Systemic Enamel Hypoplasia: Etiology, Classification, Clinical Presentation, and Treatment
Developmental Enamel Defects: Systemic Hypoplasia. Overview of the Etiology, Clinical Forms, Diagnosis, and Aesthetic Restoration Techniques for Teeth.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
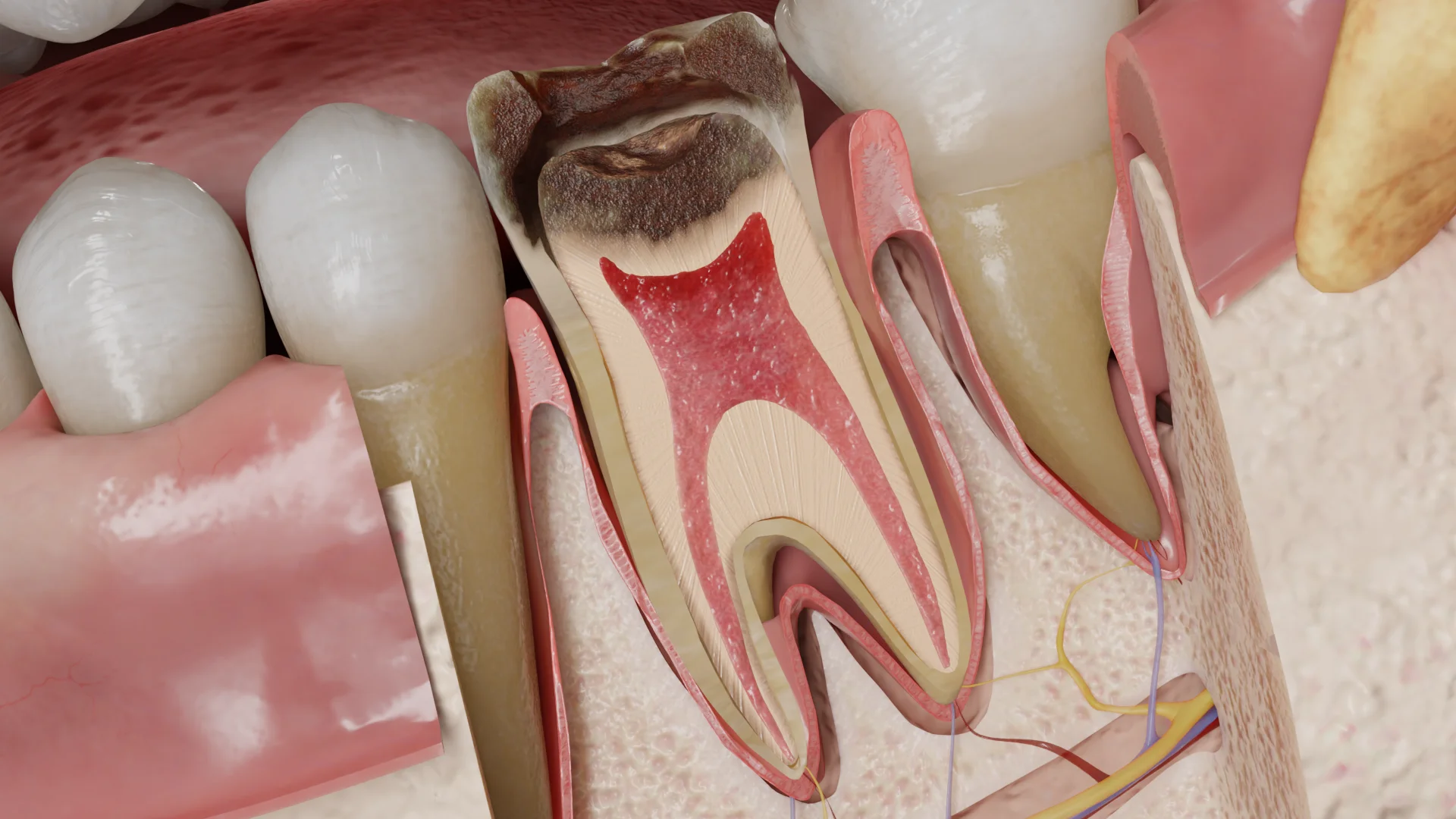
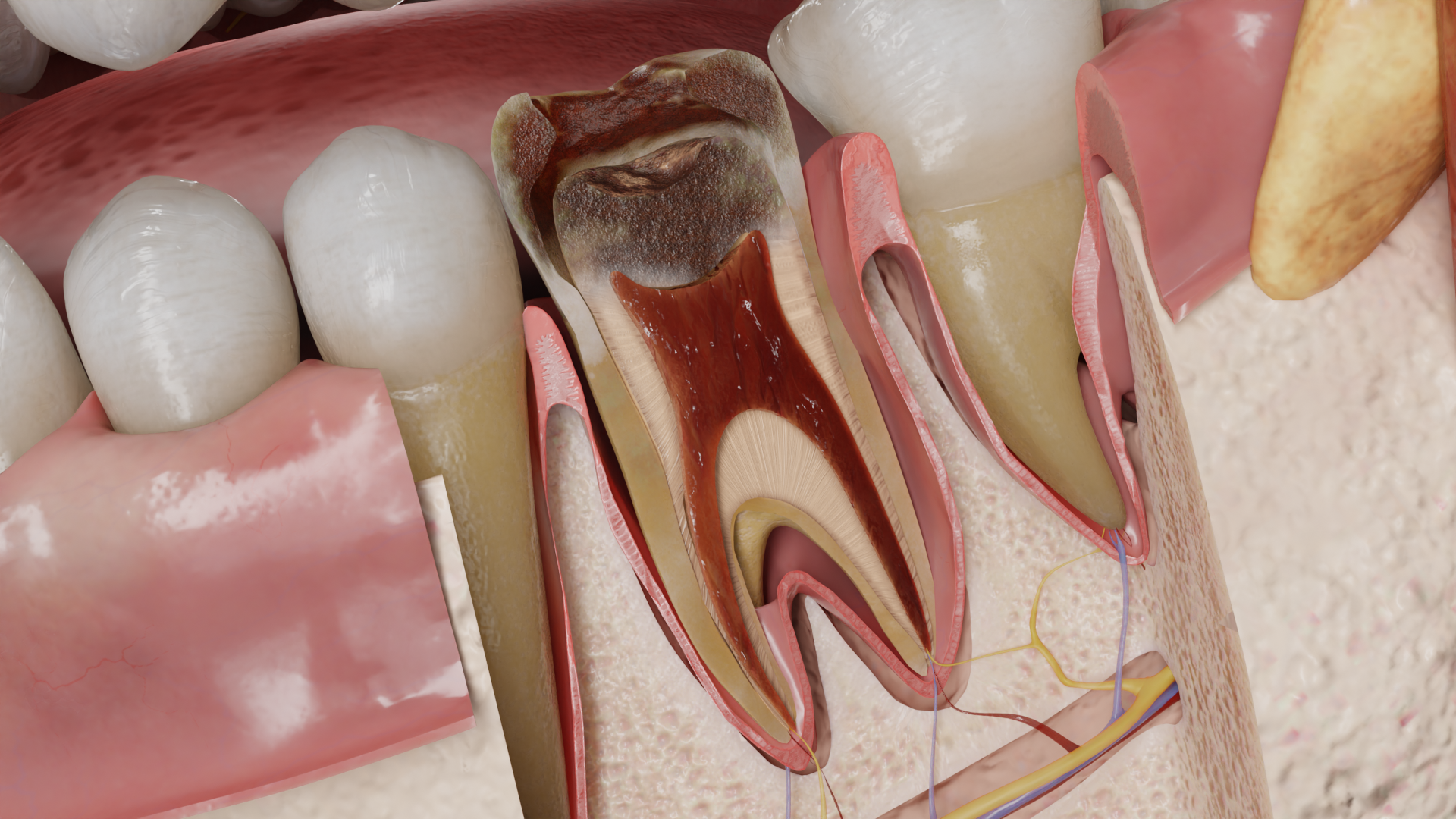
Apical granuloma, or periapical granuloma, is the most common form of chronic apical periodontitis (AP). It is an inflammatory lesion composed of granulomatous tissue rich in lymphocytes, macrophages, and plasma cells.
Chronic AP is a long-term inflammatory process affecting the tissues around the root apex of the tooth. This condition leads to periapical bone resorption, which has no significant clinical symptoms but is detectable on radiography.
Chronic inflammation in the periapical region is primarily triggered by a bacterial infection of the root canal system. In teeth that have not previously undergone endodontic treatment, AP serves as a protective response to the primary infection in the necrotic pulp. Another possible etiological factor is a secondary infection, introduced into the root canal system due to endodontic treatment (e.g., inadequate isolation during the procedure, improper obturation, or insufficient coronal sealing). Moreover, extrusion of chemical agents and root-filling materials beyond the apical foramen can lead to toxic tissue damage. Substances like talc, calcium salts, cellulose from paper points, or cotton fibers may promote the formation of a foreign body giant cell granuloma. Additionally, a foreign material in the periapical region may become a perfect substrate for a biofilm.
The necrotic pulp within the root canal system provides an ideal environment for bacterial colonization and functioning. Here, bacterial aggregates are enclosed in an extracellular matrix and organized into biofilms that attach to the walls of the root canals. In this form, microorganisms are protected from the host immune system, as defense mechanisms cannot function effectively within the poorly vascularized root canal. Furthermore, the biofilm structure makes bacteria more resistant to a variety of antibacterial agents. If the biofilm in the root canal is not eradicated or substantially disrupted, AP may become chronic as the pathogens will persist. Histologically, macrophages and lymphocytes are the primary and predominant cells in this process, with occasional foam and giant cells observed.
The hallmarks of chronic AP are bone resorption in the periapical region and proliferation of fibrovacular granulation tissue. The former process is triggered by activated osteoclasts, while the latter represents an attempt to repair tissues and limit the inflammatory process. It is worth mentioning that resorption may also affect apical fragments of the tooth root.
The possible outcomes of apical granuloma include:
– Healing of the periapical tissues following successful endodontic treatment;
– Progression to an acute or chronic apical abscess if the source of infection persists and the host immune response is compromised by exposure to bacterial infection.
Depending on the etiology, the following anatomical changes may be observed in the affected tooth:
This condition is characterized by necrotic pulp that appears yellowish-gray or grayish-black. At the root apex, there is a focus of destruction of the periodontal ligament and bone, filled with granulomatous tissue.
This tissue is infiltrated by mast cells, macrophages, lymphocytes, plasma cells, and occasionally polymorphonuclear leukocytes. In addition, multinucleated foreign body giant cells, foam cells, cholesterol crystals, and epithelial cells in the form of disorganized strands can be present. In the peripheral area, fibrous tissue is usually observed.

The condition is usually asymptomatic. On visual examination, a tooth with a deep carious lesion, restoration, or traumatic defect penetrating the pulp chamber is observed.
Percussion of the tooth is typically painless, as is the palpation of the mucobuccal fold. However, if the cortical plate is involved, palpation may cause discomfort. There is usually no response to thermal or electrical pulp testing. Gingival probing depth remains within normal limits (1–3 mm), and the tooth mobility is physiological.
Find more scientifically accurate content on our social media








Although it is impossible to make a differential diagnosis with other forms of apical periodontitis on the basis of radiography, and the histologic status is usually unknown, the treatment consists of eliminating the etiologic factor. Endodontic treatment of the tooth is performed: extirpation of necrotic pulp or removal of old filling material from the root canals, mechanical and medical treatment of root canals, obturation with subsequent restoration of the tooth.
If access to the source of infection is difficult, in addition to conservative endodontic treatment, microsurgical methods (periradicular curettage, resection of the root apex with retrograde filling, amputation of the tooth root), intentional replantation are used.
In cases where endodontic treatment may have unfavorable outcomes, tooth extraction is indicated.
1. What is an apical granuloma?
2. What are the main symptoms of an apical granuloma?
3. What is the treatment for an apical granuloma?
4. What complications may arise from an untreated apical granuloma?
List of Sources
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Berman, L. H., & Hargreaves, K. M. (2020). Cohen’s Pathways of the Pulp Expert Consult. Elsevier.
3.
Torabinejad, M., Fouad, A., & Shabahang, S. (2020). Endodontics: Principles and Practice. Elsevier.
4.
American Association of Endodontists. Guide to Clinical Endodontics – American Association of Endodontists [Internet]. American Association of Endodontists. 2019.
Available from: https://www.aae.org/specialty/clinical-resources/guide-clinical-endodontics/
5.
Ricucci, D., & Siqueira, J. F. (2013). Endodontology: An Integrated Biological and Clinical View. Quintessence Publishing (IL).
6.
Bergenholtz, G., Hørsted-Bindslev, P., & Reit, C. (2013). Textbook of Endodontology. John Wiley & Sons.
7.
Hülsmann, M., Schäfer, E., Bargholz, C., & Barthel, C. (2009). Problems in endodontics: Etiology, Diagnosis and Treatment. Quintessence Publishing (IL).
8.
Beer, R., Baumann, M. A., & Kielbassa, A. M. (2004). Taschenatlas der Endodontie.
9.
Petersson A, Axelsson S, Davidson T, Frisk F, Hakeberg M, Kvist T, Norlund A, Mejàre I, Portenier I, Sandberg H, Tranæus S, Bergenholtz G. Radiological diagnosis of periapical bone tissue lesions in endodontics: a systematic review. International Endodontic Journal [Internet]. 2012 Mar 19;45(9):783–801.
Available from: https://doi.org/10.1111/j.1365-2591.2012.02034.x




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io