Systemic Enamel Hypoplasia: Etiology, Classification, Clinical Presentation, and Treatment
Developmental Enamel Defects: Systemic Hypoplasia. Overview of the Etiology, Clinical Forms, Diagnosis, and Aesthetic Restoration Techniques for Teeth.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
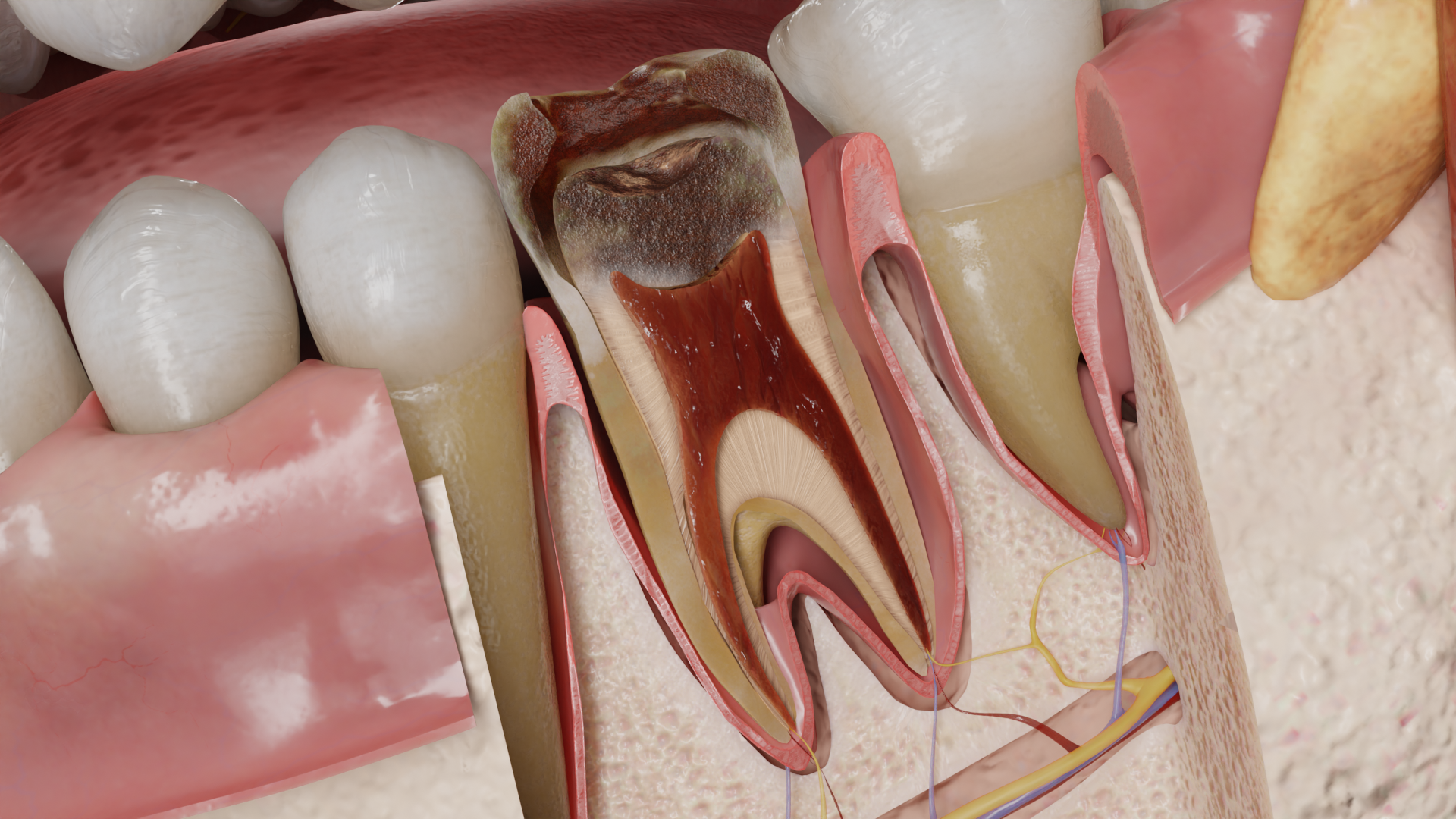
Reversible pulpitis is a clinical diagnosis based on objective and subjective signs of the presence of mild inflammation in the pulp tissue. If the cause of inflammation is eliminated, the pulp returns to normal.
Reversible inflammation of the pulp may be the result of a carious process, recent dental treatment, or trauma.
Tooth decay is the main cause of inflammatory damage to the pulp. Inflammatory changes in the pulp are observed at all stages of the active carious process. Toxins, bacterial metabolic products, proteolytic enzymes and dentin dissolution products make their way to the pulp through the dentinal tubes. In response, local infiltration of the pulp tissue by macrophages, plasma cells, and lymphocytes occurs. Pulp irritation leads to activation of nonspecific inflammatory reactions with release of histamine, bradykinin and arachidonic acid metabolites. Lysosomal enzymes of polymorphonuclear leukocytes and protease inhibitors are also released. There is overgrowth of terminal portions of afferent pulp fibers with the release of pro-inflammatory neuropeptides causing vascular responses:
The pulp can be irritated by mechanical, chemical and thermal factors such as:
The following factors irritate the pulp during dental treatment:
Polymerization shrinkage of the filling material in case of violation of the technique of direct restoration leads to tearing of the material from the tooth tissues, loss of tightness of the restoration promotes microfluidation of microorganisms into the dentinal tubes and development of pulp inflammation.
Mechanical, thermal, and chemical stimuli result in rapid fluid movement in the dentinal tubules. This stimulates the myelinated A𝛅 nerve fibers of the pulp. They have high nerve impulse conduction speed and low stimulation threshold, are located superficially at the junction of pulp and dentin, transmit pain directly to the thalamus and generate sharp, stabbing localized pain.
The pulp of the tooth has increased sensitivity to damaging influences and difficult regeneration, because it is in a confined space without the possibility of expansion, and has insufficient collateral circulation. However, when exposed to a weak and/or brief stimulus, the pulp can mobilize protective responses leading to healing with minimal damage.
In response to irritation, the following reactions are activated:
The toxic effect is reduced by the constant flow of dentinal fluid and its buffer capacity. All these mechanisms are aimed at decreasing permeability and reducing the possibility of irritants entering the pulp.
Inflammation of the pulp can regress if the infected dentin is removed and the damaging factor is eliminated. Aspirated odontoblast nuclei can be subjected to autolysis.
The resulting tertiary dentin remains as a “scar” after previous inflammation.
Depending on the cause of pulp irritation, the affected tooth may have:
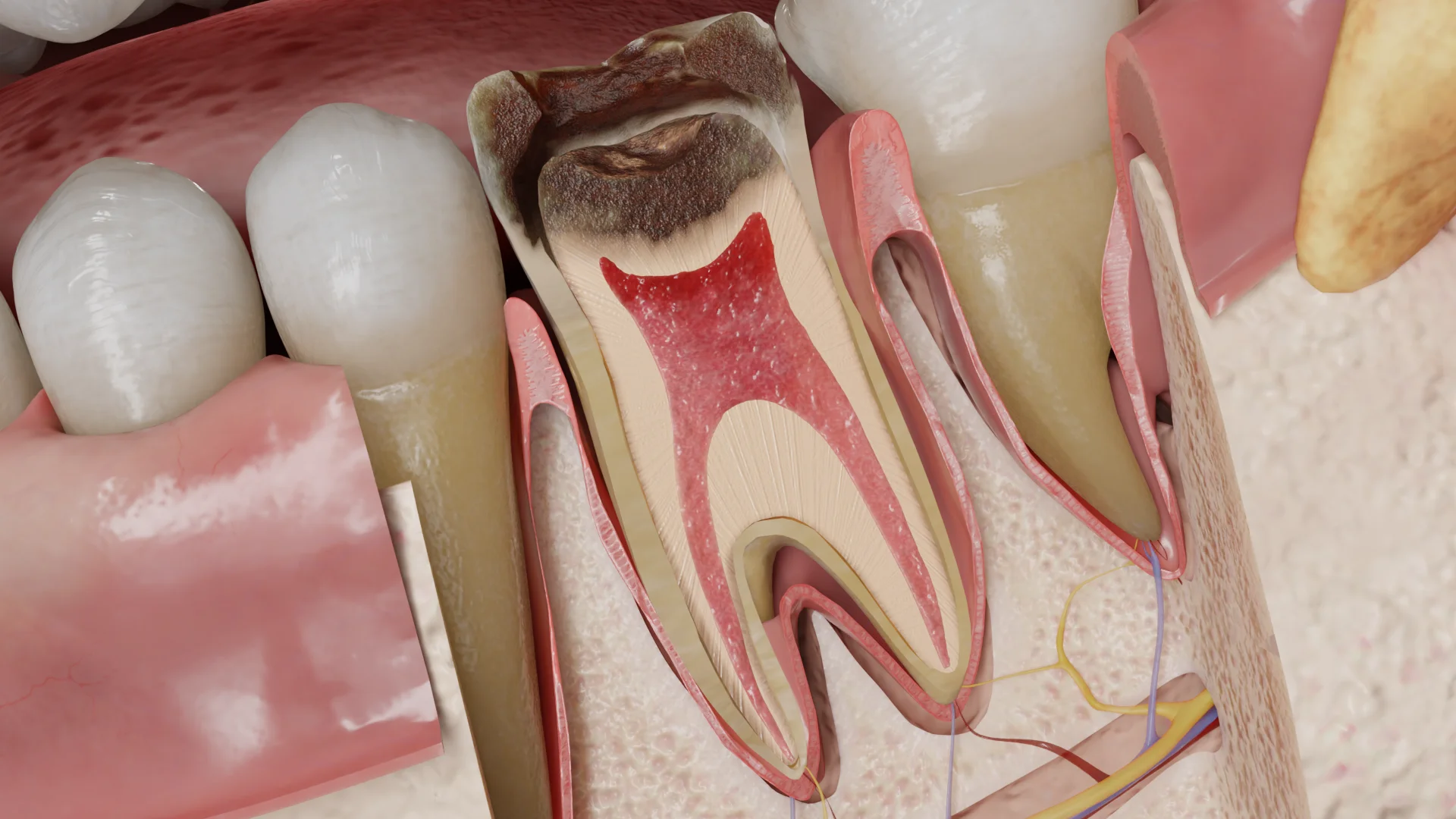
Tissue of the crown pulp in the peripheral parts is edematous, hyperemic. At the border of dentin and pulp in the projection of the carious lesion may be observed deposition of tertiary dentin.
To date, no 100% accurate clinical methods have been found to reliably analyze the condition of the pulp tissue. Apart from pain, the other classic signs of inflammation (redness, swelling, fever, loss of function) cannot be determined because the pulp is not accessible for direct examination. In an inflamed pulp, the clinical symptoms usually do not correspond to the histologic picture.
Clinically, it is often very difficult to distinguish between reversible and irreversible pulp inflammation. The patient may complain of sharp, rapidly passing pain from cold or hot things, or there may be no complaints.
Exposure to a stimulus, such as cold or hot liquid or air, can cause acute pain. Removal of the stimulus causes the pain to disappear immediately or within a few seconds.
Find more scientifically accurate content on our social media








Treatment is aimed at eliminating the irritant and sealing the exposed dentin and/or vital pulp.
In the presence of carious process – preparation and careful necrectomy of infected dentin with subsequent restoration.
In traumatic injuries – restoration of lost tissue, direct coverage of the exposed vital pulp with biocompatible material, or partial pulpotomy.
Further dynamic observation with periodic control of pulp vitality is carried out. The patient should be warned about the possible development of irreversible inflammation and necrosis of the pulp, as well as the need to seek dental care if symptoms of irreversible pulpitis (prolonged pain from temperature stimuli, spontaneous pain) occur.
1. What is reversible pulpitis?
2. What are the causes of reversible pulpitis?
3. Why can pulp inflammation be reversible?
4. What is the difference between reversible pulpitis and irreversible pulpitis?
5. Can reversible pulpitis become irreversible?
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Berman, L. H., & Hargreaves, K. M. (2020). Cohen’s Pathways of the Pulp Expert Consult. Elsevier.
3.
Torabinejad, M., Fouad, A., & Shabahang, S. (2020). Endodontics: Principles and Practice. Elsevier.
4.
American Association of Endodontists. (2019, June 3). Guide to Clinical Endodontics – American Association of Endodontists.
https://www.aae.org/specialty/clinical-resources/guide-clinical-endodontics/
5.
Ricucci, D., & Siqueira, J. F. (2013). Endodontology: An Integrated Biological and Clinical View. Quintessence Publishing (IL).
6.
Bergenholtz, G., Hørsted-Bindslev, P., & Reit, C. (2013). Textbook of Endodontology. John Wiley & Sons.
7.
Beer, R., Baumann, M. A., & Kielbassa, A. M. (2004). Taschenatlas der Endodontie.




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io