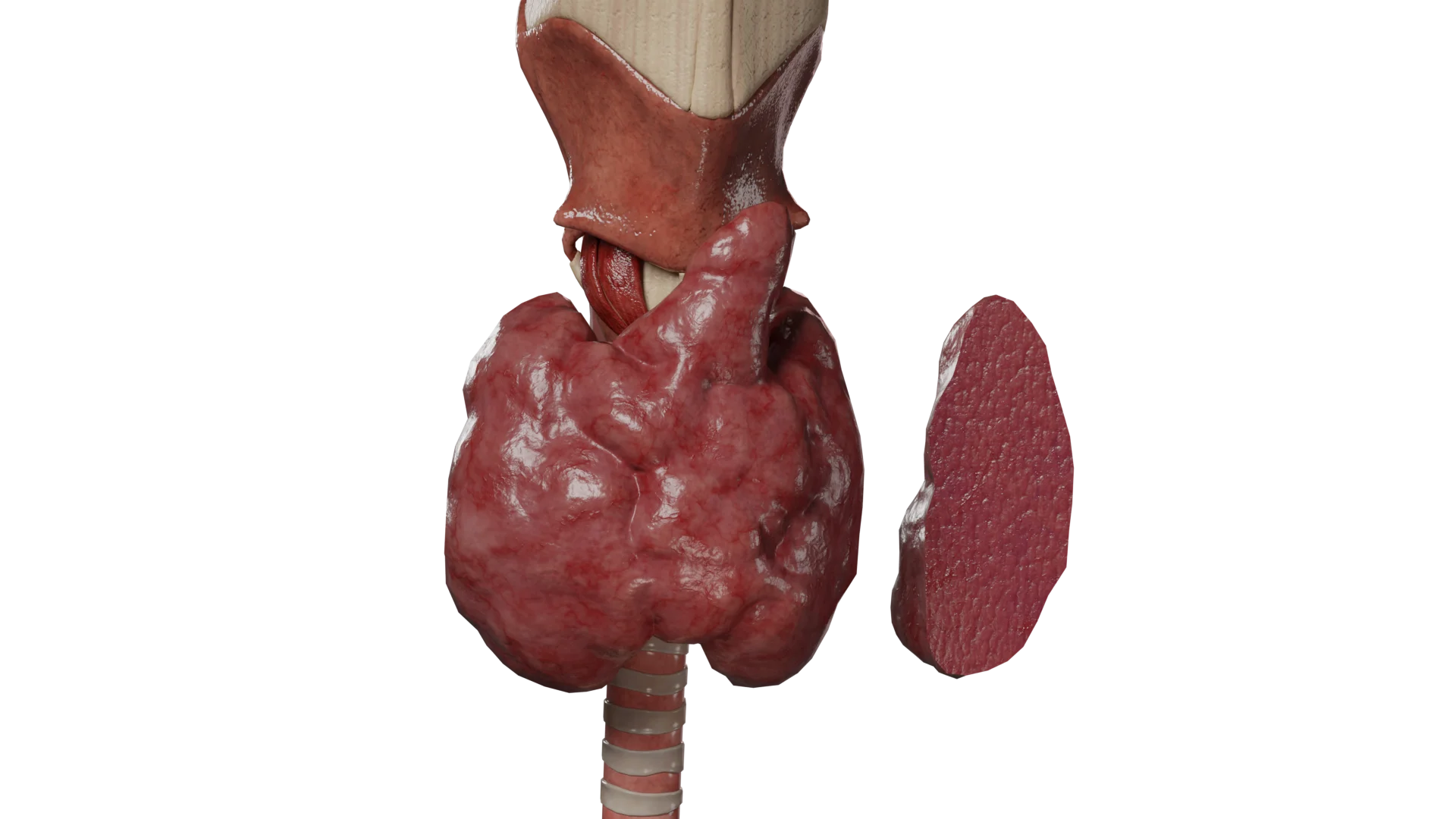
Nodular goiter: enlargement is due to a solitary nodular mass.
3D animation: nodular goiter
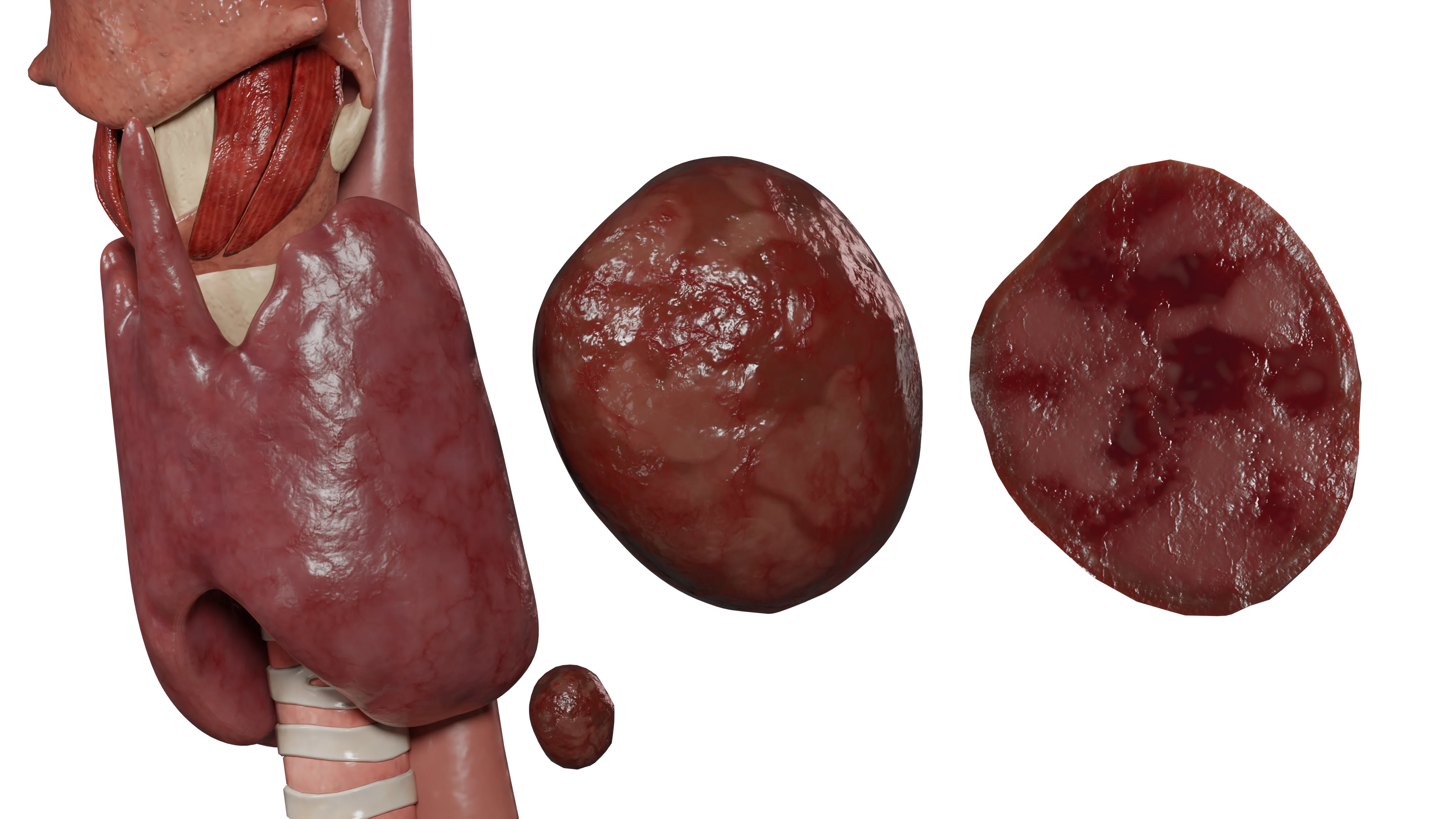
Multinodular goiter means the presence of multiple (2 or more) nodules.
3D animation: multinodular goiter
Function:
Nontoxic goiter (euthyroid goiter): function is normal (euthyroidism) or reduced (hypothyroidism).
Toxic goiter: thyroid hormone levels are elevated.
Anatomy:simple goiter (on the neck) or retrosternal goiter (located below the jugular notch).
By stage (degrees of enlargement)
Stage 0: thyroid gland is not enlarged (no goiter).
Stage I: thyroid gland is enlarged on palpation, neck contour is not deformed with normal neck position.
Stage II: enlargement of the thyroid gland is detected both by palpation and visually (deformation of the neck contour with its normal position).
Etiology and pathogenesis of goiter
Causes
The most common cause of goiter is iodine deficiency.
Iodine deficiency: reduced iodine intake increases the risk of goiter.
Thyroid diseases: goiter can result from autoimmune, inflammatory, or tumor lesions.
Genetic abnormalities: mutations in NIS, thyroperoxidase, DUOX2, and other genes have been identified.
Goitrogens: administration of drugs (lithium, amiodarone) and foods (cabbage, sorghum).
Other factors: exposure to ionizing radiation, insulin resistance, metabolic syndrome.
Pathogenesis
The goiter is an adaptive response of the follicular cells of the thyroid gland to a process that blocks thyroid hormone production.
Mechanism: iodine deficiency leads to decreased hormone production. In response, the pituitary gland increases secretion of TSH.
Outcome: elevated levels of TSH lead to follicular cell stimulation, thyroid hyperplasia, and goiter formation.
Clinical presentation and symptoms of goiter
The clinical presentation of goiter is due to two syndromes: the syndrome of compression of surrounding organs and tissues due to the increase in the size of the gland and the syndrome of endocrine dysfunction. The vast majority of patients are euthyroid and have no complaints.
Compression syndrome
Includes symptoms such as persistent fever and a feeling of a lump in the throat, impaired phonation, dysphagia, increasing dyspnea, and neck contour deformity. Since the volume of the thyroid gland typically increases slowly, these symptoms develop gradually and patients do not have any complaints for a long time.
Endocrine dysfunction syndrome
Clinical manifestations are due to the development of hypo- or hyperthyroidism. The vast majority of patients are euthyroid and have no complaints.
Hypothyroidism (nontoxic goiter): rapid fatigue, lethargy, apathy, drowsiness, emotional lability, brittle nails and hair, dry skin, swelling, increased body weight, decreased libido, irregular menstruation in women.
Hyperthyroidism (toxic goiter): tachycardia, arrhythmias, decreased body weight with increased appetite, emotional lability, increased sweating, hand tremors.
Diagnosis and treatment of goiter
Diagnostic methods
History taking
The facts of living in iodine deficiency endemic areas, previous exposure to ionizing radiation, hereditary history, taking medications that affect thyroid function are important.
Examination and palpation
They allow assessing the size of the gland. On examination, patients with stage 2 goiter will have a deformed neck contour with a normal neck position, and the skin is usually of normal color.
On palpation, the thyroid gland is enlarged in size, has elastic consistency, and is painless and mobile relative to the surrounding tissues.
In case of nodular/multinodular goiter, single or multiple elastic painless round-shaped masses are detected on palpation in the thyroid tissue.
Laboratory diagnostics
Determination of thyroid hormone levels in serum (T3, T4, free T3, free T4, TSH, TG, TPOAb, TTHAb, TGAb).
Ultrasound
It is the primary method of thyroid imaging. It allows assessing the location, size of the organ, the presence of nodal pathology.
The Thyroid Imaging Reporting and Data System (TI-RADS) is currently used to evaluate nodal masses.
Ultrasound classification (TI-RADS)
TI-RADS
Risk of malignancy, %
Description
TI-RADS 1
0
No nodal pathology
TI-RADS 2
0
Colloid nodule of types I, II, III
TI-RADS 3
< 5
Hyper-, iso- or hypoechoic nodules with partially formed capsule (Hashimoto’s pseudo nodules)
TI-RADS 4a
5 – 10
Solid or mixed hyper-, iso- or hypoechoic nodule with thin capsule with or without calcifications
TI-RADS 4b
10 – 80
Hypo-, iso- or hyperechoic nodule, with irregular contour, without a clear border with normal parenchyma, with the presence of microcalcifications
TI-RADS 5
> 80
Iso- or hypoechoic nodule, without capsule, with multiple calcifications, with increased vascularization
TI-RADS 6
100
Malignant nodule previously confirmed by biopsy results
Additional visualization
CT/MRI and scintigraphy are used as methods of clarifying and functional diagnostics.
Fine-needle aspiration (FNA) biopsy
It is used for differential diagnosis of nodal masses.
It’s performed under ultrasound control. The procedure does not require special preparation and anesthesia.
Complications: subcutaneous hematoma, local soreness, local inflammation. They are rare, usually do not require treatment and resolve on their own within a few days.
Differential diagnosis
It is performed with lymphoma, thyroid cancer, parathyroid adenoma, median neck cyst, vascular malformations, abscess and lymphadenopathy. Diagnosis is made with help of ultrasound, CT, MRI and FNA biopsy followed by cytological examination of the punctate.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Treatment and prognosis
Nontoxic goiter (stage 1): in euthyroidism and absence of complaints does not require treatment, but is subject to annual observation with mandatory ultrasound and assessment of thyroid status.
Hypothyroidism: hormone replacement therapy with levothyroxine sodium is indicated. The dose is selected individually and adjusted under the control of TSH levels, free T4.
Stage 2 goiter / compression syndrome: generally require surgical treatment.
Surgical treatment: indicated for nodular and multinodular goiter (hemithyroidectomy or thyroidectomy).
Prognosis: the prognosis in patients with diffuse and nodular forms of goiter is favorable.
FAQ
1. What is goiter in simple words?
A goiter is an increase in thyroid volume above normal size (more than 18 cm³ in women, 25 cm³ in men).
2. Can colloid goiter progress to cancer?
Colloid goiter is considered a benign process. The risk of developing thyroid cancer in colloid goiter patients is less than 5%.
3. What are the risks of Graves disease (GD)?
Graves disease (GD) is dangerous for developing hyperthyroidism, which can lead to serious complications including heart rhythm disorders, heart failure, and thyroid crisis (thyroid storm).
4. How to treat goiter in women if hormone levels are normal (euthyroidism)?
Stage 1 euthyroid goiter without complaints does not require treatment, but should be monitored. If the goiter is nodular or causes compression syndrome, surgical treatment may be required.
5. What is stage 1 nodular goiter, and what does it mean by TI-RADS?
Stage 1 nodular goiter means that the patient has a nodular mass with a small degree of enlargement of the thyroid gland. According to TI-RADS, nodules may be categorized as low or high risk of malignancy.
6. Why is goiter more common in women?
Goiter is 4–5 times more common in women than in men, which is due to hormonal factors (pregnancy, lactation), as well as a higher prevalence of autoimmune thyroid diseases in the female population.
References
1.
VOKA Catalog. [Electronic resource].
https://catalog.voka.io/
2.
Ahmed S Can, Rehman A. Goiter. [Internet].
https://www.ncbi.nlm.nih.gov/books/NBK562161/
3.
World Health Organization. Goitre as a determinant of the prevalence and severity of iodine deficiency disorders in populations. [Internet].
S. V. Novosad, M. O. Rogova, N. S. Martirosyan, N. A. Petunina, “Modern prognostic models of thyroid cancer risk stratification”. Doktor.Ru, vol. 8(125), pages 52–56, 2016. [in Russian] (Новосад С. В., Рогова М. О., Мартиросян Н. С., Петунина Н. А. Современные прогностические модели стратификации риска рака щитовидной железы. Доктор.Ру. 2016;8(125):52–56).