




Chalazion: Etiology, Pathogenesis, Diagnosis and Treatment Methods
A Detailed Analysis of Chalazia of the Eyelid. Explore the Etiology, Pathogenesis, Clinical Presentation, Differential Diagnosis and Modern Treatment Protocols.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hematology
Hematopoiesis and blood-related disorders
Hepatology
Liver, gallbladder, and biliary tract diseases
Histology
Microscopic tissue and cell structures
Infectious diseases
Bacterial, viral, and parasitic infections
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Orthopedics
Bone, joint, and soft tissue disorders
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hematology
Hematopoiesis and blood-related disorders
Hepatology
Liver, gallbladder, and biliary tract diseases
Histology
Microscopic tissue and cell structures
Infectious diseases
Bacterial, viral, and parasitic infections
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Orthopedics
Bone, joint, and soft tissue disorders
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
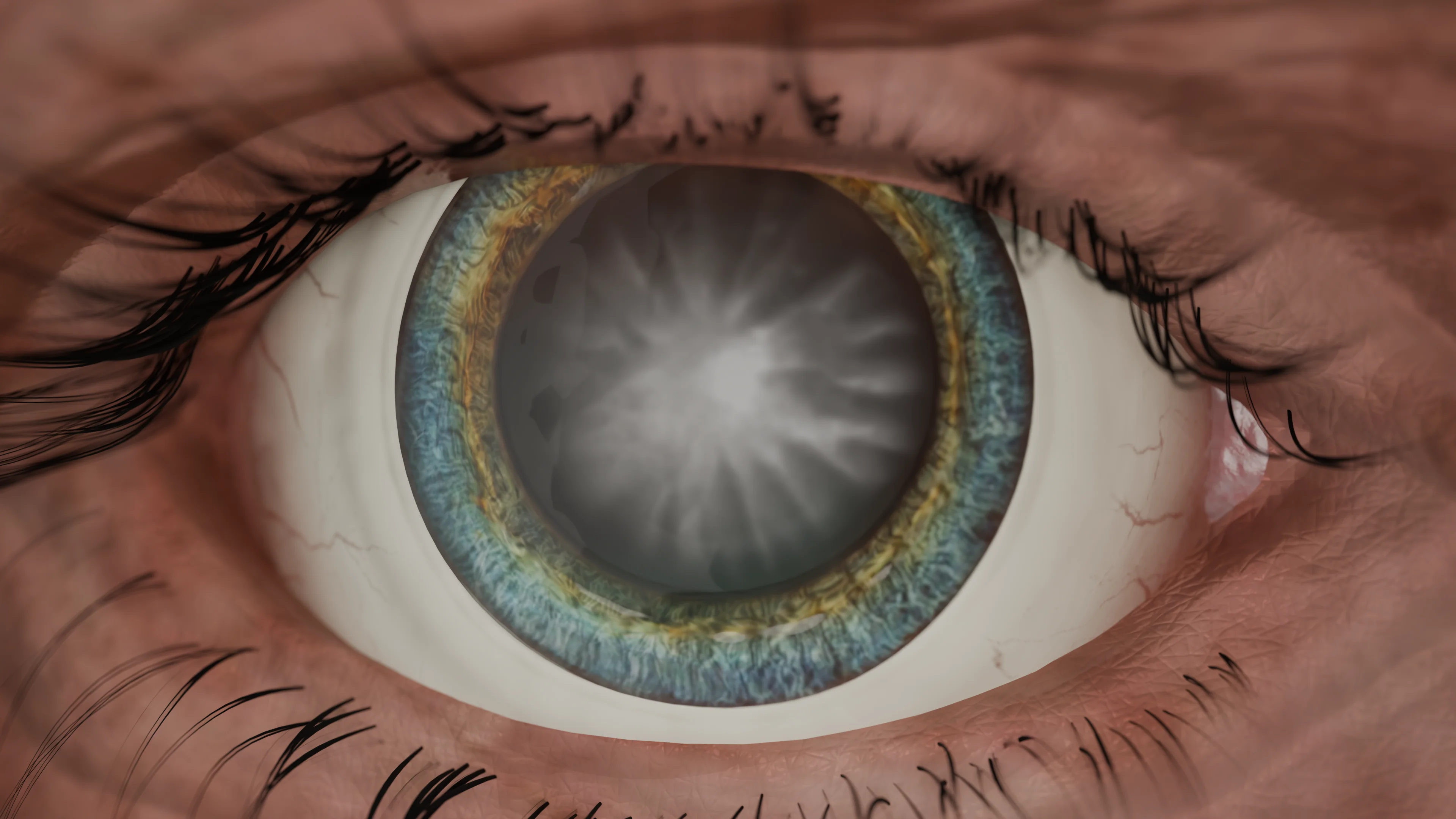
A cataract is a clouding of the natural lens of the eye, which is a component of the optical system of the eyeball. This pathology leads to a significant reduction in visual acuity and subsequently to the complete loss of visual functions.
The lens is a transparent, biconvex anatomical structure located between the iris and the vitreous body. The lens has the shape of a biconvex lens and comprises elastic tissue. Its diameter is approximately 9–10 millimeters.
The main part of the lens consists of transparent protein fibers that ensure its transparency and flexibility. The lens changes its shape due to the action of the ciliary muscles, allowing the eye to focus on objects at various distances. This is called accommodation. The lens must remain transparent so that light can pass through to the retina without distortion. Clouding of the lens, as in the case of cataracts, can lead to a decrease in visual acuity.
There are many factors contributing to the development of cataracts. They can be both congenital and acquired.
Depending on the localization of the opacities in the lens fibers, the following types can be distinguished:
According to the degree of maturity, the following forms of senile cataract are distinguished:
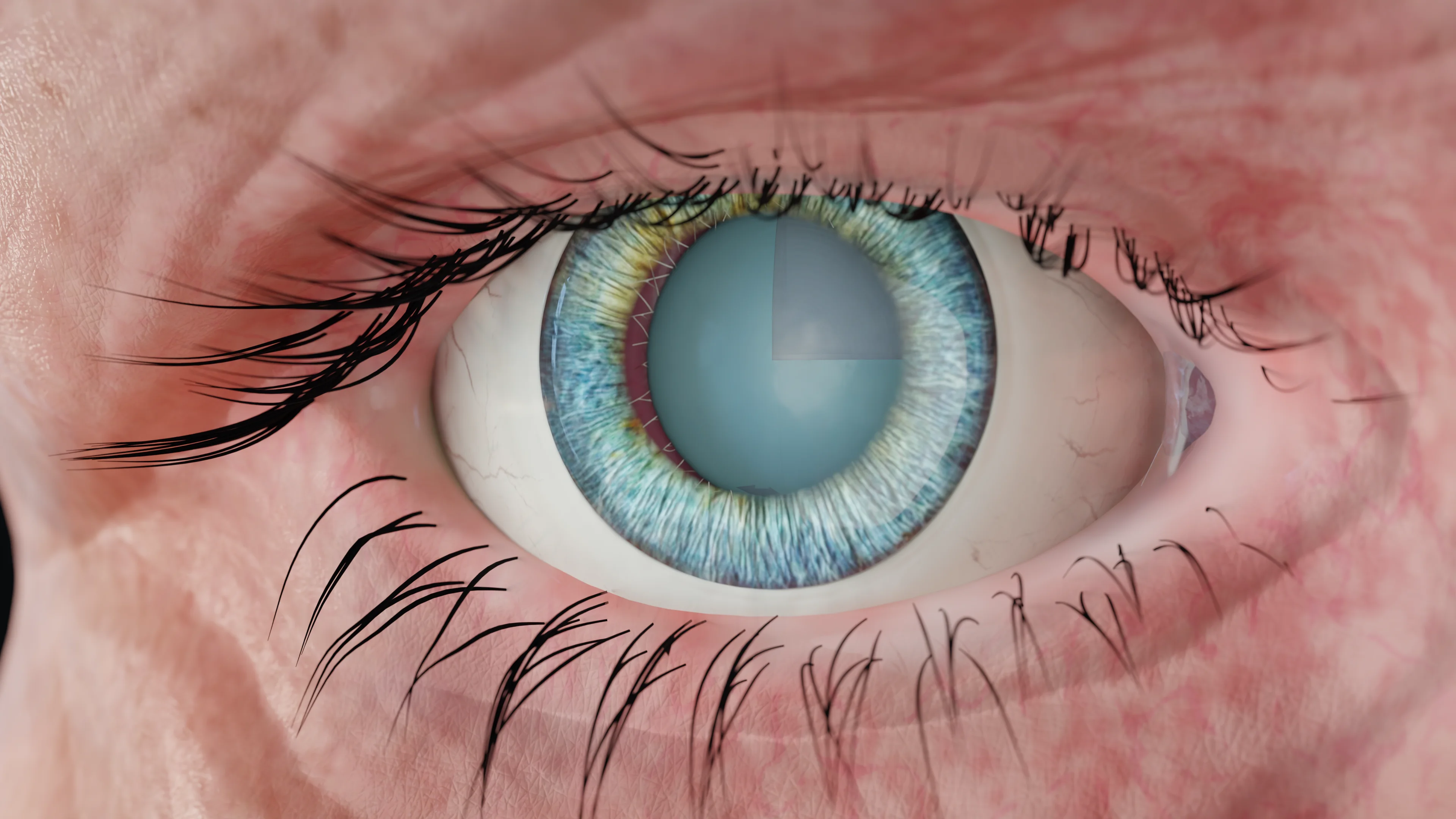
Cataract diagnosis is based on clinical examination and evaluation of symptoms. The main diagnostic criteria include:
Find more scientifically accurate content on our social media








Modern cataract treatment methods primarily focus on surgical intervention, as it is the only way to restore normal vision in this pathology.
Intracapsular artiphakia is a condition of the eye where an artificial intraocular lens (IOL) is implanted into the capsular bag in place of the removed lens, typically during cataract surgery.
Intraocular lenses help restore vision in patients with cataracts, as well as in patients with refractive errors (myopia, hypermetropia, astigmatism).
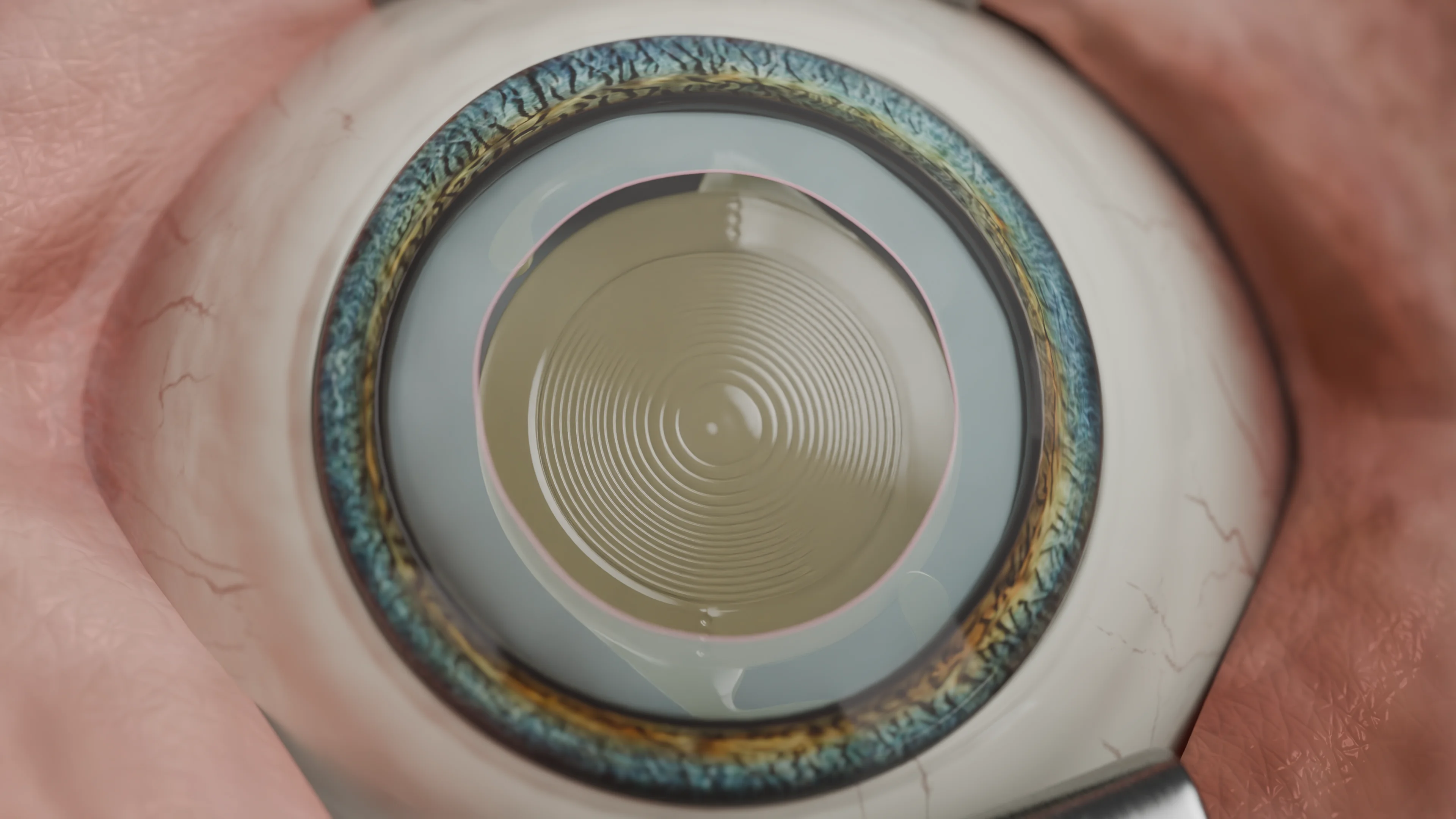
Cataract surgeries with the implantation of IOL in the posterior chamber of the eyeball are performed in patients of various ages, often under local anesthesia in outpatient settings. Thousands of lens replacement surgeries are performed worldwide every day.
IOL selection is based on the patient’s eye parameters (anterior-posterior axis [APA], corneal refractive power, and effective lens position), as well as the properties of the IOL, implantation features, and indications.
Aphakic intraocular lenses are implanted into the capsular bag after phacoemulsification.
The choice of aphakic IOL type depends on numerous factors:
Intraocular lenses are classified as follows based on the focus range:
According to a 2024 meta-analysis published in BMC Ophthalmology, multifocal IOL show good results in carefully selected patients, with satisfaction rates of 85-90%.
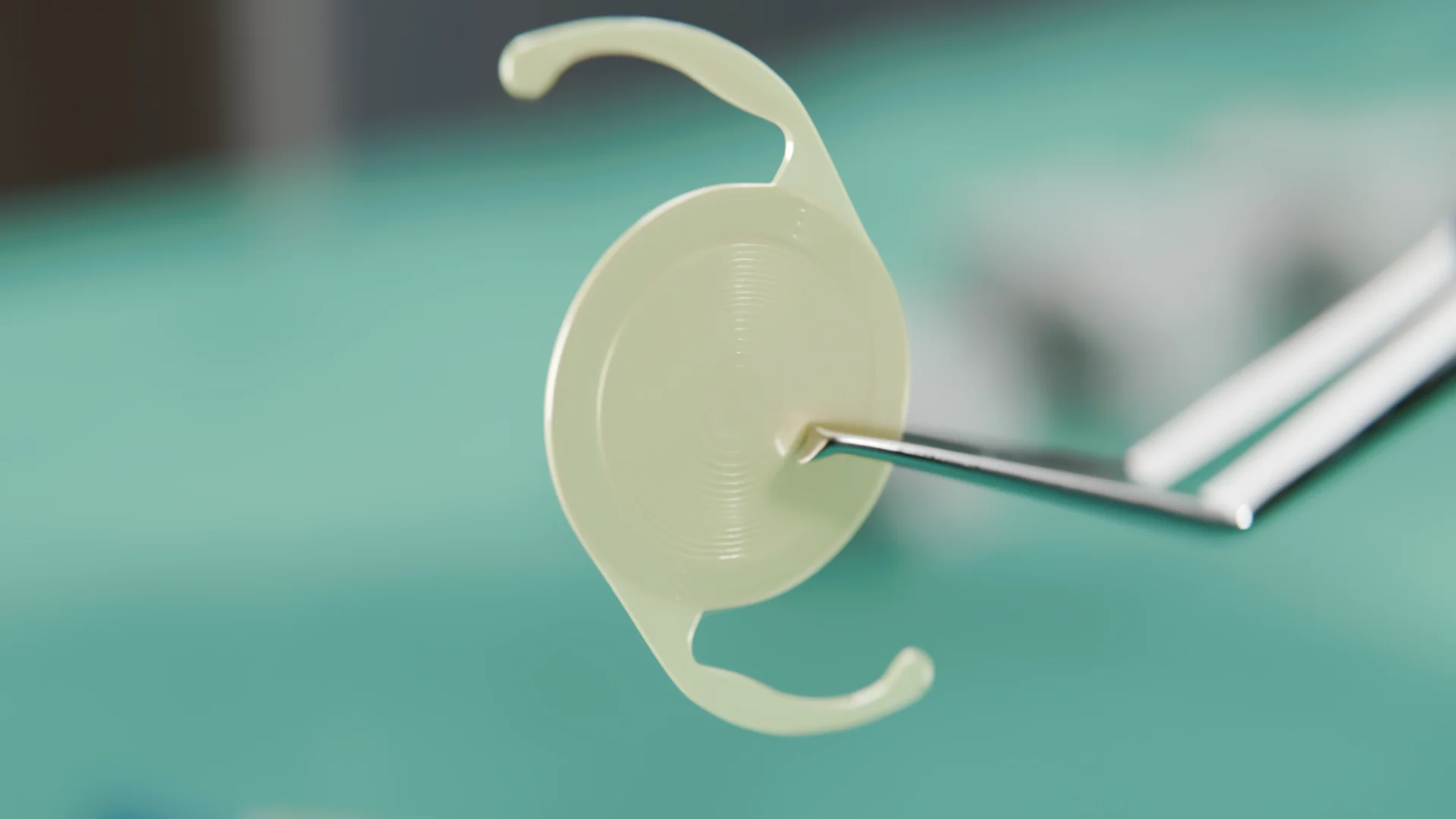
Modern intraocular lenses are made from high-tech biocompatible materials that are fully accepted by the body without risk of rejection or allergic reactions. The main materials used for IOL production are:
The primary function of an IOL is the precise focusing of light rays on the retina. The optical power of an IOL is measured in diopters and is selected individually for each patient based on detailed measurements of the eye’s anatomical parameters.
The working principle of an intraocular lens is based on the laws of light refraction. When light rays pass through the IOL, it alters their direction to focus precisely on the retina, creating a clear image.
An intraocular lens comprises optics and haptics. The haptic elements participate in the secure fixation of the IOL within the eye in anatomically and physiologically correct positions. The optical part is responsible for visual functions: it refracts and directs light rays onto the retina at the required angle. It can have multiple optical zones on its surface, allowing clear vision both near and far.
1. What is a cataract, and why is it dangerous if left untreated?
2. What clinical signs indicate the development of cataracts?
3. What is the fundamental difference between cataract and glaucoma?
4. Is there an option for conservative cataract treatment without surgery?
5. What is a secondary cataract, and how it can be cured?
6. At what stage of disease progression is surgery recommended?
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Pesudovs K, Lansingh VC, Kempen JH, et al. Cataract-related blindness and vision impairment in 2020 and trends over time in relation to VISION 2020: the Right to Sight: an analysis for the Global Burden of Disease Study. Invest Ophthalmol Vis Sci. 2021;62:3523.
3.
Global Burden of Disease 2019 Blindness and Vision Impairment Collaborators Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the Right to Sight: an analysis for the Global Burden of Disease Study Lancet Glob Health. 2021; 9:e144-e160.
4.
Alabdulwahhab KM. Senile Cataract in Patients with Diabetes with and Without Diabetic Retinopathy: A Community-Based Comparative Study. Journal of Epidemiology and Global Health [Internet]. 2021 Dec 7;12(1):56–63.
Available from: https://doi.org/10.1007/s44197-021-00020-6
5.
Rong X., He W., Zhu Q., Qian D. et al. Intraocular lens power calculation in eyes with extreme myopia: Comparison of Barrett Universal II, Haigis, and Olsen formulas. Journal of Cataract and Refractive Surgery. 2019;45(6):732–737. DOI: 10.1016/j.jcrs.2018.12.025.
6.
Jae Shin Song, Do Yeh Yoon, Joon Young Hyon, Hyun Sun Jeon. Comparison of Ocular Biometry and Refractive Outcomes Using IOL Master 500, IOL Master 700, and Lenstar LS900. Korean J Ophthalmol. 2020;34(2):126-132. DOI: 10.3341/kjo.2019.0102.
7.
IOL power calculation formulas: Haigis, Holladay, SRKT, Hoffer Q. East Valley Ophthalmology [Internet]. [cited 2021 Apr 10].
Available from: https://doctor-hill.com/iol-main/formulas.htm
8.
Karam M, Alkhowaiter N, Alkhabbaz A, Aldubaikhi A, Alsaif A, Shareef E, et al. Extended depth of focus versus trifocal for intraocular lens implantation: an updated systematic review and meta-analysis. Am J Ophthalmol. 2023 Jul;251:52-70. doi: 10.1016/j.ajo.2023.01.024.
Loading test 6 questions
Table of Contents




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io
.webp)