Systemic Enamel Hypoplasia: Etiology, Classification, Clinical Presentation, and Treatment
Developmental Enamel Defects: Systemic Hypoplasia. Overview of the Etiology, Clinical Forms, Diagnosis, and Aesthetic Restoration Techniques for Teeth.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Condensing osteitis (focal sclerosing osteomyelitis, focal sclerosing osteitis) is a localized area of increased bone formation around the apex of the tooth root that forms in response to prolonged exposure to a bacterial irritant.
The development of condensing osteitis is thought to be due to a prolonged inflammatory process associated with the activity of low-virulent microflora in the root canal system of a tooth with irreversible pulpitis, pulp necrosis, or chronic apical periodontitis. In this condition, instead of resorption, osteoblasts are stimulated by growth factors/cytokines and trabecular or cancellous bone grows around the apex of the tooth root. It is more common in childhood and young adulthood in the mandibular premolars or molars, but can occur in any tooth.
Healing after endodontic treatment, remodeling of excess bone tissue to normal may occur.

The lesion is usually found around the root tips of the molar or premolar roots of the mandible.
The affected tooth may be observed in the affected tooth:
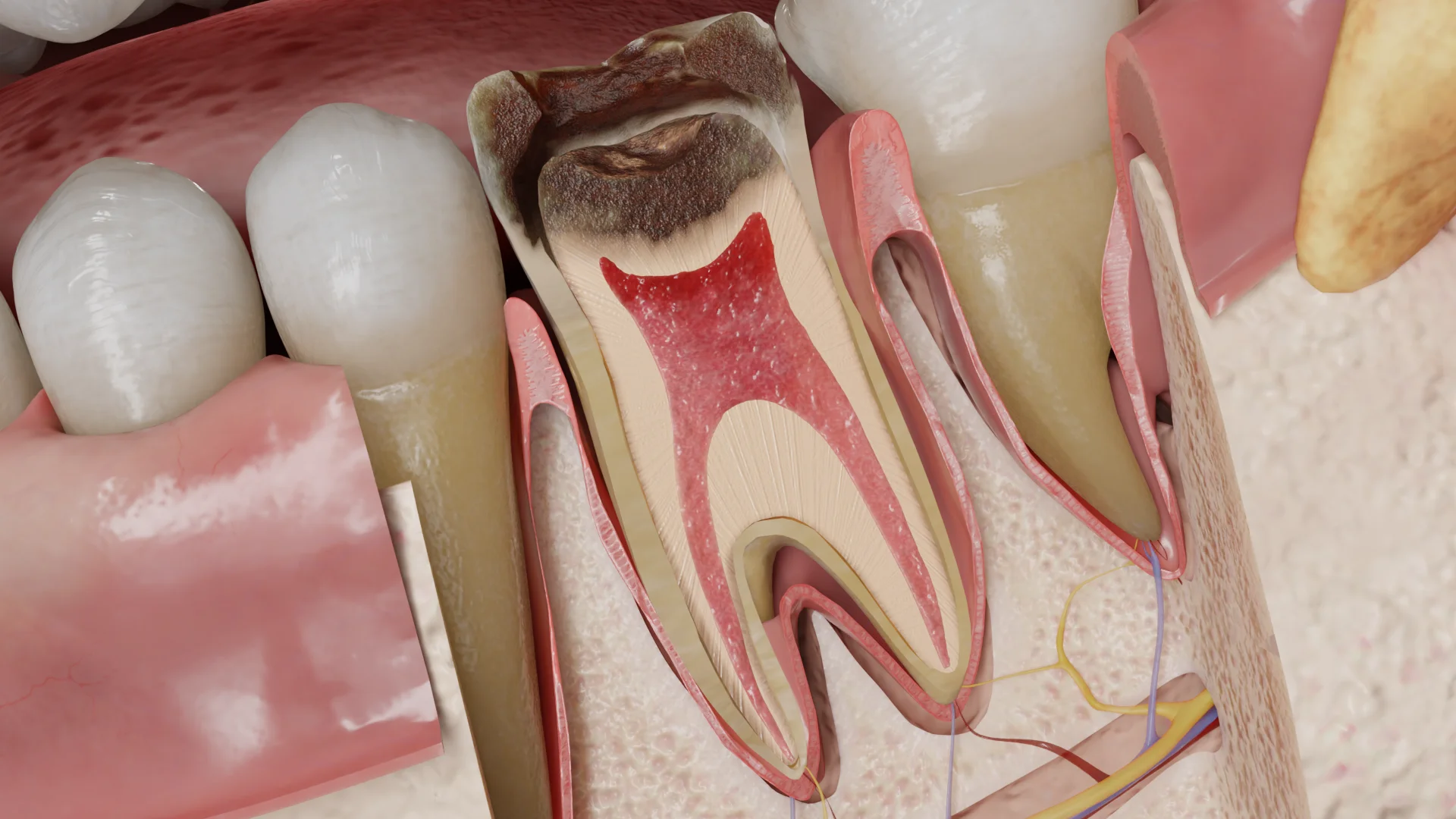
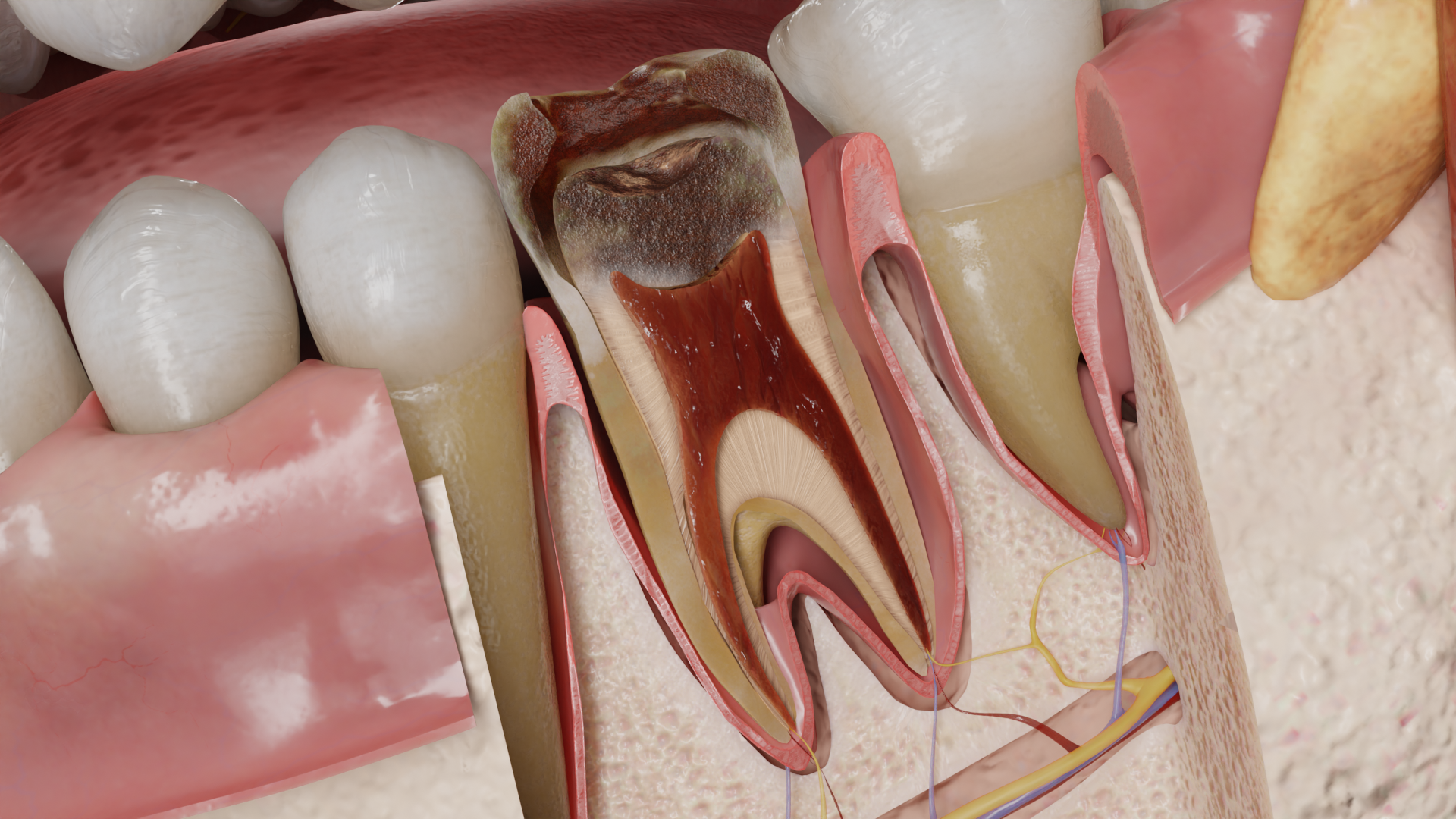
The pulp of the tooth is represented by whitish dense coarse-fibered scar tissue, or necrotic and has a yellowish-gray or gray-black color. The space of the periodontal ligament may be widened. In the periapical area there is a concentric deposition of bone substance infiltrated with a small number of lymphocytes, without bone destruction.
As the medullary spaces shrink and obliterate, the bone takes on the appearance of compact bone with reduced lacunae, many of which do not contain osteocytes.
The process is usually asymptomatic or the patient may present complaints characteristic of chronic irreversible pulpitis (prolonged pain due to thermal, chemical stimuli). Depending on the cause, a deep carious cavity, restoration or traumatic defect penetrating into the pulp chamber is visually identified in the tooth.
Percussion is usually painless, palpation of the transitional fold is painless. The thermal test may be positive in the presence of a vital pulp in a state of irreversible inflammation, or there may be no response to a thermal stimulus in the case of pulp necrosis. The causative tooth does not respond to the electrical stimulus or has a higher electrical stimulation threshold than healthy teeth.
Find more scientifically accurate content on our social media








Endodontic treatment of the tooth is carried out: pulp removal, instrumentation and medication of root canals, then their obturation with subsequent restoration of the tooth.
If the prognosis of endodontic treatment is unsatisfactory, the tooth should be extracted.
1. How is condensing osteitis diagnosed?
2. What causes condensing osteitis?
3. Is tooth extraction required for condensing osteitis?
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Berman, L. H., & Hargreaves, K. M. (2020). Cohen’s Pathways of the Pulp Expert Consult. Elsevier.
3.
Torabinejad, M., Fouad, A., & Shabahang, S. (2020). Endodontics: Principles and Practice. Elsevier.
4.
American Association of Endodontists. (2019, June 3). Guide to Clinical Endodontics – American Association of Endodontists.
https://www.aae.org/specialty/clinical-resources/guide-clinical-endodontics/
5.
Ricucci, D., & Siqueira, J. F. (2013). Endodontology: An Integrated Biological and Clinical View. Quintessence Publishing (IL).
6.
Bergenholtz, G., Hørsted-Bindslev, P., & Reit, C. (2013). Textbook of Endodontology. John Wiley & Sons.
7.
Hülsmann, M., Schäfer, E., Bargholz, C., & Barthel, C. (2009). Problems in endodontics: Etiology, Diagnosis and Treatment. Quintessence Publishing (IL).
8.
Beer, R., Baumann, M. A., & Kielbassa, A. M. (2004). Taschenatlas der Endodontie.
9.
Prabhu, S. R. (2021). Handbook of Oral Pathology and Oral Medicine. John Wiley & Sons.
Loading test 6 questions




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io