Post-Infarction Left Ventricular Aneurysms: Etiology, Pathogenesis, Diagnosis, and Treatment
Oleg K.Cardiovascular surgeon, MD
19 min read·January 29, 2026
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
A post-infarction left ventricular (LV) aneurysm is a localized bulging of the LV wall, occurring after a myocardial infarction (MI) in the area of transmural necrosis and scarring. This condition is a serious complication affecting the contractile function of the heart and the patient’s survival prognosis.
Two fundamentally different types of damage are identified.
True LV aneurysm
The wall in this case is formed by all layers of the myocardium (scarred, thinned, but continuous myocardium).
The aneurysm cavity communicates with the LV cavity via a wide neck.
It has a low risk of rupture but leads to systolic dysfunction, arrhythmias, and thrombosis.
False aneurysm (pseudoaneurysm) of the LV
Occurs when the free wall of the LV ruptures. In such a case, the aneurysm wall is formed by pericardium/fibrous tissue, not myocardium.
Typically, it has a narrow neck and a sac-like cavity.
It has an extremely high risk of rupture and cardiac tamponade, thus it is considered a life-threatening condition usually requiring surgical intervention.
True (left) and false (right) left ventricular aneurysms: 3D model
Epidemiology
Thanks to early reperfusion, the incidence of LV aneurysm development has significantly decreased and is estimated at about 5–8% among patients with previous transmural MI.
False LV aneurysm occurs much less frequently — in about 0.2–0.5% of patients post-MI, often localized in the inferior and lateral walls. Despite its rarity, pseudoaneurysm is associated with high mortality due to the risk of sudden rupture (according to various retrospective studies, mortality without surgery can reach 80% in the first years of observation).
Epidemiology
Development of true LV aneurysm
Acute transmural myocardial infarction: necrosis of the entire myocardial layer, most often in the anterior descending artery territory.
Early remodeling phase: the necrotized wall becomes thinned, loses contractility, and develops akinesia or dyskinesia. Under the influence of intraluminal pressure, the section gradually bulges.
Fibrosis and scar formation: necrotic tissue is replaced by fibrous scar, which preserves wall integrity but poorly resists stretching.
Chronic remodeling and aneurysm: lead to stable, fixed bulging with a thinned, scarred wall and altered LV geometry, resulting in progressive systolic dysfunction, mitral regurgitation, and intracavitary thrombus formation.
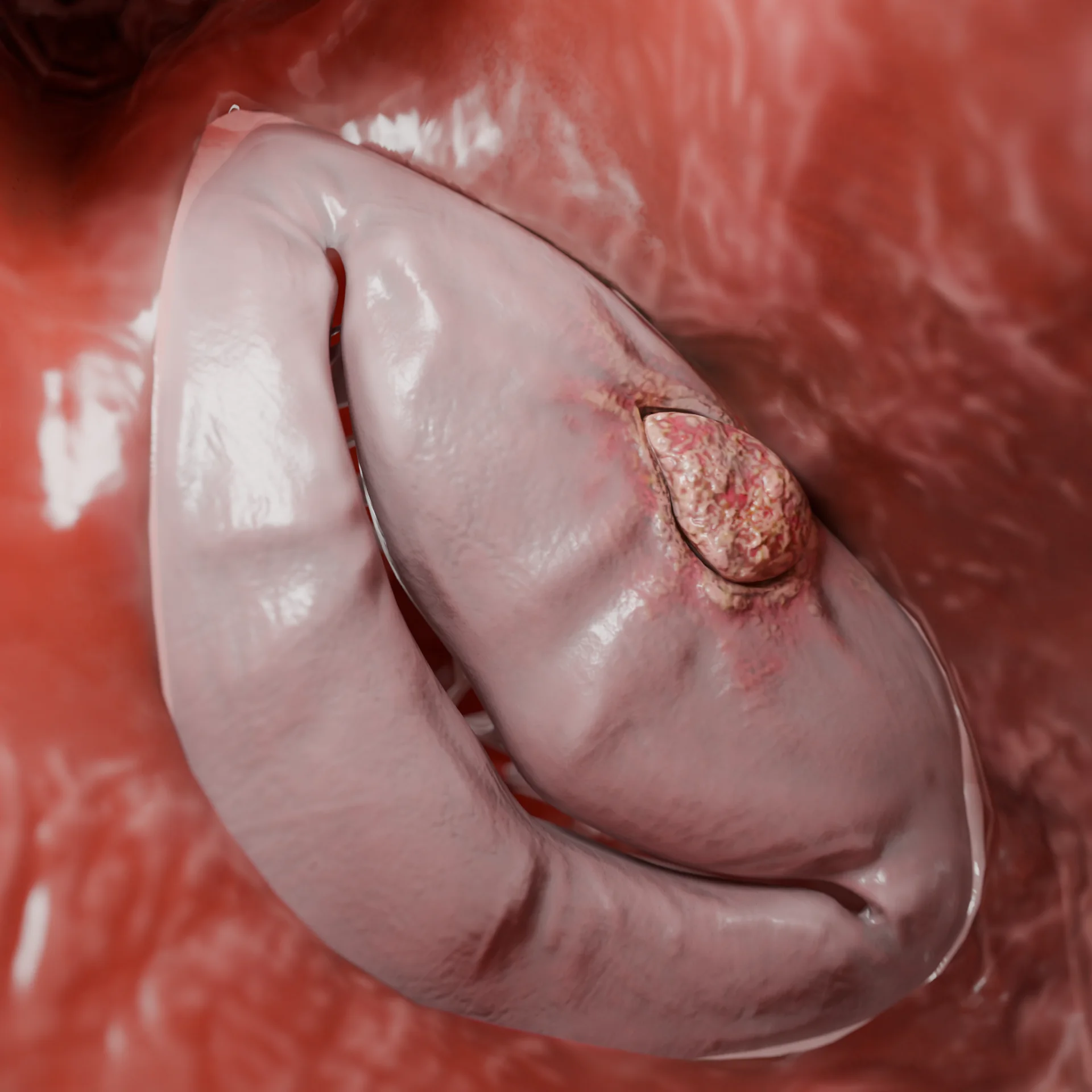
Thrombotic masses in the cavity of a true LV aneurysm: 3D model
Development of LV pseudoaneurysm
Rupture of the free LV wall: often occurs in the course of acute or subacute transmural MI. Sometimes rupture may appear as sluggish “leakage” of blood.
Pericardial restraint of rupture: blood from the LV cavity moves into the pericardial space but does not cause immediate tamponade due to local pericardial adhesions or clot formation.
Formation of pseudoaneurysm cavity: a cavity forms, typically communicating with the LV through a narrow opening. The wall is represented by the pericardium, fibrin, blood clots, and granulation tissue, without a full myocardial layer.
Progression and risk of rupture: the cavity can expand, increasing pressure and the risk of recurrent, potentially fatal rupture and tamponade. Additional possible complications include thromboembolisms, severe congestive heart failure, and arrhythmias. Upon final wall rupture, blood from the LV cavity bursts into the pericardium, causing acute tamponade and rapidly leading to death without immediate surgical intervention.
Classification
By wall structure
True aneurysm: the wall consists of a thinned, scar-altered myocardium (includes all layers of the wall).
False (pseudoaneurysm): occurs when the LV free wall ruptures, limited by the pericardium, blood clot, or scar tissue, with a lack of intact myocardial wall.
By time post-myocardial infarction
Acute: up to 2 weeks post-MI.
Subacute: weeks 2–6.
Chronic: more than 6–8 weeks post-MI.
By form of aneurysmal protrusion
Diffuse: broad base, with a gradual transition from the normal wall to the aneurysm zone.
Saccular: localized, more sharply demarcated bulging. Such a form more often raises suspicion towards pseudoaneurysm, especially with a markedly narrow neck.
True (left) and false (right) left ventricular aneurysms: 3D model
Clinical manifestations
Symptoms may range from no complaints to critical conditions.
True LV aneurysm:
Dyspnea and signs of chronic heart failure (CHF): a result of decreased contractility and LV systolic dysfunction.
Angina: occurs with persistent myocardial ischemia.
Arrhythmias: ventricular extrasystoles, stable or unstable ventricular tachycardia due to scar substrate.
Embolic complications: strokes, peripheral artery emboli in the presence of an intracardiac clot.
Asymptomatic course: in some patients, the aneurysm is detected asymptomatically during echocardiography or MRI.
False LV aneurysm:
Hidden symptoms: may present with mild symptoms or nonspecific complaints (dyspnea, weakness, atypical chest pain).
Often manifests with signs of heart failure, severe dyspnea.
Ventricular arrhythmias and thromboembolism may occur.
Fatal rupture: the main threat is sudden rupture leading to hemopericardium and cardiac tamponade, which may result in sudden collapse and death.
Diagnosis
Laboratory methods
There are no specific laboratory markers for LV aneurysm, but the following are used in practice:
Cardiospecific troponins, CK-MB: elevated in the acute phase of MI, helping to date the event.
BNP/NT-proBNP: reflects the severity of CHF and pressure/volume overload, often elevated in significant aneurysms.
Complete blood count, creatinine, electrolytes, coagulation profile, and other parameters are necessary for the assessment of comorbid conditions, surgical preparation, and anticoagulant therapy monitoring.
Instrumental methods
Echocardiography (transthoracic and transesophageal): a key method for primary diagnosis and differentiation of true and false aneurysms.
True aneurysm: localized thinning and bulging of the LV wall; broad opening between the LV cavity and aneurysm; dyskinesia/akinesia in the aneurysm zone; possible presence of mural thrombotic masses.
False aneurysm: narrow neck with a sudden transition from the LV cavity into the aneurysmal cavity; wall appears thin and heterogeneous, without a typical myocardial layer; pericardial effusion is often detected; a Doppler study reveals turbulent flow through the narrow opening.
Echocardiography: 1 — left ventricle, 2 — left atrium, 3 — false aneurysm (pseudoaneurysm)
Coronary angiography: it is conducted to assess the coronary bed, plan surgical intervention, and clarify ischemic etiology. Recommended before surgical correction of both true and false aneurysms.
Coronary angiography: critical stenosis of the anterior interventricular branch (1), occlusion of the circumflex branch (2)
Computed tomography (CT) and magnetic resonance imaging (MRI) of the heart.
Cardiac MRI: to evaluate the structure and function of the left ventricle, the thickness and composition of the wall, the volume and shape of the aneurysm, and the presence of blood clots. Allows for clear differentiation between a true aneurysm (scarred myocardium) and a pseudoaneurysm (wall without myocardium, limited by the pericardium).
Heart CT: an alternative to MRI; visualizes calcifications, pericardial changes, and the anatomy of the pseudoaneurysm neck.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Treatment for left ventricular aneurysm
Medication therapy
Aimed at treating the consequences of myocardial infarction and chronic heart failure, preventing thromboembolism and arrhythmias, and optimizing condition before/instead of surgery. The main groups of drugs are:
Antiplatelet therapy: aspirin and P2Y12 inhibitors are considered a standard therapy after myocardial infarction and stenting, in the absence of a high risk of bleeding.
Anticoagulants: vitamin K antagonists or non-vitamin K antagonist oral anticoagulants (NOACs) in the presence of intraventricular thrombus, at high risk of embolism, or large aneurysms with significant blood stasis, provided there is no high risk of bleeding.
Angiotensin-converting enzyme inhibitors (ACEIs)/angiotensin receptor blocker (ARBs)/angiotensin receptor-neprilysin inhibitors (ARNIs): reduce remodeling and improve prognosis in systolic dysfunction of LV.
Beta-blockers: reduce the risk of arrhythmias, decrease myocardial workload, and improve survival.
Mineralocorticoid receptor antagonists and SGLT2 inhibitors: in CHF with reduced ejection fraction, they represent a standard of modern therapy.
Diuretics: for control of symptoms of congestive CHF.
Antiarrhythmics therapy, implantable cardioverter-defibrillator (ICD): implantation of a cardioverter-defibrillator may be discussed for life-threatening ventricular arrhythmias.
Surgical therapy
True left ventricular aneurysm (indications):
Symptomatic CHF with severe systolic dysfunction of LV associated with aneurysmal deformation.
Refractory angina in the presence of significant coronary disease.
Life-threatening ventricular arrhythmias associated with the scarred area of the aneurysm.
Recurrent systemic embolism in the context of intraventricular clot, not controlled medically.
Main types of surgeries:
Resection of the aneurysm sac with reconstruction of the left ventricular cavity using a patch;
Linear aneurysmoplasty and other modifications;
Often combined with coronary artery bypass grafting (CABG) and/or mitral valve plasty (in cases of ischemic mitral regurgitation).
False pseudoaneurysm of LV (indications):
Due to the high likelihood of rupture, LV pseudoaneurysm is usually considered an absolute indication for surgical treatment, especially when identified in the first few months after MI and when the cavity size is >3 cm.
Main approaches:
Open surgical correction: suturing or closure of the pseudoaneurysm neck with a patch (pericardial or synthetic); reconstruction of the free wall of LV; simultaneous CABG if necessary.
Percutaneous closure: discussed in patients with high surgical risk and a well-defined pseudoaneurysm neck.
Conservative tactics (only medication and observation) are possible only in individual patients with chronic, stable, small pseudoaneurysms and high surgical risk, but they are associated with a significant risk of sudden death.
FAQ
1. How does a true left ventricular aneurysm differ from a false one?
The true one has a wall made of scarred myocardium and rarely ruptures. A false aneurysm (pseudoaneurysm) is formed when the LV wall ruptures and is held only by the pericardium; the risk of rupture is extremely high.
2. When are post-infarction aneurysms most commonly formed?
Usually 2–6 weeks after a transmural myocardial infarction.
3. What symptoms may indicate a left ventricular aneurysm?
Dyspnea, fatigue, signs of heart failure, chest pain, arrhythmias, or embolism. A false aneurysm may present as a sudden collapse.
4. What factors increase the risk of developing an aneurysm after a heart attack?
Large transmural infarction, a lack of access to timely percutaneous coronary intervention (PCI), recurrent myocardial infarction, and hypertension in the acute period.
5. What is the main diagnostic method for left ventricular aneurysms?
Echocardiography, supplemented by MRI/CT of the heart to clarify the thickness of the wall, the neck of the aneurysm, and the risk of rupture.
6. What laboratory indicators may be altered in left ventricular aneurysm?
Nonspecific: NT-proBNP (increasing), markers of HF; in the presence of clots, there may be signs of systemic embolization. No specific laboratory test is available.
7. When is surgical treatment required for left ventricular aneurysm?
In the case of symptomatic true aneurysm with heart failure or arrhythmias, in the presence of blood clots posing a risk of embolism, as well as in false aneurysm requiring urgent surgery due to high risk of rupture.
8. What types of surgery are used for true and false left ventricular aneurysms?
Aneurysmectomy, left ventricle reconstruction (Dor, Jatene), wall plasty, and blood clot removal. For a false aneurysm: closure of rupture and reinforcement of the wall.
9. Can development of left ventricular aneurysm be prevented after an infarction?
Yes. Timely reperfusion (PCI), strict pressure control, comprehensive therapy of MI and heart failure, and adherence to rehabilitation significantly reduce risk.
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Torchio, F., Garatti, A., Ronco, D., et al. (2022, May). Left ventricular pseudoaneurysm: The niche of post-infarction mechanical complications. Annals of Cardiothoracic Surgery, 11(3), 290–298. DOI: 10.21037/acs-2022-ami-25.
3.
El Ouazzani, J., & Jandou, I. (2022, February 24). Aneurysm and pseudoaneurysm of the left ventricle. Annals of Medicine and Surgery (London), 75, 103405. DOI: 10.1016/j.amsu.2022.103405.
4.
Damluji, A. A., van Diepen, S., Katz, J. N., et al. (2021, July 13). Mechanical complications of acute myocardial infarction: A scientific statement from the American Heart Association. Circulation, 144(2), e16–e35. DOI: 10.1161/CIR.0000000000000985.
5.
Lorusso, R., Matteucci, M., Lerakis, S., et al. (2024, May 14). Postmyocardial infarction ventricular aneurysm: JACC Focus Seminar 5/5. Journal of the American College of Cardiology, 83(19), 1917–1935. DOI: 10.1016/j.jacc.2024.02.044.
6.
Inayat, F., Ghani, A. R., Riaz, I., et al. (2018, August 2). Left ventricular pseudoaneurysm: An overview of diagnosis and management. Journal of Investigative Medicine High Impact Case Reports, 6, 2324709618792025. DOI: 10.1177/2324709618792025.
7.
Ruzza, A., Czer, L. S. C., Arabia, F., et al. (2017, October 1). Left ventricular reconstruction for postinfarction left ventricular aneurysm: Review of surgical techniques. Texas Heart Institute Journal, 44(5), 326–335. DOI: 10.14503/THIJ-16-6068.
8.
Kim, S. J., Kim, K. H., Kim, J. H, et al. (2024, October 1). Surgical repair of postinfarction left ventricular pseudoaneurysm. Texas Heart Institute Journal, 51(2), e248405. DOI: 10.14503/THIJ-24-8405.