The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
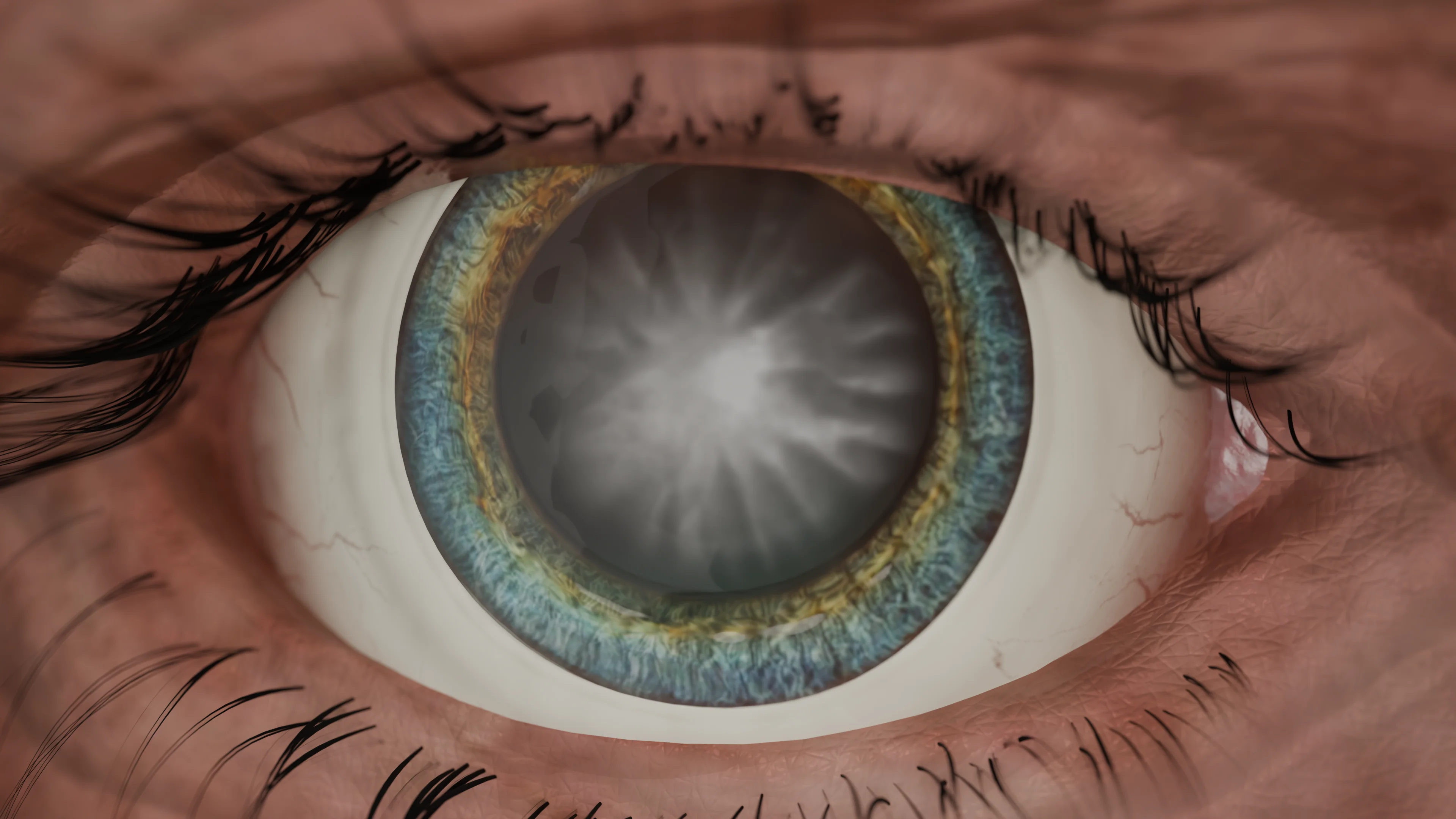
A pterygium is a pathological condition that affects the anterior segment of the eyeball. It is characterized by fibrovascular proliferation of wing-like, vascularized tissue that starts from the bulbar conjunctiva, crosses the corneoscleral junction (limbus), and extends to the adjacent cornea.
Etiology
Currently, long-term exposure to UV light, changes in lacrimal fluid, cytokine or growth factor imbalances, and p53 mutations are thought to be the major triggers for pterygia.
Anatomic Pathology
A pterygium consists of three parts — head, neck, and body. The head is the invasive part of a triangular-shaped formation, characterized by progressive growth. The neck connects the head to the body and covers the limbus; it is the narrowest part of a pterygium. The body is the broadest conjunctival portion of the pterygium, with its base directed toward the medial corner of the eye. Both early and late stages of the disease may present with an opaque surface of the cornea near the apex of a pterygium (halo).
The key pterygium feature is vessels that appear more dilated than other normal adjacent conjunctival vessels. The formation is typically semitransparent.
Pterygium Classification
The condition has 3 grades based on the length of a pterygium:
Grade 1: The initial stage, where the pterygium head is observed near the limbal cornea; visual function or refraction is not affected.
Grade 2: The pterygium head is located midway between the limbus and the projection of the external border of the normal pupil (3 mm). Irregular corneal astigmatism is observed directly in front of the pterygium head, while the central zone is characterized by minor regular astigmatism. Visual acuity typically remains unaffected.
Grade 3: The pterygium head is located on the cornea in the projection of the pupil diameter in daylight (3 mm), astigmatism may reach up to 13 diopters; visual function may be impaired due to the thickening of the corneal horizontal meridian.
One more pterygium classification is based on the likelihood of its proliferation:
1st degree: Episcleral vessels are clearly visible through the semitrasparent, atrophic membrane. Progression risks are low.
2nd degree: This is an active condition. Episcleral vessels are partly visible through the semitrasparent pterygium above the cornea.
3rd degree: An opaque, red, sarcotic pterygium proliferates promptly. Episcleral vessels are not visible for examination.
Pterygium Classification by Length and Likelihood of Proliferation
Classification
Description
By distribution relative to the cornea: Stage I
Pterygium head at the limbal zone of the cornea, without changes in vision and refraction
By distribution relative to the cornea: Stage II
Head at the middle between the limbus and the projection of the outer edge of the pupil (3 mm), irregular astigmatism in front of the head, in the center – correct weak astigmatism; vision is preserved
By distribution relative to the cornea: Stage III
Head in the projection of the pupil diameter (3 mm), astigmatism up to 13 diopters, decreased vision
By propensity to grow: 1st degree
Membrane translucent, atrophic, episcleral vessels clearly visible; risk of progression is low
By propensity to grow: 2nd degree
Pterygium translucent, episcleral vessels partially visible; active growth
By propensity to grow: 3rd degree
Pterygium fleshy, scarlet in color, episcleral vessels not visible; high risk of progression
Foreign body sensation, smarting eyes, burning sensations;
Eyeball hyperemia;
Increased light sensitivity (photophobia);
Decreased contrast sensitivity due to impaired corneal transparency.
Investigations:
Corrected visual acuity test;
Autorefractometry;
Keratometry;
Tonometry;
Optical coherence tomography (OCT) of the anterior segment of the eye.
Physical examination: Slit-lamp examination of the anterior segment of the eye.
Clinical Manifestations
The diagnosis is based on the following clinical manifestations:
Fibrovascular proliferation of the conjunctiva within the exposed palpebral fissure;
Involvement of the corneal surface;
A triangular or trapezoid-shaped membrane;
Proliferation starting from the nasal or temporal limbus;
A white or pink formation depending on the presence of vessels;
A pigmented epithelial line composed of iron deposits (Stocker’s line) adjacent to a pterygium, which is a marker of a chronic disease.
Pterygium Treatment
Pterygia may be treated both medically and surgically.
Surgical removal of pterygia should be carried out with caution due to the risk of relapse and other complications. The procedure is indicated if a pterygium has not responded to medical therapy, causes constant discomfort, obscures the visual axis, or leads to astigmatism-induced impairment of vision. It may also become too large or restrict ocular motility.
Medical Therapy
An inflamed pterygium may cause irritation, foreign body sensation, and tearing. Most of these symptoms may be relieved with over-the-counter eye drops containing high levels of dexpanthenol or hyaluronic acid. To reduce inflammation, short-term local corticosteroids may be used. These include 0.1 % dexpanthenol eye drops and 0.5 % hydrocortisone eye cream. However, long-term use is not recommended.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Surgical treatment
Currently, complete pterygium removal combined with conjunctival autografts is considered the industry gold standard, as the procedure is associated with a low relapse rate.
Excision with an amniotic membrane graft may be an alternative technique, but unlike a conjunctival autotransplant, the relapse rate is higher.
Simple excision with bare sclera or conjunctival closure has shown a relapse rate of up to 80 %, which makes it unacceptable.
Peripheral reconstructive lamellar keratoplasty (PALK) is an option in case of corneal opacity.
FAQ
1. Why is pterygium dangerous?
A pterygium poses a risk when it progresses. Key concerns include: Visual acuity reduction: As the growth extends, it induces astigmatism, which, in advanced cases, can reach up to 13 diopters. Optical obstruction: When the pterygium invades the corneal zone aligned with the pupil, it mechanically blocks the optical pathway, leading to permanent vision impairment. Chronic irritation: The expanding tissue causes persistent irritation of the eye’s surface, presenting as redness (hyperemia), a foreign body sensation, and light sensitivity (photophobia).
2. When should a pterygium be surgically treated?
Surgical intervention is recommended when specific indications arise, including a progressive growth reaching close to the pupil, which can give rise to severe astigmatism and significantly impact vision; persistent discomfort or inflammation that does not respond to conservative treatment; cosmetic concerns that cause psychological distress for the patient.
3. Should a pterygium be removed?
Not all cases of pterygia require surgical removal. An early-stage pterygium, when the growth is small and does not affect vision, may require regular follow-up and eye protection from UV exposure. However, when a pterygium progresses and causes visual impairment, or leads to persistent eye irritation, surgery becomes necessary. Modern surgical approaches, such as conjunctival autotransplantation, significantly reduce the risk of recurrence.
4. How long does it take to recover after pterygium removal?
The recovery time depends on the surgical method used. In standard removal with conjunctival grafting, complete healing takes approximately 2–4 weeks. Mild pain, conjunctival swelling, tearing, and light sensitivity may occur in the first few days. Visual acuity usually stabilizes within 1–2 months, especially in cases of severe astigmatism prior to surgery. Following the doctor’s recommendations is crucial to prevent relapses — using prescribed eye drops, avoiding direct sunlight, and wearing UV-protective glasses.
List of Sources
1.
Delic, N. C., Lyons, J. G., Di Girolamo, N. D., and Halliday, G. M. (2017). Damaging effects of ultraviolet radiation on the cornea. Photochem. Photobiol. 93, 920-929. doi: 10.1111/php.12686.
2.
Ting, D. S. J., Foo, V. H. X., Yang, L. W. Y., Sia, J. T., Ang, M., Lin, H. T., et al. (2021). Artificial intelligence for anterior segment diseases: emerging applications in ophthalmology. Br. J. Ophthalmol. 105, 158-168. doi: 10.1136/bjophthalmol-2019-315651.
3.
Zhou, Z., Wu, R., Yang, Y., and Li, J. (2018). Analysis of the relationship between corneal aberration and the size of pterygium. J. Clin. Ophthalmol. 4, 315-317.
4.
Droutsas K, Sekundo W (2010) Epidemiology of pterygium. A review. Ophthalmologe 107(6):511-516.
https://doi.org/10.1007/s00347-009-2101-3
5.
Kim SW, Park S, Im CY et al (2014) Prediction of mean corneal power change after pterygium excision. Cornea 33(2):148-153.
https://doi.org/10.1097/ICO.0000000000000036
6.
Maurizi, E. et al. Tara. A novel role for CRIM1 in the corneal response to UV and pterygium development. Exp. Eye Res. 179 (2019).
7.
Hu, Y., Atik, A., Qi, W. & Yuan, L. The association between primary pterygium and corneal endothelial cell density. Clin. Exp. Optom. 103, 778-781.

.webp)
.webp)
.webp)