



Ptosis (Blepharoptosis): Causes, Classification, Treatment
What is ptosis of the upper eyelid, or blepharoptosis? Learn more about the etiology (both congenital and neurogenic), severity, classification, and treatment options.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
A chalazion (translated from the Greek “chálaza”, meaning “small hailstone” or “small lump”) is a chronic, aseptic, lipogranulomatous inflammation caused by the obstruction of the meibomian gland’s outlets. The conditions can affect both the upper and lower eyelids.
Although the pathophysiology of chalazia is well known, the predisposing factors of this meibomian gland dysfunction are less well known. A chalazion results from obstruction of the meibomian gland duct.
The exact underlying cause of this obstruction remains unclear, but a number of key triggers stand out:
The meibomian glands are abundantly innervated, and their function is regulated by a complex array of substances, such as androgens, estrogens, progestins, retinoic acid, growth factors, and possibly neurotransmitters. Sex hormone levels are known to affect the structure of the lacrimal and meibomian glands, the conjunctiva, the lateral cells, the cornea, the anterior chamber, the iris, the ciliary body, the lens, the vitreous, and the retina.
Hormone therapy is also a risk factor for meibomian gland dysfunction and dry eye syndrome. Studies suggest that in vitro fertilization (IVF), coupled with powerful hormonal therapy at the stage of embryo implantation and sometimes even throughout the entire pregnancy, also affects the meibomian glands’ functioning.
IVF patients tend to develop meibomian gland dysfunction, meibomitis, styes, and chalazia, which often recur.
The incidence of chalazion in various medical literature studies varies from 0.2% to 0.7%.
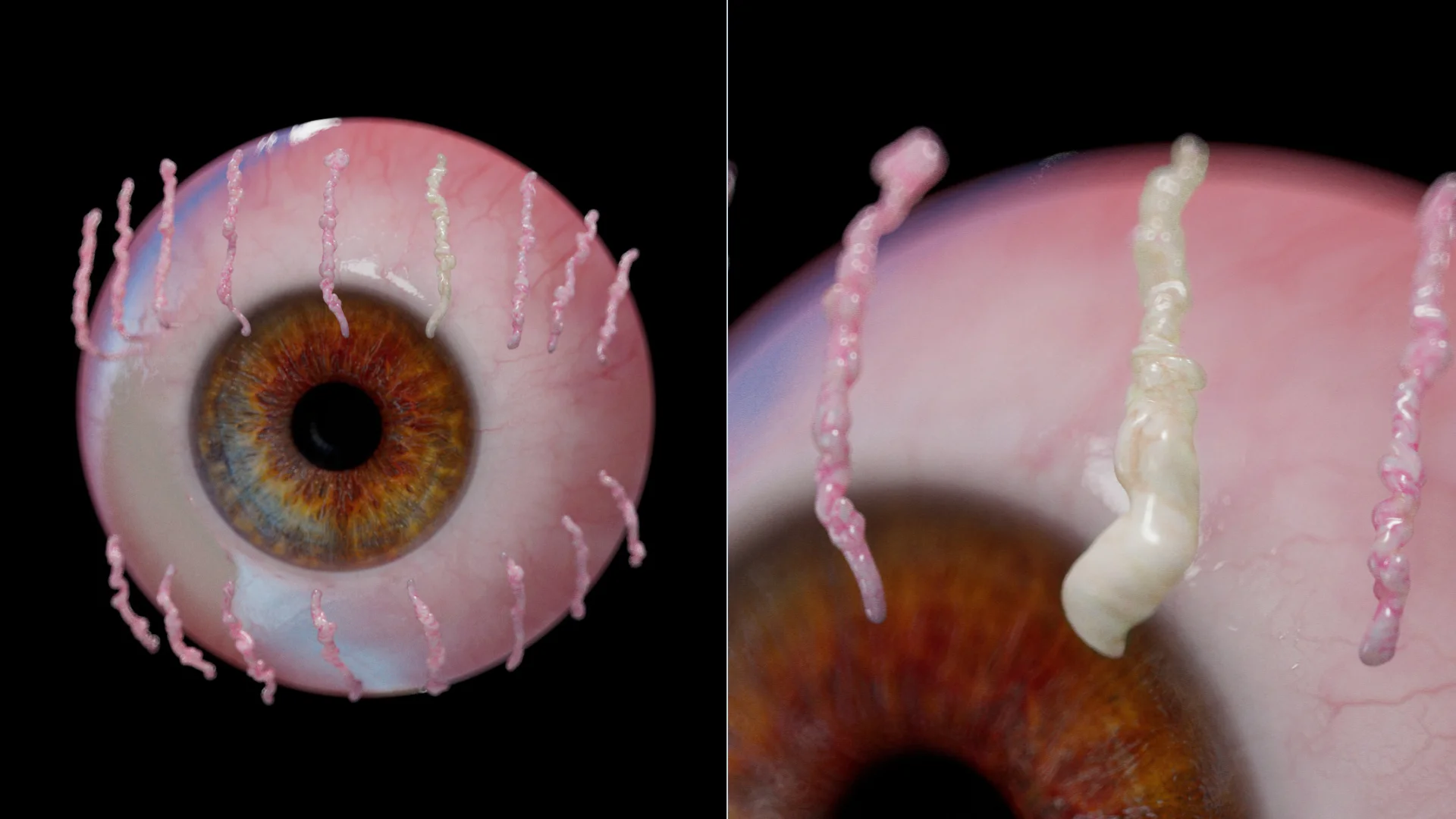
Meibomian glands usually produce an oily sebaceous secretion, which is distributed over the surface of the cornea and conjunctiva to keep them moist and prevent the ocular surface from drying.
Mechanism of development:
When a chalazion develops, patients most often complain about the formation of an elastic mass (“bump”) that creates a cosmetic defect and discomfort.
Main symptoms:
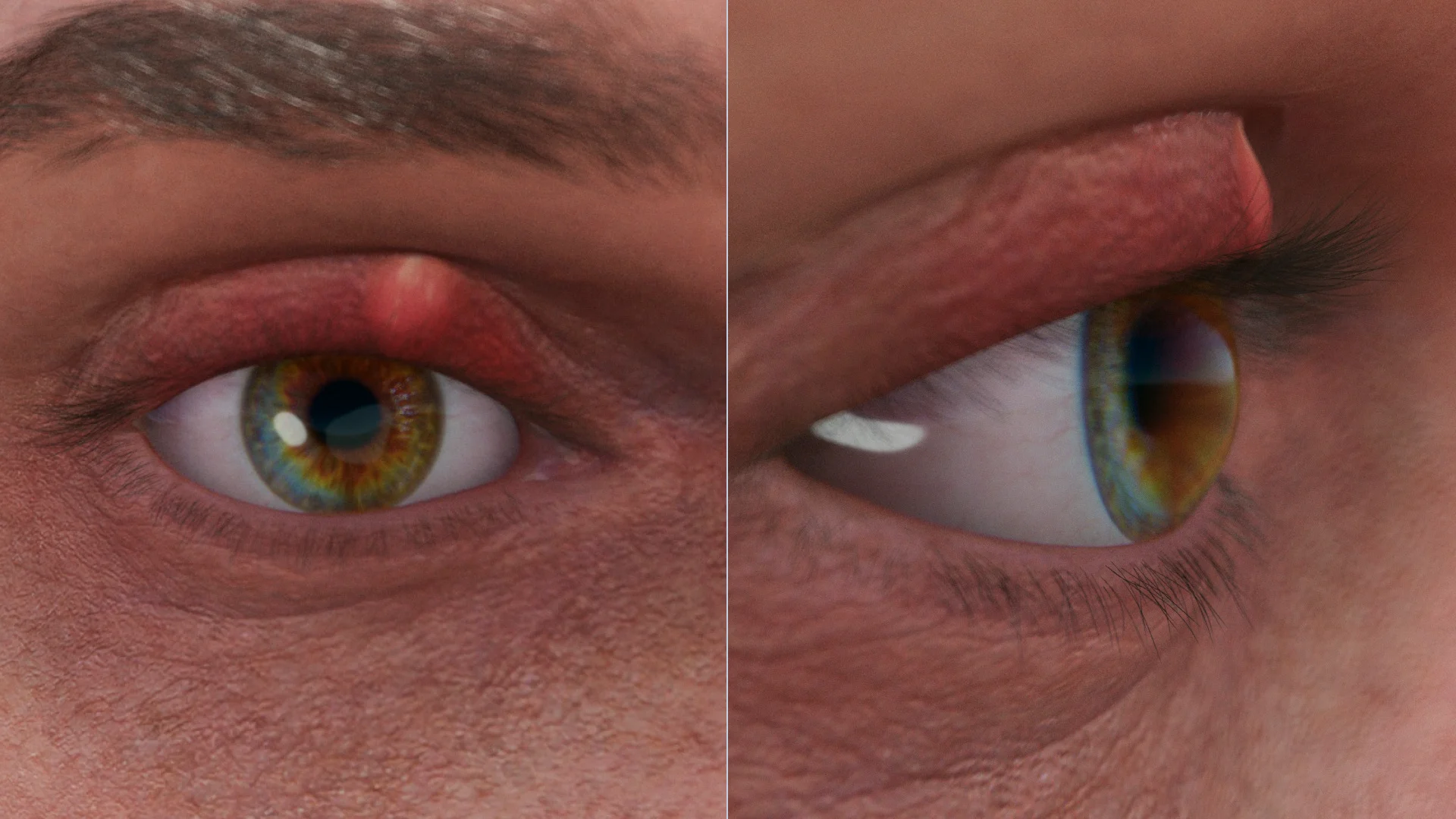
Diagnosis is made after physical examination. Comprehensive examination: biomicroscopy of the anterior segment, visometry, keratometry, tonometry, and echoscopy.
Picture during visual inspection (slit lamp):
Find more scientifically accurate content on our social media








In about a quarter of cases (25%), chalazia go untreated.
The first line of therapy for chalazia is non-surgical therapy.
If a chalazion is recurrent or when non-surgical treatment is ineffective, it may be necessary to inject corticosteroids (betamethasone) into the chalazion cavity.
The probability of success after a single injection is about 80%. A repeat injection can be given after 1-2 weeks.
Removal of the chalazion is performed if non-surgical methods fail or the formation is too large. Course of the procedure:
1. What is the difference between a chalazion and a stye?
2. Can a chalazion resolve on its own?
3. What should be done if a chalazion bursts (opens)?
4. Are chalazia contagious?
5. Is anesthesia administered during removal, and is it painful?
6. Why does a chalazion reappear (recur)?
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Devlioti D, Tsintarakis T, Milioti G, Seitz B, Kasmann-Kellner B. Unusual course of a chalazion. Ophthalmologe. 2015;112(3):269-71.
3.
Kumar J, Pathak AK, Verma A, Dwivedi S. Study of Incidence And Risk Factors of Chalazion in Bundelkhand Region. IOSR J Dent Med Sci. 2017;16(5):5-8.
4.
Sun M.T., Huang S., Huilgol S.C., Selva D. Eyelid lesions in general practice. Aust J Gen Pract. 2019 Aug;48(8):509–514.
5.
Manaa Alkatan H., Al‐Mohizea A., Alsuhaibani A. A case of localized amyloidosis of the eyelid misdiagnosed as recurrent chalazion. Saudi JOphthalmol. 2017 Jul‐ Sep;31(3):180–182. DOI: 10.1016/j.jcjo.2017.01.019.
6.
Трубилин В.Н., Полунина Е.Г., Анджелова Д.В., Евстигнеева Ю.В., Чиненова К.В. Влияние беременности на функциональное состояние мейбомиевых желез и сле‐ зопродукцию. Офтальмология. 2018;15(2):151–159. [Trubilin V.N., Poluninа E.G., Andzhelova D.V., Evstigneeva Y.V., Chinenova K.V. The Functional State of Meibomian Glands and Tear Production in Pregnant Women. Ophthalmology = Ophthalmology in Russia. 2018;15(2):151–159 (In Russ.)]. DOI: 10.18008/1816‐5095‐2018‐2‐151‐159.
Loading test 6 questions




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io
.webp)