Scalp Injuries: Etiology, Mechanisms of Traumatization, Pathogenesis, Clinical Picture, Treatment
Artur D.Neurosurgeon, MD
18 min read·August 13, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Scalp injuries are a pathological condition caused by the impact of mechanical factors on the soft tissues of the head, resulting in damage to the latter.
Scalp injuries are commonly categorized into:
Abrasions to the soft tissues of the head;
Soft tissue contusions to the head;
Soft tissue wounds to the head;
Subcutaneous hematomas of the soft tissues of the head.
Etiology and pathogenesis of scalp injury
Scalp injuries are directly related to the prevalence and causes of head injury in adult and pediatric populations. The most common causes of brain injury in children and adults are:
Falls from heights (including your own height);
Traffic accidents;
Facts of willful injury to health.
In the course of any of the above factors of trauma, there is mechanical traumatization of the soft tissues of the head. This is due to the peculiarities of the anatomical structure of this area:
Connection of skin, subcutaneous fat and tendon helmet by connective-tissue trabeculae;
The presence of abundant blood supply to the soft tissues of the area;
Location beneath the soft tissue of the rigid bones of the skull vault;
Fusion of the periosteum with the cranial sutures.
These features explain the high risks of forming open wounds in the soft tissues of the head, as well as the high risks of subcutaneous hematoma formation in this area.
From an epidemiologic perspective, scalp injuries account for about 50% of patients presenting for head injury to the emergency room of clinics.
Thus of all scalp injuries encountered when patients seek inpatient care, abrasions occur in 4% of patients, soft tissue contusions of the head occur in about 27% of patients, scalp wounds and subcutaneous hematomas of the head region occur in about 35% of patient cases.
Soft tissue injuries of the head, although they are prognostically favorable in terms of their course and potential full recovery of the patient, require close attention of doctors of all specialties, as they are associated with an increased risk of concomitant craniocerebral trauma.
Soft tissue contusions to the head
3D Animation: Soft Tissue Contusion to the Head
Contusion of soft tissues of the head – a pathological condition arising from traumatization of the soft tissues of the head without violation of the integrity of the skin and without damage to large vascular structures within the scalp.
Soft tissue contusion without concomitant head injury is characterized by the appearance of only local symptoms in the area of traumatization:
As a rule, no specific treatment is required for soft tissue contusions of the head.
Treatment of soft tissue contusions of the head
Treatment is provided symptomatically:
In order to limit bruising in this area, as well as to partially reduce the pain syndrome and swelling of soft tissues, it is recommended to apply cold to the site of injury for 5-10 minutes at intervals every 1 hour for 3-4 hours.
The use of nonsteroidal anti-inflammatory drugs with a pronounced pain syndrome in the area of impact.
Treat the bruise site with antiseptic solution, wash the bruise site if it is contaminated, and check the patient’s vaccination status for vaccination or revaccination with adsorbed pertussis-diphtheria-tetanus vaccine.
The outcomes of soft tissue contusions of the head are favorable, the patient does not need treatment in hospital conditions, complete healing of the contusion area is observed within 5-7 days.
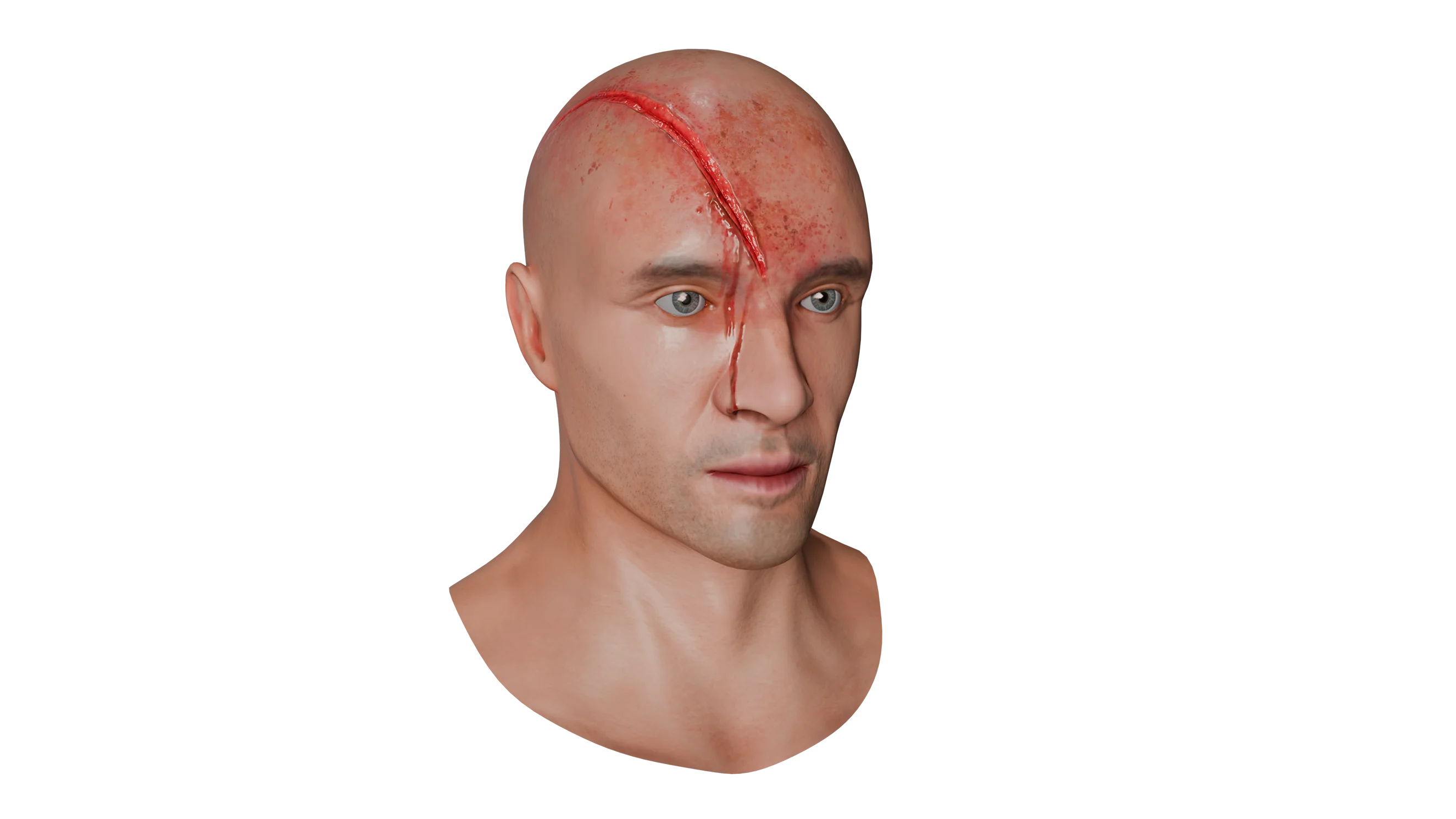
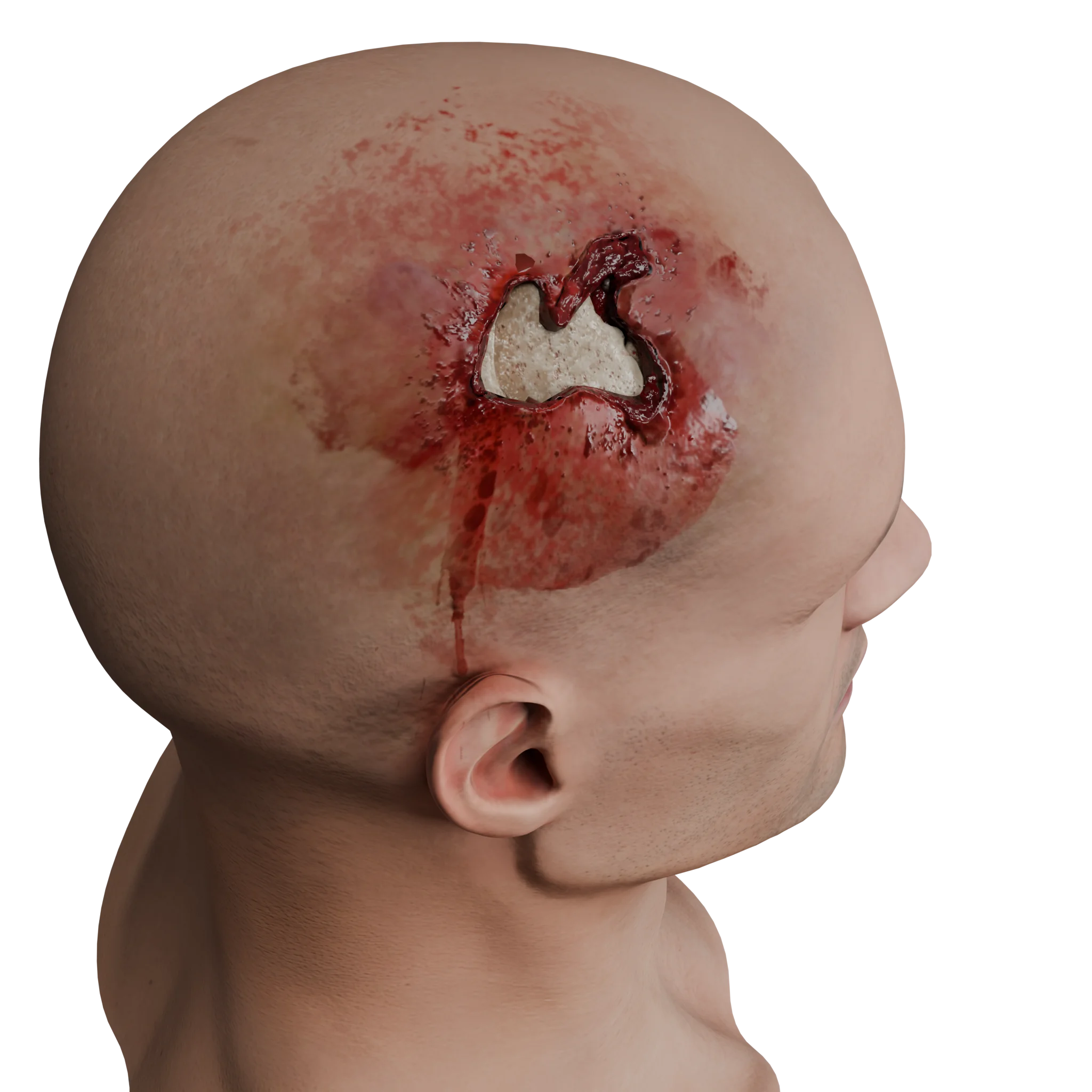
Head soft tissue wounds
3D Animation: Scalp Wound Without Aponeurosis Injury
Soft tissue wounds of the head region are a pathology characterized by damage to the skin, subcutaneous fatty tissue with or without damage to the aponeurotic helmet and underlying structures.
The peculiarities of the topographic anatomy of the head region, such as the presence of bridges in the subcutaneous fatty tissue, connecting the skin with the aponeurosis, as well as the location of the entire scalp on the bony base in the form of the skull vault, determine a high risk of wound formation.
The clinical picture of soft tissue wounds of the head is characterized by the presence of an area of skin damage with or without damage to the aponeurosis with signs of established or ongoing bleeding. Head soft tissue wounds with and without aponeurosis damage are presented in our 3D Models.
Due to the high blood supply to this area, one of the clinical manifestations of a bruised head wound is profuse bleeding from the damaged skin (in some cases, in case of untimely provision of assistance to the patient can lead to significant blood loss).
Diagnosis of soft tissue wounds of the head
Diagnosis and treatment of soft tissue wounds of the head include a comprehensive approach to determine the patient’s condition and exclude possible complications:
Clarification of the age and history of the injury, the presence of loss of consciousness after the injury, the presence of retrograde or antegrade amnesia after the injury;
Assessment of the level of consciousness according to the SCG, neurological examination of the patient in order to exclude intracranial injuries;
Examination of the site of contact with the traumatic agent, assessment of the presence of ongoing bleeding, wound revision followed by PCW or dressing with delayed PCW.
Exclude concomitant head injury, perform a CT scan of the brain.
Treatment of soft tissue wounds of the head
When caring for a patient with head wounds, attention should be paid to:
The length, depth, shape of the wound;
The presence of ongoing bleeding;
The presence of foreign bodies in the wound area;
The viability of the tissues that make up the wound edges.
Primary care
Stop the bleeding;
Extensive washing of the wound with antiseptic solution;
Revision of the wound in order to remove foreign bodies in their presence; Local infiltration of the wound area with adrenaline solution and local anesthetic for hemostasis.
Hemostasis is usually achieved by local infiltration of the wound area with adrenaline solution and local anesthetic. If bleeding is not stopped by this method, mechanical and thermal methods of hemostasis may be used.
Surgical treatment
After achieving hemostasis, removal of foreign bodies in the area and abundant washing of the wound with antiseptic solution, in the absence of signs of wound infection and early terms of its receipt (up to 24 hours), it is recommended to perform primary surgical treatment of the wound – economical excision of non-viable and infected tissues followed by one-stage suturing of the area.
If there are signs of primary infection of the wound, treatment is carried out in an open manner, daily dressings with the use of antibacterial solutions and ointments in order to completely clean the wound, followed by delayed suturing.
The method of wound closure is usually chosen by the surgeon. Strip suturing (if the wound size is less than 10 cm) and metal staples are preferred.
Nodal sutures can be used in case of severe bleeding for the purpose of mechanical hemostasis in the wound area.
Conservative treatment
Conservative treatment at the outpatient stage until the removal of sutures consists of monitoring wound healing, wound treatment with antiseptic solution and timely dressing.
If suppuration has joined the wound area, a BAK-sewing is required and antibiotic therapy is prescribed.
The suture material is removed from the wound after about 7-10 days in the absence of local complications at the outpatient stage of the patient’s treatment.
It is obligatory to check the vaccination status of the patient for vaccination or revaccination with adsorbed pertussis-diphtheria-tetanus vaccine. In the absence of vaccination, vaccination should be carried out in the emergency room of the hospital according to the instructions.
Forecast
Most head wounds have a favorable prognosis, do not leave pronounced cosmetic defects and are characterized by rapid healing.
Wound infections in this area are extremely rare due to the abundant blood supply to the skin in this area.
An aggravating factor in wound healing is the disruption of its blood supply and the presence of concomitant disease, leading to a decrease in the healing capacity of tissues.
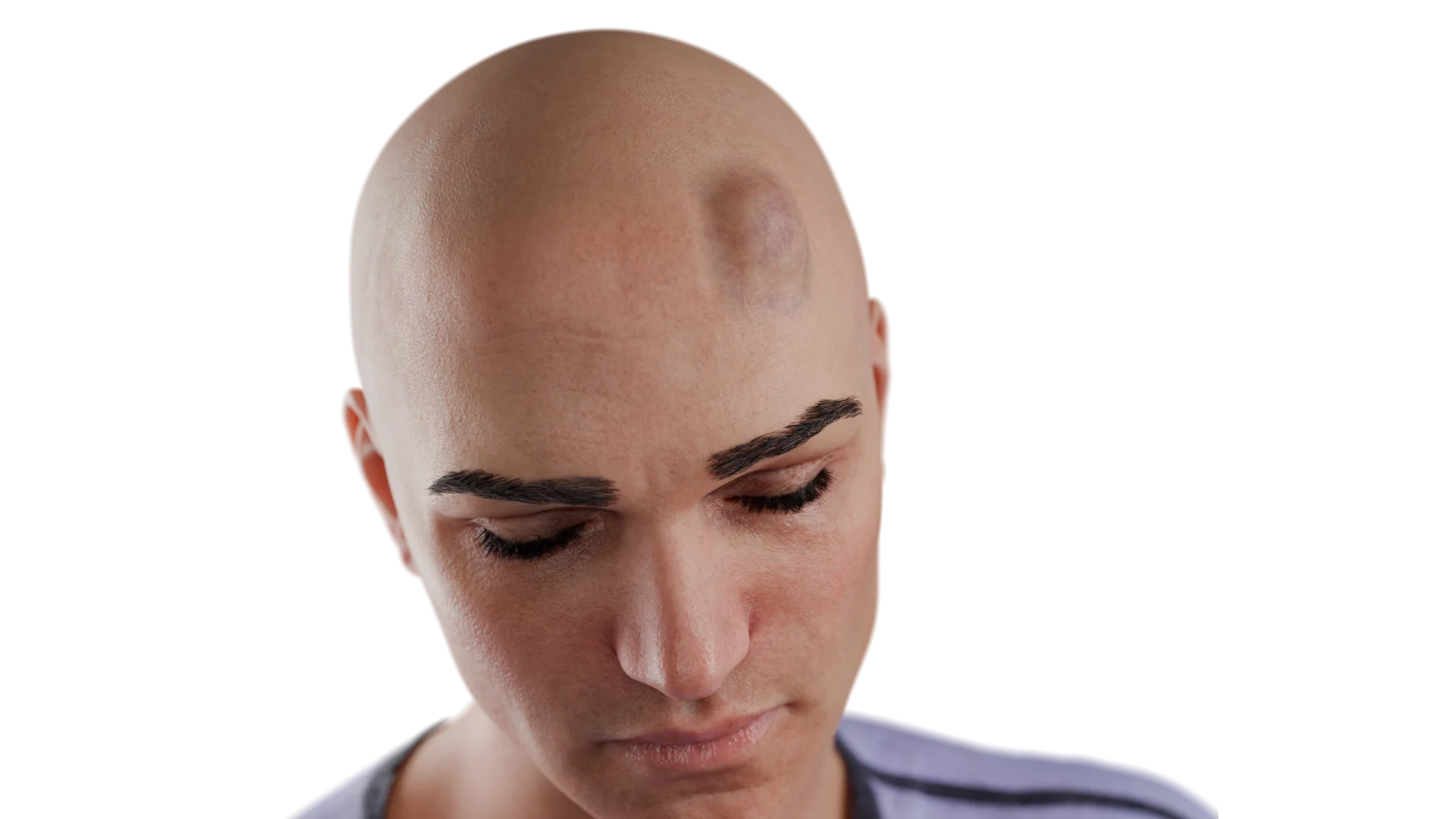
Subcutaneous hematoma of the soft tissues of the head
Subcutaneous hematoma of the soft tissues of the head is a pathology characterized by an accumulation of blood under the scalp due to damage to arterial vessels that supply blood to the scalp.
Subcutaneous hematomas can be either directly related to the presence of wounds in the area of their formation, or they can form without any visible injury to the scalp.
Subcutaneous Hematoma of Soft Tissues of the Head – 3D Model
The incidence of subcutaneous hematomas is 35 per 100 emergency patients presenting with various head injuries. The presence of scalp soft tissue hematoma is associated with an increased risk of head injury.
For example, some prospective studies report the following results:
In the absence of visible soft tissue injuries to the head, including subcutaneous hematomas, the risk of concomitant head injury is close to 0;
In the presence of a subcutaneous hematoma, especially >4 cm in size, the risk of concomitant craniocerebral injury increases to approximately 10%.
The etiological factors in the development of subcutaneous hematomas of the soft tissues of the head remain the most frequent causes of traumatization in craniocerebral trauma:
Falls from heights (including your own height);
Traffic accidents;
Intentional infliction of bodily harm.
Hematomas of this area, as a rule, have an uneven, well-defined shape, which is directly related to the anatomical features of the scalp mentioned above (the presence of bridges between the aponeurosis and the skin), which causes blood to flow beyond the area bounded by these trabeculae. Abundant blood supply contributes to the development of large hematomas.
The incidence of soft tissue hematomas is:
The frontal area is 46%;
Occipital area – 25%;
The dark area is 20%;
Temporal area – 8%.
The clinical presentation of hematomas of the soft tissues of the head includes swelling and edema in the area of contact with the traumatic agent, as well as pain in the area. In some cases, in the presence of massive hematomas, such as in the frontal or occipital region, the hematoma may spread to the para-orbital region or to the neck.
Diagnosis of soft tissue hematomas
Diagnosis of soft tissue hematomas of the head consists of:
Clarification of the age and history of injury, the presence of loss of consciousness after injury, and the presence of retrograde or antegrade amnesia after injury;
Assessment of the level of consciousness according to the SCG, neurological examination of the patient in order to exclude intracranial injuries;
Examination of the site of contact with the traumatic agent;
Performing soft tissue ultrasound when a tense hematoma is suspected;
Exclusion of concomitant head injury, CT scan of the brain.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Treatment of soft tissue hematomas of the head
Conservative treatment of soft tissue hematomas of the head is based on the reduction of local symptoms and relief of the patient’s condition:
Pressure dressing to the area of the hematoma;
Local hypothermia to the hematoma area for the first 24 hours;
Nonsteroidal anti-inflammatory drugs to control pain;
Routine administration of antibiotics for prophylactic purposes is not required. AB-therapy is prescribed only in case of signs of infection of the hematoma and should be prescribed after drainage of the focus of infection with subsequent adjustment after obtaining cultures for flora and sensitivity.
Surgical treatment is performed in the presence of tense hematomas of soft tissues of the head and is aimed primarily at opening the hematoma, evacuation of its contents, achieving hemostasis and leaving drainage in the cavity of the hematoma.
In the absence of vaccination with adsorbed pertussis-diphtheria-tetanus vaccine, vaccination in the emergency room of the hospital is required according to the instructions.
In most cases, soft tissue injuries of the head are not life-threatening, but are an important indicator of possible head injury in the patient. Neurological examination and instrumental diagnostics are mandatory in patients with this pathology if craniocerebral trauma is suspected.
FAQ
1. What is a soft tissue contusion of the head?
This is an injury to the soft tissues of the head in which there is no disruption of skin integrity or damage to major vessels. The main injury is rupture of small vessels, resulting in swelling, bruising and localized pain.
2. How is a contusion different from a wound or fracture?
In a contusion, there is no overt damage to the skin, nor is there a fracture of the bones of the skull.
3. What are the main symptoms of a head injury?
Redness, swelling, soreness on palpation, sometimes bruising. In isolated contusion there are no neurological symptoms.
4. Do I need a CT scan for a soft tissue contusion of the head?
A CT scan is not necessary if there are no signs of brain injury. However, if there is loss of consciousness, nausea, vomiting, amnesia, in the elderly, or in patients taking anticoagulants, a CT scan is mandatory to rule out intracranial injury.
5. When should a subcutaneous soft tissue hematoma be opened?
Indications for drainage of subcutaneous hematoma is its tense form, i.e. the presence of tissue tension over the hematoma, impaired sensitivity in this area, as well as signs of ongoing bleeding into the hematoma cavity.
6. How to treat a soft tissue contusion of the head?
In most cases, symptomatic therapy is sufficient: applying cold for 5-10 minutes every hour and a half in the first 3-4 hours, NSAIDs for pain, antiseptic treatment of the bruise area.
7. Is inpatient observation necessary for isolated soft tissue injuries to the head?
Inpatient observation is not required if the patient has no evidence of concomitant brain injury.
8. When should sutures be removed for soft tissue wounds of the head?
Due to the good blood supply to the head area, the wound heals quickly enough, and the sutures can be removed on 7-10 days in the absence of inflammatory changes in the wound area.
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Acar E., Yamanoğlu A. The Importance of Scalp Hematoma in Predicting Intracranial Injury in Elderly Patients with Minor Blunt Head Trauma // Haydarpasa Numune Medical Journal. – 2022. – Vol. 62, No. 1. – P. 59–64. – DOI: 10.14744/hnhj.2021.24471.
3.
Clinicopathological Characteristics of Traumatic Head Injury in Different Age Groups // Chinese Medical Journal. – 2018. – Vol. 131, No. 6. – P. 684–689. – PMID: 29533929.
4.
Head injury in the elderly – an overview for the physician // BMJ Open. – 2019. – Vol. 9, No. 2. – e024940. – DOI: 10.1136/bmjopen-2018-024940.
5.
The Frequency of Brain CT-Scan Findings in Patients with Mild Traumatic Brain Injury and Scalp Lacerations // Chinese Journal of Traumatology. – 2018. – Vol. 21, No. 5. – P. 278-281. – DOI: 10.1016/j.cjtee.2018.04.002.
Traumatic subgaleal hematoma drainage in an adolescent // Journal of Surgical Case Reports. – 2023. – No. 4. – Article ID: rjad092.
8.
American College of Surgeons. Best Practices Guidelines for the Management of Traumatic Brain Injury. – Chicago: ACS Trauma Quality Programs, 2024. – 140 p.
9.
Tintinalli J. E., Ma O. J., Yealy D. M., et al. Emergency Medicine: A Comprehensive Study Guide. – 9th ed. – New York: McGraw-Hill Education, 2020. – 2176 p.
10.
Adams R. D., Victor M., Ropper A. H. Principles of Neurology. – 11th ed. – New York: McGraw-Hill Education, 2020. – 1568 p.
11.
Clinical Practice Guidelines: Head Injury // Emergency Medicine Australasia. – 2021. – Vol. 33, No. 5. – P. 738–749.